
Case Report | DOI: https://doi.org/10.31579/2641-0419/182
*Corresponding Author: Kana Fujikura, MD, PhD, Advanced Cardiovascular Imaging Laboratory, National Heart, Lung and Blood Institute, National Institutes of Health, Department of Health and Human Services. 10 Center Drive, Bldg 10, Rm B1D416 Bethesda. MD 20892-1061
Citation: Calin V. Maniu, Kana Fujikura., (2021) Newly Diagnosed Heart Failure with Renal Insufficiency – Cardiac MRI-guided Clinical decision making. J. Clinical Cardiology and Cardiovascular Interventions, 4(11); Doi:10.31579/2641-0419/182
Copyright: © 2021 Kana Fujikura, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 10 May 2021 | Accepted: 17 May 2021 | Published: 25 May 2021
Keywords: Heart failure; cardiac magnetic resonance imaging; ischemic cardiomyopathy; cardiomyopathy
A 63 year-old female with multiple atherosclerotic risk factors presented with newly diagnosed heart failure. Clinical presentation and initial work-up studies (e.g. laboratory findings, ECG, and echocardiography) were indeterminate for ischemic or non-ischemic etiology. As she developed contrast-induced nephropathy, coronary angiography was initially deferred and cardiac MRI was performed instead. Cardiac MRI elegantly demonstrated non-ischemic cardiomyopathy that was subsequently confirmed by invasive coronary angiography. This case emphasizes the important role of cardiac MRI in establishing the etiology of cardiomyopathy, ultimately altering the clinical management of the patient with newly diagnosed heart failure.
A 63 year-old female with hypertension, hypercholesterolemia and active cigarette smoking presented with orthopnea and dyspnea on exertion that had worsened over the previous 2 months. Pulmonary embolism was ruled out with chest CT angiogram. ECG showed new T-wave inversion in the lateral wall when compared to an old tracing (Figure 1)

.Laboratory data showed severely elevated pro-BNP (23,615 pg/mL). Initial troponin T was undetectable. Her renal function worsened secondary to contrast-induced nephropathy (Cr 1.5 mg/dL [baseline 0.9 mg/dL], eGFR 42 ml/min/1.73 m2 [baseline 71 ml/min/1.73 m2]). Echocardiography showed biventricular dilatation and decreased systolic function (LV EF 20%) with regional wall motion abnormalities (Video 1).
Video 1: Echocardiography of apical (A) 4-chamber, (B) 2-chamber, and (C) 3-chamber views. The left ventricle was mildly dilated with severely decreased function. The right ventricular function was moderately decreased. The left ventricular wall motion was globally severely hypokinetic with regional variations. Inferior and inferoseptal segments were akinetic, whereas the wall motion of basal anterior and lateral segments were rather preserved. The findings were suggestive of ischemic cardiomyopathy.
Cardiac MRI cine imaging showed severely dilated LV with severely decreased systolic function (LVEF 17%) with global hypokinesis (Video 2).
Video 2: Cardiac MRI steady-state free precession (SSFP) cine imaging of long axis views: (A) 2-chamber, (B) 3-chamber, and (C) 4-chamber views. Cardiac MRI cine imaging showed severely dilated left ventricle with severely decreased systolic function (ejection fraction 17%). The left ventricular wall is globally severely hypokinetic with minimal regional variations. There were prominent trabeculations in the anterior wall from base to apex that did not meet the criteria for non-compaction. The right ventricle was severely dilated with moderately decreased systolic function.
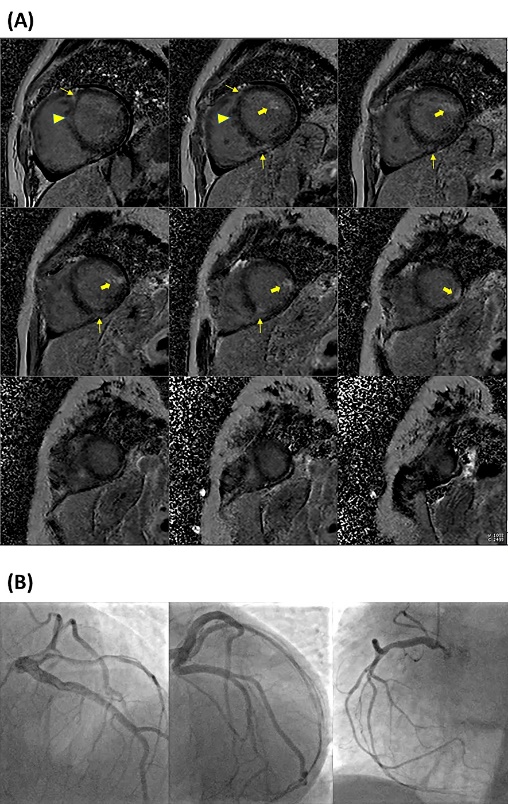
On late gadolinium enhancement imaging, there was patchy myocardial fibrosis in the anterolateral papillary muscle and a small portion of the mid lateral wall, mid-wall fibrosis in the basal anteroseptal segment, and fibrosis at both anterior and inferior right ventricular insertion sites (Figure 2A). Cardiac MRI findings were compatible with non-ischemic cardiomyopathy. Invasive coronary angiography performed due to subsequent troponin elevation revealed normal coronaries (Figure 2B).
Antiplatelet therapy was discontinued. She was discharged home with low dose furosemide, carvedilol, losartan, isosorbide dinitrate, and hydralazine. Her symptomatic status improved and furosemide was discontinued. Losartan was then switched to sacubitril/valsartan. Subsequent dose up-titration of her regimen was well tolerated and she remained in NYHA class I. Follow-up echocardiography showed normalization of LV size along with improvement of the systolic function (LVEF 45 %) 4 months after her initial presentation.
Coronary artery disease is the most common cause of systolic heart failure in Western countries. Ischemic cardiomyopathy is associated with decreased survival when compared to non-ischemic cardiomyopathy [1]. If feasible, surgical coronary revascularization improves survival when compared to medical management [2]. This case emphasizes the important role of cardiac MRI in establishing the etiology of cardiomyopathy, ultimately altering the clinical management of the patient with newly diagnosed heart failure.
Disclosures: There are no relationships with industry.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
