
Research Article | DOI: https://doi.org/10.31579/2578-8868/269
Neurophysiology Department, Ysbyty Gwynedd Hospital, Bangor, North Wales, UK. LL57 2PW.
*Corresponding Author: Salim Hirani, Neurophysiology Department, Ysbyty Gwynedd Hospital, Bangor, North Wales, UK. LL57 2PW.
Citation: Salim Hirani, (2023), Neurophysiological study for Ulnar Entrapment at Wrist, J. Neuroscience and Neurological Surgery. 13(4); DOI:10.31579/2578-8868/269
Copyright: © 2023, Salim Hirani. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 07 June 2023 | Accepted: 02 October 2023 | Published: 04 October 2023
Keywords: ulnar nerve neuropathy at wrist ; guyon’s canal ; dorsal ulnar cutaneous nerve entrapment, wrist injury cause ulnar nerve entrapment ; ulnar sensory branch entrapment
Background:The localization of ulnar nerve entrapment across wrist (UNEAW) may be categorised in a number of ways utilising one of a range of presently available methods via nerve conduction study (NCS). A number of approaches as to how to confirm entrapment at the wrist have been described in the literature. There are number of research paper showing several different ways to confirm entrapment.The aim of this research is to establish, using the best available evidence, a clinically appropriate revision of the current UNEAW nerve conduction study, and to compare this with existing Neurophysiological procedure. The proposed revised research is based on more nuanced, descriptive categories, ranging from ulnar sensory branch in digit V, mid palm ulnar sensory entrapment, sensor-motor entrapment across wrist and involvement of dorsal ulnar cutaneous nerve (DUCN). Method: A total of 46 hands were included in this study. Data was collected based on the extensive and detailed description mentioned in different research papers. The tests were performed by a qualified clinical physiologist (Neurophysiology) using a Keypoint 9033A07 machine, used in line with departmental protocol (Ulnar nerve screening protocol1.1, 2020). All data was recorded numerically to ensure methodological reliability. Result:Of the 46 hands tested, the NCS showed that 21 hands had entrapment only in ulnar sensory branch at digit V, 16 hands showed entrapment below wrist (at the palm), 12 hands showed entrapment across wrist (Guyon’s Canal), 11 hands showed entrapment across elbow involving ulnar sensory branch as well, and only one hand showed sensory entrapment above wrist due to a local injury. Conclusion: The ulnar nerve entrapment at or below wrist could easily be missed. Lack of familiarity of the anatomical localization of ulnar sensory nerve could be misdiagnosed with entrapment across elbow. Nerve conduction study is necessary to diagnose the level of entrapment of ulnar nerve at or below wrist.
The ulnar nerve is the second most common compressed nerve at the elbow in the region of the cubital tunnel and less frequently at the wrist in the Guyon’s canal or below 5. With the compression of the ulnar nerve, patient complaints can include paraesthesia or numbness, or both, in the small or the ring finger, or in both. In more severe cases, ulnar nerve motor dysfunction will lead to weakness, atrophy, pain across elbow and hand clumsiness 6.
Reason:
The aim of this research is to establish, using the best available evidence, a clinically appropriate revision of the current UNEAW nerve conduction study, and to compare this with existing Neurophysiological procedure.
There are several primary grading tests mentioned in literature, such as placing paper between digits IV-V, Tinel sign at wrist or elbow, flexion elbow at 90 ͦ, supinate the forearm, and extend the wrist. These are subjective tests based on patient’s clinical response. Other tests like Ultrasound, NCS and EMG needle examination are objective tests that have been used for Ulnar nerve entrapment (UNE) which are reliable, evidence-based and objective test, and not dependent on patient’s clinical response.
T1o ascertain the severity and level of entrapment of ulnar nerve, specific neurophysiological testing is required. There are several investigations specifically related to UNE; [Karvelas9, Daniele Coraci6, Solange G. Garibaldi11, Magdalena Lewanska10, Laboratoire d’e´lectromyographie8, Anthony Chiodo2, and Carisa Pearce4]. Most of the grading studies are subjective. Some lack a neurophysiological focus in objectivity during the collection of the data. Some researches only use either Sensory NCS or Motor NCS or ultrasound to differentiate the severity of ulnar nerve. Not all researchers have used sensitive techniques to diagnose ulnar nerve entrapment at different levels at or below wrist.
