
Review article | DOI: https://doi.org/10.31579/2578-8868/203
1 Department of Neuroscience, Biomedicine and Movement Sciences - Verona University, Verona, Italy
*Corresponding Author: Sheila Veronese, Department of Neurosciences, Biomedicine and Movement Sciences, Verona University – 10 Sq. A.Stefani, Verona 37134, Italy
Citation: Sheila Veronese, Marco Cambiaghi, Andrea Sbarbati (2021) New Protocol for Auditory Brainstem Implant Positioning. J. Neuroscience and Neurological Surgery. 9(5); DOI:10.31579/2578-8868/203
Copyright: © 2021 Sheila Veronese, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 20 August 2021 | Accepted: 29 September 2021 | Published: 12 October 2021
Keywords: ABI; EABR; intraoperative monitoring; electrodes positioning
Background: Surgery for applying the auditory brainstem implant is an otoneurosurgery that requires careful intraoperative monitoring to optimize the placement of the electrode paddle. This study aimed to validate a new method capable of increasing the accuracy of electrode array placement, reducing channel interaction, electrical artefacts, and saturation effects, and providing the largest number of electrodes that can be activated with the lowest possible electric charge.
Materials and methods: Thirty-six subjects aged between 1.42 and 69.92 years were tested during surgery for auditory brainstem implantation. We recorded auditory electrical responses of the brainstem using the implant supplier's suggested stimulation protocol and the new protocol.
Results: Saturations effects and electric artefacts were noticed respectively in 81.85% and 53.25% of recordings using implant supplier's method, while in 70.34% and 24.75% of recordings using the new method, with a percentage variation of 11.51% and 28.50%. Considering the amount of charge required to activate the electrodes, with the implant supplier's method an average charge of 14 nC was needed, while with the new protocol an average charge of 8 nC was necessary.
Conclusions: The new method improves the coupling between the auditory brainstem implant and the surface of the cochlear nucleus.
The auditory brainstem implant (ABI) represents a device that effectively restores auditory sensations in patients with NF2 and acoustic neuromas. Its application was extended to children and adults with injuries or malformations of the cochlea and cochlear nerve, who are not eligible for a cochlear implant [1], [2].
The use of electrophysiology, in particular of the electrical auditory brainstem responses (EABR), is known to facilitate electrode plate placement during ABI implant surgery [3], [4], [5].
Waring optimized pacing and recording parameters to achieve efficient EABR monitoring during surgery [6], [7]. Achieving efficient monitoring means being able to recognize the waveforms of auditory responses and distinguish them from the current of stimulation and other evoked potentials that could result from stimulation of nearby non-auditory anatomical structures.
Many authors have tried to define the optimum EABR monitoring procedure and to correlate its results with the auditory outcomes [8], [9], [10], [11], [12], [13].
Nevison et al. [8] demonstrated that achieving good intraoperative EABRs is not related to the performance of implanted patients, but subjects who achieve good EABRs also have postoperative auditory sensations. Furthermore, they reported the presence of non-auditory sensations during ABI programming in 92.3% of cases. This means that the number of usable electrodes varies significantly between subjects, and that an imperfect coupling of the electrodes with the cochlear nuclei can more easily induce the excitation of non-auditory stimulations.
This study aimed to validate a new method capable of increasing the accuracy of electrode array placement, reducing channel interaction, electrical artefacts, and saturation effects, and providing the largest number of electrodes that can be activated with the lowest possible electric charge.
Surgical and electrophysiological procedures were approved by the Ethics Committee of Verona Hospital. For these procedures, an informed written consent was acquired from the patients and children’s parents. This study
was carried out in accordance with the Declaration of Helsinki.
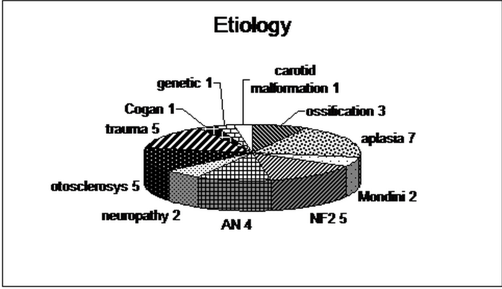
Thirty-six ABI subjects aged between 1.42 and 69.92 years were tested during ABI implantation surgery. They presented different aetiologies (Figure 1). The chosen implant was the Cochlear Nucleus ABI24M (Cochlear Ltd., Sydney, Australia), for all the patients.
