
Research Article | DOI: https://doi.org/10.31579/2637-8892/149
1 Simple Departmental Operational Unit of Clinical Psychology, Major Hospital of Lodi, Lodi, Italy.
*Corresponding Author: Ciro D’Auria, Simple Departmental Operational Unit of Clinical Psychology, Major Hospital of Lodi, Lodi, Italy.
Citation: Ivana Cacciatori, Chiara Grossi, Ciro D’Auria, Asia Bruneri, Silvia Rozza (2022) Newly Hired Health Workers during the Peak of COVID-19 show no Burnout: Resilience as a Protective Factor. Psychology and Mental Health Care, 6(2): DOI: 10.31579/2637-8892/149
Copyright: © 2022, Ciro D’Auria, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 04 October 2021 | Accepted: 28 December 2021 | Published: 21 January 2022
Keywords: COVID-19; burnout; resilience; healthcare workers; emotional exhaustion
Background: Burnout syndrome is a condition in which health workers pour out very frequently, especially due to the 2020 pandemic.
Aims: To deal with a possible risk of burnout due to the psychological and social pressure of the pandemic, it is good to have personal resources that work as a protective factor, such as resilience. The objective of this study is to investigate the differences between a sample of new hospital hires in 2019 and a sample of new hospital hires in 2020, in Lodi, Italy.
Methods: To fulfill these purposes, a burnout test and a resilience test were used, and a dummy variable representing the condition of COVID-19 was created.
Results: The results indicate that COVID-19 did not significantly affect burnout in the two samples.
Limitations: Since the tests were carried out on hiring, the operators may not have been conditioned by the work weight, although Lodi was the epicenter of the pandemic in Italy.
Conclusions: These data suggest that newly hired health workers would measure their work stress on personal resilience rather than the danger of COVID-19, despite government restrictions such as lockdowns, the mandatory use of safety devices, media reports on deaths and the risk of contagion.
Since December 2019, when the first cases of human infections from coronavirus (SARS-CoV-2) (Jin et al., 2020) appeared, the emergent infective illness (now called COVID-19) rapidly spread all over the world, infecting people in more than 219 countries (World Health Organization, 2020).
In March 2020 the infection of COVID-19 has been declared pandemic, due to the invasive epidemic spreading uncontrollably (World Health Organization, 2020).
COVID-19 has arisen an emergency state in public health that has no antecedents in modern history and that causes serious psychological and health problems in general population, including high levels of anxiety, depression, stress, fear, frustration and burnout (Ornell et al., 2020; Arslan et al., 2020; Brooks et al., 2020).
On November 7th there were more than 49,106,931 confirmed cases of infection and 1,239,157 deaths for COVID-19 (World Health Organization, 2020). Such alarming data created uncertainty about how we’ll defeat the virus and the effectiveness of protective devices (such as face masks and social distancing) and the application of preventive measures, like lockdown measures, curfew and the closure of specific commercial activities, resulted in increasing the potential for higher levels of mental health problems and psychological disorders (Talaee et al., 2020). In addition, living stressful conditions, like those that characterized the above-mentioned 2020 period, can take along many adverse effects on mental health and on psychological functioning, and can lead to mental confusion, social deprivation and severe mood disorders (Yildirim & Arslan, 2020).
According to some sources (Medscape, 2020), the 10% of all COVID-19 cases are healthcare professionals. These people had been exposed to long shifts, trying to respond to the increasing demand of health cares (Huang et al., 2020; Ornell et al., 2020). At the beginning of the diffusion of the virus, hospitals had to face limited availability of personal protective devices and a lack of established procedures and guidance (Xiang et al., 2020). Therefore, many health professionals felt confused and unprepared to treat properly patients infected with the new virus (Huang et al., 2020). This situation of uncertainty, characterized by lack of help, alienation, isolation and difficulty in managing workload, made health professionals feel lonely and perceive the stigma for their conditions and the weight of high expectations, with the possibility to lead them to severe psychological and emotional consequences, such as anger, insomnia (Ran et al., 2020; Zhang et al., 2020), up to burnout (Ornell et al., 2020).