It appears that there is no clear accepted dominance of any study universally; a proper neurophysiological test is required to diagnose the level of severity of ulnar nerve at or below wrist.
There is no clear guidance to diagnose the ulnar nerve at or below wrist published by BSCN British Society for Clinical Neurophysiology (BSCN) or (Association of the neurophysiological scientists (ANS) which are the professional bodies in the UK.
The aim of this research is to establish, using the best available evidence, a clinically appropriate revision of the current UNEAW nerve conduction study, and to compare this with the existing Neurophysiological procedures. This could support the Surgeon to ascertain the level of severity and decide on a conservative or surgical approach to treatment. Although surgeons have to take their own decision for the treatment, if they want to consider the treatment on the basis of Nerve conduction study, it will benefit by patient for proper treatment.
No clinical assessments were conducted during the Neurophysiological test so as eliminate bias of the patient’s condition.
The test was performed by a qualified Clinical Physiologist (Neurophysiology) using Keypoint 9033A07 (Skovlunde, Denmark) machine, on the basis of departmental protocol (Ulnar nerve screening protocol1.1, 2020). A quantitative method was used for collecting data, to ensure accuracy and to avoid bias. The sample size of patients in the study was used for all those tested for NCS over a period of 6 months from October 2019 to March 2020, across the population of North Wales. The data was collected from patients with an age range above 18 years, who were referred to the Neurophysiology department from the Orthopaedics and Neurology departments within the local Health Board, as well as General Practices (GPs) in North Wales. No individual patient was recruited in this research. The inclusion criteria were considered only on the basis of the referral diagnosis. No clinical assessment was conducted prior to the study in the department. Referral was considered based on paraesthesia, pain, swelling in median or ulnar distribution area or digits IV-V, worsened by sleep.
Data was analysed on certain widely accepted assumptions of sensory amplitude and CV and distal motor latency (DML), amplitude and CV1,3.
The procedure started by carrying out the sensory testing, by placing the stimulating ring electrodes on digit III4 and the recording electrode on the surface of the median nerve on the wrist. Same procedure applied while recording ulnar nerve from digit V to wrist. The orthodromic technique was used for both sensory and motor NCS test, for median and ulnar nerves. A maximal current was applied to record the full response of the nerve, at the digits III for median sensory and digit V for ulnar sensory recording1. A maximal current was applied to stimulate median nerve pathways at the wrist and at the elbow for motor recording from abductor pollicis brevis (APB), and ulnar nerve pathways from First dorsal interosseous (FDI). Recording were made from wrist by stimulating the mid-palm of the ulnar side, to test if either the response from digit V was less than 5µV or absent. Response was recorded from Dorsal ulnar cutaneous nerve (DUCN) if amplitude was less than 5µV or absent between palm to wrist and between digit V to wrist. Amplitude was recorded from peak to peak for sensory responses, and base to peak for motor responses.
All patient data was collected by fulfilling the criteria mentioned in above paragraph depending on the severity. The reason for using an additional criteria is to describe the full range of severity which was not fully covered by other researchers mentioned earlier in this paper. Criteria mentioned in above paragraph are intended to be more reliable from a Clinical Physiologist prospect.
The data was collected for a period of 6 months from October 2019 to March 2020. A total of 46 hands were included in this study. Of the 46 hand tested, 22 were right handed and 24 were left handed. The age range was 19 to 98 years, with a median age of 56 years. The numbers of hands in each grade of severity are shown in Figure 1 and Table 1.