The amplitudes analysis of EABRs recorded from the edge electrodes of the array (Figure 3b) permits to quantify both the rotational shift and the transversal axis of the array respect to the cochlear nucleus surface. Instead, EABR recordings from the lateral electrodes of the array (Figure 3c) clarifies the longitudinal axis of the array respect to the axis of the cochlear nucleus.
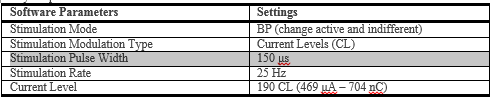
Software parameters are reported in Table 1. All electrode combinations were stimulated with alternate current so to cancel the stimulus artefact.
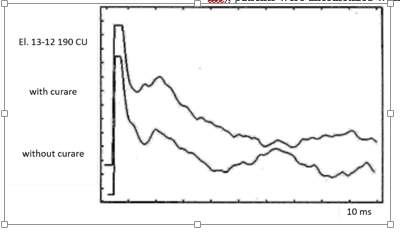
In order to evaluate only the acoustic response (without components of other cranial nerve stimulation, usually presented after the first 4 – 4.5 ms), patients were anesthetized with curare (Figure 5).
Data were analyzed from the morphological point of view, in terms of number and amplitudes of the peaks in each recording, and considering the presence of saturation effects and of electric artefacts.
Activation occurred from 27 to 67 days from the surgery. The amount of charge needs to elicit the acoustic response was compared.
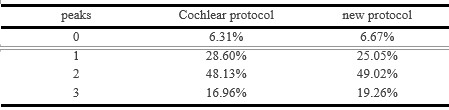
n all patients, intraoperative EABR were recorded, obtaining 507 waveforms with Cochlear electrodes combination and 917 waveforms with the new procedure. Table 2 summarized the characteristics of both protocols’ waveforms. Respectively, in 6.13% (Cochlear pr.) and 6.67% (new pr.) of cases, it was impossible to obtain an acoustic response. Most frequently a 2-peaks wave was obtained with both procedures. A significant reduction (3.54%) of 1-peak waves was noticed with the new protocol, while there was an increase of 2.29% in 3-peak waves presence.
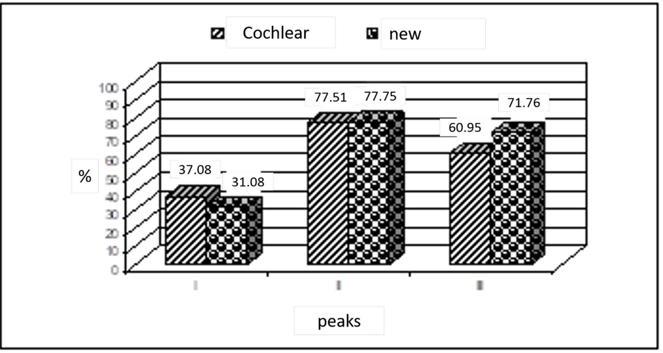
In Figure 6, peaks in each waveform are shown, considering the standard latencies of 0.7 ms (0.6 ms – 1.1 ms) for the first peak, of 1.6 ms (1.2 ms – 1.9 ms) for the second peak and of 2.7 ms (2.2 ms – 3.7 ms) for the third peak [7]. Peak II was the most dominant and reliable peak for both methods. Peak I was detected 31.08% of times with the new protocol with a decrease of 6% respect to Cochlear protocol. Using the new protocol peak III was identified in 71.76% of recordings (10.81% more than using Cochlear protocol).
Examples of EABR recordings of the same subject are shown in Figure 7. In Table 3, mean amplitude values of different peaks are presented. Magnitude of these waves is larger using Cochlear method. Particularly, this is evident for peak I. In Figure 8 is shown the EABRs recorded with an electrode combination in witch distances between the active and reference electrodes are progressively reduced. It is clear that shorter is the distance, lower is the magnitude. This means that enlarging the distance between the electrodes a larger number of fibers are elicited and so in the recorded response a sizeable component of other electrodes is presented.