Burnout syndrome is a state of physical, emotional and mental exhaustion, due to the exposure to stressing factors or emotionally requiring situations at work (Kristensen et al., 2005; Maslach & Leiter, 2008; McVicar, 2003). The first conceptualizations of burnout as a kind of illness comes from the difference between resources and demands (Cherniss, 1980). Maslach (1982) explained burnout as a reaction to the emotional distress determined by a continuous and direct contact with other human beings, expecially if they are suffering. Burnout may have an adverse effect on organizations and individuals, such as turnover, truancy, sick leave, injuries and accidents, low productivity and interpersonal and organisational conflicts (Ruotsalainen et al., 2015).
Health workers are exposed to high risk of developing burnout because of implicit requests and due to the stress in taking care of patients, due to long and solitary shifts and to the stressing environment (Kristensen et al., 2005; Ruotsalainen et al., 2015).
Health professional’s burnout is one of the emerging challenges that healthcare systems all over the world need to face with and includes protecting and safeguarding patients. Health professionals, as a consequence of burnout, may develop symptoms such as anxiety, irritability, moodiness, insomnia, depression, post-traumatic stress disorder, suicidal thoughts and feelings of failure (Kozak et al., 2013; Hämmig et al., 2012; McVicar, 2003; Reinhard et al., 2015; Shanafelt et al., 2011). Burnout consequences can be psychosomatics, including impairments like headaches, high blood pressure, cardiopulmonary diseases, musculoskeletal and gastric disorders, stomach ulcers, insomnia and fatigue (Maslach, 2001). Finally, symptoms may lead to a lower performance at work and to a poor care for the patient. Many reviews had noticed the prevalence and the determinants for burnout in health workers from the most developed and westernized countries, from North America, to Europe, to Australia (Bennett et al., 2005; Ramirez et al., 1996; Aiken et al., 2012; Bakker et al., 2000; Arigoni et al., 2009; Goehring et al., 2005), and in arabic countries too (Elbarazi et al., 2017).
Some researches repeatedly show high levels of burnout in nurses (Aiken et al., 2012; Bakker et al., 2000) and physicians (Arigoni et al., 2009; Goehring et al., 2005), with a higher risk of burnout for physicians compared to the rest of the hospital staff, due to labour conditions and to those requests and responsibility that are entrusted to the professional figure of the doctor (Hämmig et al., 2012). Many studies (Epp, 2012; Moss et al., 2016; Zhang et al., 2013) show that intensive care units and hospital’s emergency departments can be considered as stressful workplaces, where it’s easy to develop burnout syndrome.
In Maslach model (1982), there are three elements identified as risk factors for burnout syndrome: emotional exhaustion, depersonalization and low personal realization. Emotional exhaustion represents an initial warning signal, followed by defensive detachment reaction; at last, it comes what Maslach defined “low personal realization”. This situation makes health professionals feel bewildered, perceive the loss of the possibility of aid, as much as exhaustion of energies, that can be expressed through physical, psychological or social problems (Gandi et al., 2011; Shimazu et al., 2010; Borritz et al., 2006).
During pandemic or other critical situations, protective factors can help health professionals to face the emergency. After SARS epidemic, health professionals reported that the most functional coping strategies had been: clear guidelines, supervisor’s support, a proper training, precautionary measures and social, familiar and religious support (Chan & Huak, 2004; Cheng & Wong, 2005; Maunder et al., 2006). It’s been demonstrated that even personality traits can have an influence on how health professional’s health may answer to stress. In fact, during SARS emergency optimism, resilience and altruism reduced psychological distress in health professionals (Bai et al., 2004; Lee et al., 2007).
Most of the studies about burnout during COVID-19 emergency period have been conducted on health professionals; one study, in particular, showed a positive, significant relationship between stress and burnout (Morgantini et al., 2020). Another study investigated the relationship between burnout, anxiety and distress during COVID-19 pandemic and shows that physicians and nurses experimented high levels of psychological distress, including burnout (Sung et al., 2020). Bradley e Chahar (2020) suggest the importance of taking care of health professionals’ mental health during pandemic, to improve their productivity and to reduce burnout caused by emergency state, stress and uncertainty.