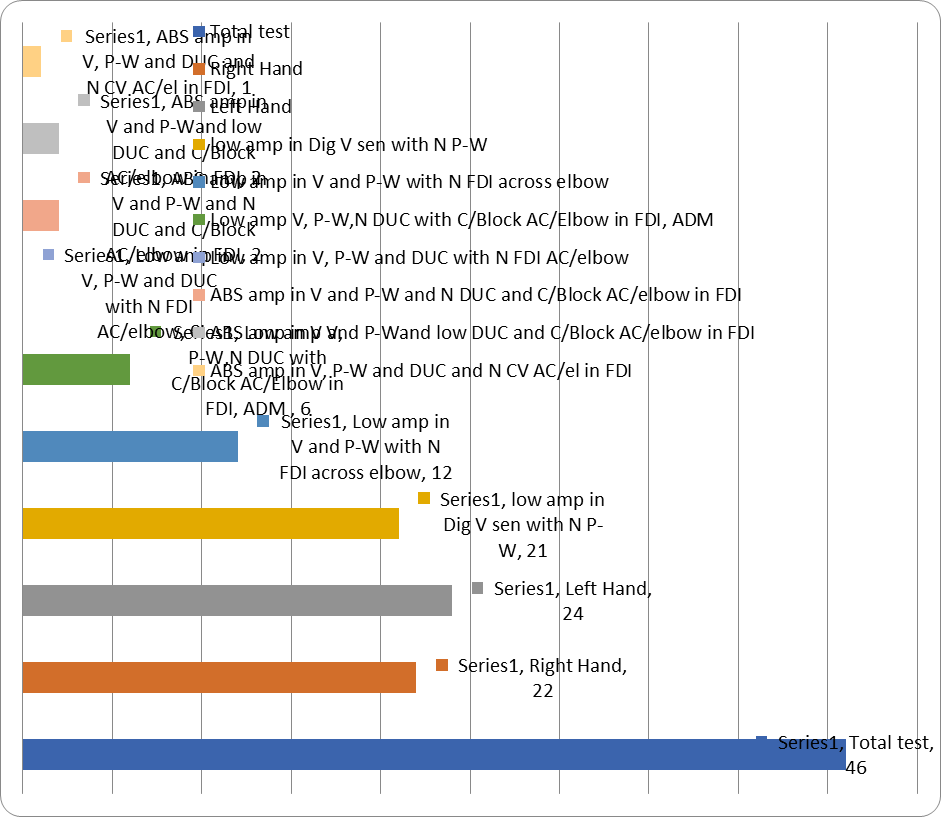
Figure 1: Level of severity of ulnar nerve at or below wrist
| Total test | 46 |
| Right Hand | 22 |
| Left Hand | 24 |
| low amp in Dig V sensory with N P-W | 21 |
| Low amp in V and P-W with N FDI AC/El | 12 |
| Low amp V, P-W,N DUC with C/Block AC/El in FDI, ADM | 6 |
| Low amp in V, P-W and DUC with N FDI AC/el | 0 |
| ABS amp in V and P-W and N DUC and C/Block AC/el in FDI | 2 |
| ABS amp in V and P-Wand low DUC and C/Block AC/el in FDI | 2 |
| ABS amp in V, P-W and DUC and N CV AC/el in FDI | 1 |
Table 1: Level of severity of ulnar nerve at or below wrist
Ulnar nerve entrapment at the wrist is uncommon and difficult to diagnose; therefore, it is important to understand the nerve’s anatomical course and distribution to allow for accurate diagnosis by clinical and electrodiagnostic evaluations. Electrodiagnosis is proving to be an important tool in identifying ulnar nerve lesions at the wrist while excluding other disorders in the differential diagnosis such as cubital tunnel syndrome, brachial lower trunk plexopathy and C8–T1 radiculopathy8.
Compression of ulnar nerve at wrist is not limited to Guyon’s canal. In 1969, Shea and McClain12 described 3 different types of ulnar nerve compression syndromes at the wrist based on the anatomical presentation of ulnar nerve.

Figure 2: This diagram depicts the course of ulnar nerve at the right wrist, which is ulnar to the ulnar artery. The yellow color highlights the zone I, the green highlights the zone II, and the purple highlights the zone III. A, ulnar artery; N, ulnar nerve; P, pisiform; H, hamate; TCL, transverse carpal ligament.
Later, Gross and Gelberman’s cadaveric study7 detailed the relationship between the symptoms and 3 anatomical zones of ulnar nerve compression at the wrist.