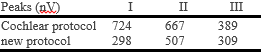
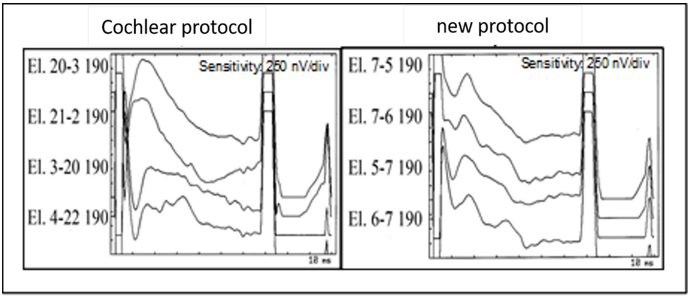
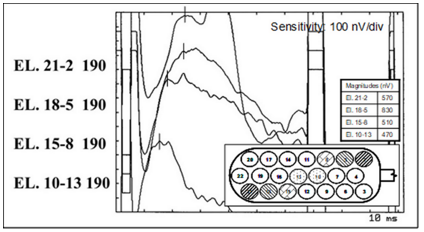
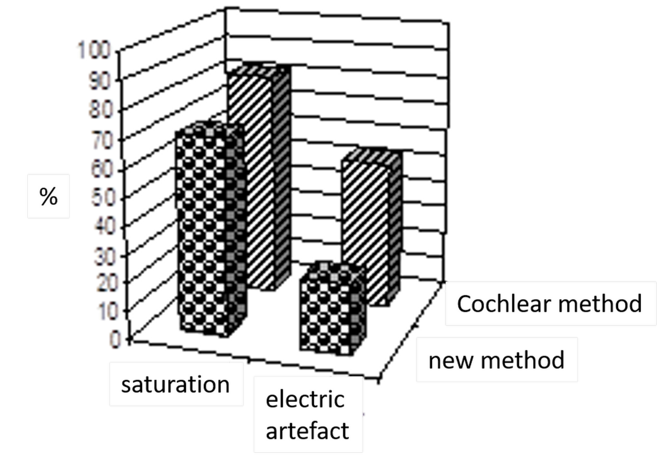
Figure 9 describes the percentage of EABRs presenting saturation effects and/or electric artefacts. Saturations effects and electric artefacts were noticed respectively in 81.85% and 53.25% of recordings using Cochlear method, while in 70.34% and 24.75% of recordings using the new method, with a percentage variation of 11.51% and 28.50%.
Tuning of the implants was performed in intensive care unit. Patients were seated in a comfort position and connected to ECG monitoring equipment to supervise their heart rhythm.
At activation of ABI, the amount of charge required resulted of 14 nC (SD = 30, max = 137 nC, min = 3 nC) for the patients tested with the Cochlear method, and of 8 nC (SD = 8, max = 29 nC, min = 2 nC) for the patients tested with the new method.
In order to increase the accuracy of the evaluation of the electrodes array placement a new procedure was developed. Aim of this procedure was to reduce channel interaction, electric artefacts and saturations effects. At the same time, it was intended reduce the amount of electrical charge needed to activate the electrodes post-operatively.
During ABI insertion EABR were recorded with both Cochlear suggested electrodes combination and a new combination of electrodes.
Responses were obtained in the same percentage for the two methods. It is interesting the reduction of 1-peak waves noticed with the new protocol and the increase of 3-peak waves. That is, waveforms appear to be more evident.
Analyzing the different peaks, peak II was the most dominant and reliable for both methods. A significant reduction of peak I detection was observed as an increase of peak III detection. But data didn’t confirm this hypothesis. On the contrary, they underlined the reductions of both these interferences. Changing perspective, it might be interested to evaluate waveforms obtained with Cochlear electrode combination. Enlarging the distance between the electrodes a larger number of fibers were elicited and so in the recorded response a sizeable component of other electrodes was presented. At this point the question was: was it possible that the first peak was due to channel interaction? Looking at the effect of channel interaction on peak magnitude (Figure 8) it can be assumed that other electrode components determined the more extensive presence of peak I in Cochlear protocol recordings.
The increase in peak III detection observed with the new procedure was explained by the saturation effect reduction.
The new procedure appears to ensure that the electrodes are stimulated with a lower current charge. And this means that the coupling obtained with the cochlear nucleus surface is better with the new procedure, being the ABI implant closer to the nucleus itself.
Conclusion
The new procedure appears to ensure that the electrodes are stimulated with a lower current charge. And this means that the coupling obtained with the cochlear nucleus surface is better with the new procedure, being the ABI implant closer to the nucleus itself.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