Some studies suggest that resilience can be considered as a mediator between stress and burnout, indicating that resilience could mitigate harmful psychological effects (Hao et al., 2015). Scientific psychological literature has proposed several definitions of resilience, but most of them is based on two central concepts: adversity and positive adjustment (Fletcher & Sarkar, 2013)
There are several difficulties that an individual must face during life time that require resilience, from little everyday troubles (such as various sort problems at work) up to more important life events (such as the death of a family member). Resilient individuals are more likely to succeed in facing adversity and adapt positively (Bonanno, 2004; Luthar & Cicchetti, 2000; Masten, 2001). Hence, resilience can be defined briefly as the capability of reaching an appropriate and positive adaptation to adversity (Fletcher & Sarkar, 2013).
Today the concept of resilience is used to know and understand health professionals who survive and grow up in the workplace (McCann et al., 2018). Reviews in literature explain that resilience is a necessary quality to succeed in healthcare contexts, because working conditions can be quite adverse (Arrogante, 2015; Jackson et al., 2007). In particular, the concept of resilience can be used to understand how health professionals at risk manage to recover after having provided care to critically ill patients and after being highly exposed to potentially traumatic experiences. In this regard, literature underlines that resilience capability can be taught (McAllister & Lowe, 2011).
Resilience can reduce the adverse effects of stress factors on mental health and promotes positive mental health in difficult times like pandemic. In a study, Arslan and colleagues (2020) examined resilience as a mediator in the relationship between positive affects, negative affects and mental health during the COVID-19 pandemic. Thus, researchers discovered that resilience can reduce the effect of negative affects and improve the effect of positive affects in mental health; furthermore, resilience plays a key role as mediator between the fear of COVID-19, the perceived risk, stress, anxiety and depression (Yildirim et al., 2020).
Concepts like resilience, burnout syndrome and mental health are linked one to another. Scientific literature demonstrated that resilience minimizes and limits negative outcomes of stressful experiences, like burnout syndrome (Dunn et al., 2008). In addition, several findings show that resilience is associated to a better mental and physical health and to a faster recover from the illness (Connor & Davidson, 2003). Despite that, there are still few evidences that demonstrate the resilience to be a mediator between burnout and health professionals’ health (Arrogante & Aparicio-Zladivar, 2017).
The present study aims to investigate the differences between healthcare professionals recruited by the ASST (“Azienda SocioSanitaria Territoriale”, acronym indicating a local hospital) of the city of Lodi in the year 2019, and those recruited since March 9th, the first day of Italian national lockdown. First, we want to investigate demographic variables and then to observe burnout and resilience in the sample.
Health professionals newly recruited from the hospital are subjected to a battery of tests, aimed at specifying the psychological suitability for the job, provided by Lodi ASST Clinical Psychology Unit. Media coverage of COVID-19 news made people, and in particular health professionals working closely with patients in public structures, concerned because of the contagion spreading. This condition not only increases the workload of stress, but also challenges individual personal resilience.
Our two samples (one from 2019 and one from 2020) are particularly useful to understand the impact of the present emergency on the perception of newly recruited health professionals, capturing a direct difference in the virus, which could lead to psychological major risks in patient treatment performance.
Our aim is to observe how much burnout levels and all its dimensions and resilience levels changed in 2020 recruited health professionals, compared to the 2019 ones. Moreover, a further goal is to observe how resilience can mediate between COVID-19 and burnout levels.
Up to now, there have been many studies investigating burnout and resilience in health professionals in relation to COVID-19 (Barello et al., 2020; Luceño-Moreno et al., 2020; Ruiz-Fernández et al., 2020; Raudenská et al., 2020; Matsuo et al., 2020; Dinibutun, 2020; Varrassi, 2020; Carmona-Rega et al., 2020; Bozdağ & Ergün, 2020; Mosheva et al., 2020; Petzold et al., 2020; Ran et al., 2020), but only a few of them realized a comparison between a former sample and a later one (Hwang et al., 2020; Stacey et al., 2020) and, anyway, none of them related burnout and resilience.