The data from the current study showed that out of 46 hands, 16 hands showed low amplitude Sensory nerve action potentials (SNAPS) in digit V with normal amplitude between palm to wrist, DUCN and FDI across elbow. This would be the lesion at mid palm at the ulnar sensory branch which supplies the digit V. This could be a local lesion due to use of crutches or riding bicycle on rough road etc. 12 hands showed low amplitude sensory potentials in digit V and between palm to wrist with normal sensory amplitude from DUC and normal distal motor latency and conduction velocity across elbow while stimulating the FDI muscles. This lesion is in the sensory branch of ulnar nerve at the wrist and motor branch was spare. This would be a part of Guyon’s canal entrapment with no motor involvement. 4 hands showed low amplitude sensory potentials from ulnar sensory digit V and between palm to wrist with normal DUCN and normal distal motor latency from FDI and ADM with conduction block across elbow. This result would fall under the ulnar nerve entrapment across elbow in moderate grade affecting sensory nerves as well with motor entrapment across elbow. Our data didn’t indicate any result where ulnar sensory nerve showed low amplitude in digit V and between palm to wrist and DUCN with normal distal motor latency and normal conduction across elbow in FDI and ADM. In one case where digit V, palm to wrist and DUC were absent along with normal motor distal latency and normal conduction velocity across elbow in FDI and ADM. This result shows that patient had a local lesion at the ulnar side of the forearm that affect the sensory branch of ulnar nerve from forearm and below. This could be due to a local injury where only ulnar sensory nerve was affected and the motor nerve was preserved. 2 hands showed absent sensory potentials from digit V, palm to wrist and DUCN with normal distal motor latency and conduction block in FDI and ADM across elbow. This result falls in the ulnar nerve entrapment across elbow in severe degree group. Ulnar sensory nerve was severely damage which I discussed in detail in my other research paper which was published in https://www.peertechzpublications.com/articles/JNNSD-9 151.php#:~:text=Journal of Neurology, Neurological Science and Disorders where I suggested the grading of ulnar nerve entrapment across the elbow. 1 hand showed absent potentials in digit V, palm to wrist and DUC with normal distal motor latency, low amplitude at wrist and normal amplitude across elbow with normal CV across elbow. From the clinical history we found that this patient had a local hand injury in the ulnar nerve at the forearm causing complete axonontemesis of sensory branch and spare the fast motor fibre.
Despite the relatively a small region of involvements of ulnar nerve entrapment at or below wrist, it has wide range of clinical presentation that may result in frequent misdiagnosis. This new grading will help the Clinical Physiologist in diagnosing the level of entrapment very clearly. At the same time this new grading will support the surgeon in deciding the conservative treatment or the surgical treatment. Non -surgical treatment, including physiotherapy or steroid injection, should considered first. Surgical intervention should only be considered when decompression of ulnar nerve at wrist is indicated at the Guyons canal level.
Abbreviations:
Ulnar nerve entrapment (UNE), Ulnar nerve entrapment across wrist (UNEAW), Dorsal Ulnar cutaneous (DUC), Nerve Conduction Studies -NCS, Betsi Cadwaladr University Health Board -BCUHB, General Practices -GPs, Association of Neurophysiological Scientists - ANS, abductor polices braves - APB, First dorsal interosseous (FDI), sensory conduction velocity - SCV, conduction velocity -CV, Distal Motor Latency - DML, normal sensory amplitude - NSA, Sensory nerve action potentials -SNAP, normal motor amplitude - NMA, Motor nerve action potentials -MNAP, motor conduction velocity – MCV, Normal (N), Palm to wrist (P-W), across elbow (AC/Elbow), Abductor digiti minimi (ADM)
Declaration:
Ethics Approval: We confirm that we have read the Journal’s position on issues involved in ethical publication and affirm that this report is consistent with those guidelines.
Written Consent from participants:
A written consent was obtained from all participants and filed in patient notes and a copy kept in the department.
Consent for Publication:
Not Applicable
Availability of data and materials:
The datasets analyzed during the current study are not publicly available as they are held within patient records but are available from the corresponding author on request.
Competing Interests:
The authors declare that they have no competing interests.
Funding:
BCUHB funded this study for publication.
Author’s Contribution:
The Author contributed by the collection, analysis and interpretation of data and in writing the manuscript.
Acknowledgements:
The author would like to acknowledge and thank Dr Gareth Payne, and Dr. Bashir Kassam for their encouragement, guidance and help with this study.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