Participants
Group "before COVID-19". 85 health workers participated in the study from January 2019 to December 2019. The recruitment criterion was the condition of each employee as a new employee in the Lodi ASST, who, as per protocol, is sent by the competent doctor for the preventive visit psychological routine. Of the 89 new hires, 4 dropped out of the study, as they no longer worked in the hospital and never completed tests. The tests were administered in the presence of the clinician through modules.
The percentage of male participants is 29.4% (n = 25), whereas the percentage of female participants is 70.6% (n = 60).
The average age is 35 years, with an SD of 8.9 years and with a range that goes from a minimum of 24 to a maximum of 61 years.
Group "after COVID-19". 104 health workers participated in the study from April 9th 2020 to October 30th 2020. The recruitment criterion was based on the Lodi ASST protocol: all the new hires were sent by the competent doctor to the Clinical and Occupational Psychology Department for the routine preventive visit. Among the 114 healthcare workers hired this year, 10 participants were excluded from the study for failing to properly complete the tests. The tests were administered by the clinician by telephone, in compliance with current regulations on COVID-19, through online forms.
The percentage of male participants is 29.8% (n = 31), while the percentage of female participants is 70.2% (n = 73).
The average age is 34 years, with an SD of 10.1 years and with a range that goes from a minimum of 22 to a maximum of 61 years.
Measures
Socio-demographic characteristics. A self-report questionnaire was administered to collect demographic data: gender, age, position in the hospital and work department.
Maslach Burnout Inventory. The Italian version of the Maslach Burnout Inventory (MBI; Maslach, 1982; Sirigatti et al., 1988) was used as an assessment tool for the level of burnout among healthcare professionals, in three subscales: Emotional Exhaustion (EE), Depersonalization (DP) and Personal Realization (PR). The tool was administered using a 7-point Likert scale, where 0 points denote the "never" response, and 4 points denote the "every day" response. The EE subscale reveals the operator's sensations in his energy expenditure, fatigue and being fed up in eight items; the DP subscale underlines the detached attitude with patients in six items; the PA subscale measures feelings of competence and perceived success achieved at work in eight items. Cronbach's alpha of the subscales at baseline for the "before COVID-19" group was α = .90 for EE, α = .79 for DP, and α = .71 for RP, indicating internal consistency acceptable to good. Cronbach's alpha of the subscales at baseline for the "after COVID-19" group was α = .92 for EE, α = .76 for DP, and α = .72 for RP, indicating internal consistency acceptable to good.
Resilience Scale. The Italian version of the Resilience Scale (Wagnild & Young, 1993; Girtler et al., 2010) was used to measure the resilience level of the study participants. We used the 10-item version of the tool, on which we scored on a 7-point Likert scale, where the value of 1 was equivalent to the strongly disagree response "and the value of 7" strongly agree ". Cronbach's alpha of the baseline scale for the "before COVID-19" group was α = .94, demonstrating good reliability of the test. Cronbach's alpha of the baseline scale for the "after COVID-19 group” was found to be α = .89, demonstrating a good reliability of the test.
Analysis
All data was analysed using SPSS version 26 (IBM, 2017). Descriptive statistics were carried out on the demographic variables and on the Resilience, EE, DP, RP and MBI Total variables, for both groups, "before COVID-19" and "after COVID-19".
Pearson's correlations between the dimensions of burnout, resilience and demographic variables were measured in both samples.
We wanted to determine the different levels between the two groups by creating a dummy variable that would represent the condition "before COVID-19" and "after COVID-19". The size of the effect was measured using f2, which is definable as the variance ratio explained by the interaction term alone with the unexplained variance in the final model. According to Cohen and colleagues (2003), the cut-offs for the size of f2 are small, medium and large, with .02, .15, and .35, respectively.
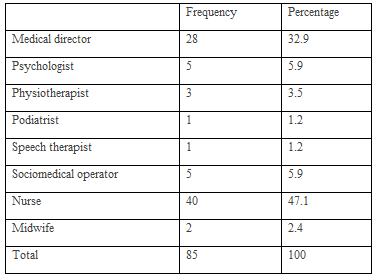
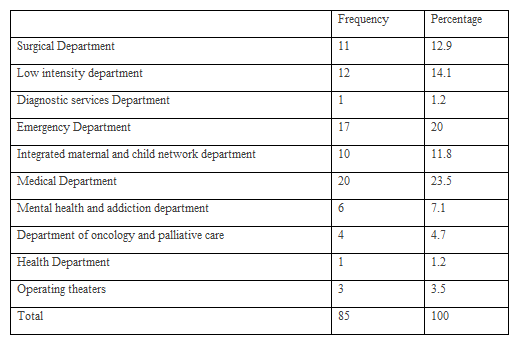
Group "before COVID-19". The descriptive statistics show the frequencies of duties (Table 1) and the departments in which health professionals work (Table 2). The job most presented is that of nurse (40 subjects, 37.1%), while the department from which more subjects came is the medical department (20 subjects, 23.5%).
The 85 subjects had an average score of 59.58 ± 5.42 on the Resilience Scale (indicating moderately high resilience); an average score of 12.36 ± 6.77 on EE (indicating a low level of emotional exhaustion); an average score of 7.39 ± 4.21 on PD (indicating a moderate level of depersonalization); an average score of 33.69 ± 5.5 on the PR (indicating a moderate level of personal achievement).
The Mann-Whitney U non-parametric two-sample test showed no association between the membership group and the Resilience Scale and MBI test results, neither for gender, nor for job, nor for work department. Therefore, within our sample, it is not desirable that the scores have depended on the particular type of employment and gender.
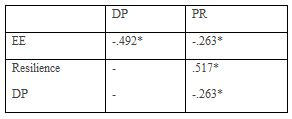
The correlation analysis between resilience and burnout demonstrated three significant associations (p <.01) (Table 3): EE correlates positively with PD but not with PR, while resilience correlates negatively with EE is positively with RP, but is not related to DP.

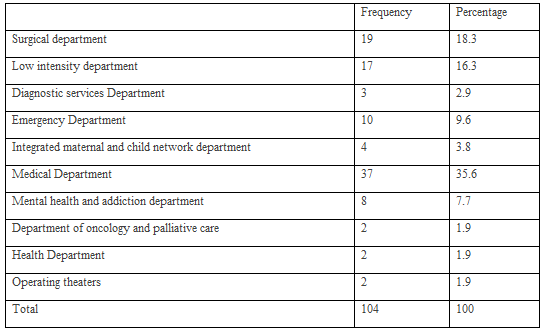
Group "after COVID-19". The descriptive statistics show the frequencies of duties (Table 4) and the departments from which health workers come (Table 5). The job most presented is that of nurse (63 subjects, 60.6%), while the department from which more subjects came is the medical department (37 subjects, 35.6%).

The 104 subjects had an average score of 56.7 ± 10.01 on the Resilience Scale (indicating moderately high resilience); an average score of 7.81 ± 7.53 on EE (indicating a low level of emotional exhaustion); an average score of 3.1 ± 3.85 on PD (indicating a low level of depersonalization); an average score of 36.98 ± 6.54 on the PR (indicating a moderate level of personal achievement).
The Mann-Whitney U non-parametric two-sample test showed no association between the membership group and the Resilience Scale and MBI test results, neither for gender, nor for job, nor for work department. Therefore, within our sample, it is not desirable that the scores have depended on the particular type of employment and gender.
The correlation analysis between resilience and burnout demonstrated four significant associations (p <.01) (Table 6): EE is negatively correlated with PD and with PR, DP negatively correlated with PR, while resilience correlates positively with PR, but is not correlated with EE and DP.
Analysis between samples "before COVID-19" and "after COVID-19". To measure the equivalence between the two samples, t-tests were performed on the demographic characteristics and on the variables of interest. The two samples did not differ significantly in terms of age (t = -.718, p > .05), gender (t = -.59, p > .05), resilience (t = -3.807, p > .05), EE (t = -4.329, p > .05), DP (t = -7.303, p > .05) and PR (t = 3.499, p > .05).
We then tested the main effect of the variables on burnout levels in the sample "after COVID-19". The size of COVID-19 had only a small major effect on EE (b = -.048, p <.05, f2 = .02), and also with regard to resilience (b = -.290, p <. 05, f2 = .056). On the DP, there was no effect of the COVID-19 variable (b = -.040, p <.05, f2 = .002), but resilience once again did (b = -.186, p <.05, f2 = .035). Regarding PR, the COVID-19 variable showed small effect size (b = -.07, p <.05, f2 = 0.053), while resilience showed a large effect size (b = -.517, p <.05, f2 = 0.364).
As further proof of the analyzes carried out so far, we performed a stepwise regression to verify which variables to exclude for the different models (Table 7).

From all three analyzes, the COVID-19 variable was always excluded from the models. The most significant model turned out to be only the one that saw resilience as a predictor of RP in burnout.
The results of our study turned out to be interesting: first of all, the comparison tests between means determined a substantial lack of difference between before and after the pandemic outbreak. Specifically, the COVID-19 condition had no significant influence on the level of burnout, much less on resilience. This is an interesting fact because, working in the active health context and being a public hospital, the health worker doesn't have the possibility to personally select patients, and exposes himself or herself to risk in the most concrete way.
Considering the present literature (Barello et al., 2020; Jalili et al., 2020; Raudenská et al., 2020), healthcare workers subjected to COVID-19-related stress had low burnout size outcomes. The same could have been expected for the health workers of the Lodi ASST, especially considering that the first COVID-19 outbreak and the first "red zone" put in lockdown measures was in the province of the city of Lodi. Instead, from the analysis of the data, something different was found, which could be due precisely to the difference from the other studies, that is, considering the condition of new hires of health workers. Considering that low scores on the psychological tests of new hires is not a condition that makes the hiring risk, the operators responded correctly to the administration. On recruitment, most healthcare workers do not result in burnout (Mazzella Ebstein et al., 2019), but the global outbreak of COVID-19, media pressure, government regulations, restrictions on social and work relationships are all factors that could have influenced the psychological assessment of a person who is about to be hired in a context with a high risk of contagion. The awareness of being in a dangerous situation and having to work in contact with possible people positive to COVID-19, with the virus transmitting risk to loved ones could have been an element that would've caused not only a high burnout, but a low resilience too, considering how much the pandemic has made us re-evaluate how much we can do and how much we can act against an invisible enemy.
Instead, what emerged was that the newly hired healthcare workers didn't result in burnout and scored well on resilience. As already widely recognized in the literature (Kutluturkan et al., 2016; Santosh & James, 2013; Yang et al., 2018), good resilience easily predicts a low level of burnout: so it was in our study. In the 2019 sample, resilience predicted two of the dimensions of burnout, while in the 2020 sample, it predicted one of the dimensions of burnout. The level of burnout may depend on other factors, such as coping (Mattei et al., 2017), but COVID-19 wasn't one of them at the time of hiring. The prospect of a new job as a health worker, especially in view of a health emergency and high demand for assistance, may have been the reason for high resilience and low burnout. COVID-19 would therefore not have influenced the level of work stress that would have been expected: compared to the 2019 sample, the new hires during the peak of the epidemic didn't show substantial differences. In a time when the professional hasn't yet experienced healthcare work closely in pandemic times, his or her perception of work doesn't seem to be altered by the COVID-19 condition, thus allowing him or her to start a new job with a burnout-free basis.
The two different samples represent different people and a different number of jobs and departments per person. This may have been a limitation to the study, due to the different stratification between the two samples, as well as the fact that the previous mental state of the participants of both samples, and the number of samples themselves, were not known. As further proof, we could think that it might be useful to include a variable for COVID-19 such as fear of contagion. It'll be interesting, in the future, to observe how the burnout and resilience conditions will change in the same individuals who continued to work in the Lodi ASST, while, for subsequent studies, it'll be interesting to insert new variables that measure various other psychological constructs.
There’s no conflict of interests.
There’s no funding to this study.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
