
Research article | DOI: https://doi.org/10.31579/2578-8949/107
1 Ivan Ivanovic*h Gribanov. Candidate of Medical Sciences, board-certified physician, plastic surgeon, cosmetologist, Junior Research Assistant at the A.I. Burnazyan Federal Medical Biophysical Center of the FMBA of Russia, member of the Interregional Public Organization for Botulinum Therapy and Russian Societyof Plastic, Reconstructive and Aesthetic Surgery
2 Zagidat Narimanovna Konovalova. Candidate of Medical Sciences, neurologist at the Central Institute of Botulinum Therapy and State-of-Art Neurology, member of the Interregional Public Organization for Botulinum Therapy
*Corresponding Author: Ivan Ivanovich Gribanov. Candidate of Medical Sciences, board-certified physician, plastic surgeon, Junior Research Assistant at the A.I. Burnazyan Federal Medical Biophysical Center of the FMBA of Russia, Director General of the Center for Aesthetic Me
Citation: II Gribanov., Konovalova Z.N. (2023) Neurological Complications of Thread Lifting. Dermatology and Dermatitis. 7(3); DOI:10.31579/2578-8949/107
Copyright: ©2023 Ivan Ivanovich Gribanov, This is an open-access article distributed under the terms of The Creative Commons. Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 07 November 2022 | Accepted: 16 November 2022 | Published: 06 January 2023
Keywords: thread lifting; complications; neuropathy
State-of-art invasive cosmetic procedures in some cases can lead to the development of neurological complications, in particular neuropathy. Neuropathy can be manifested by sensory (pain), motor and autonomic disorders. Neurological complications of thread liftingare associated with injury to both sensoryand motor nerves;facial and trigeminal nerves are most commonly affected. In case of direct nerve injury with a needle, cannula or thread, acute neuropathy occurs. Compression nerve injury is associated with a delayed symptoms development. Clinical signs of sensory nerve injury may include paresthesia, dysesthesia, anesthesia, and neuropraxia.
Nerve endings completely restore within up to 6 months, but in some cases, the injury can be catastrophic. The article presentsthe authors’ personal clinical observations.
The increase in the numberof invasive procedures in cosmetology has led to an increasein the number of variouscomplications, which is associated with both high traumatism of the new methods and insufficient qualification of a specialist, as well as non-compliance with post- procedural protocols, anatomical features, as well as concomitant diseases[4, 7].
Thread techniques for correction of the age-related facial changes can be divided into two large groups. The first is the use of threads of various sizes and configurations for the reinforcement of the skin or the so–called ‘mesothreads’. The second is the use of threads with various types of offsets, notches with fixation to connective tissue structures — the so- called lifting threads. Both techniques are associated with the risk of undesirable effects and complications characteristic of invasive
methods — pain, hematomas, inflammation. Neurological complications (neuropathies) are particularly challenging.
Neuropathy is a disease of the peripheral nervous system characterized by an injury to the peripheral nerve fibers that make up various nerves. Neuropathy can be manifested by sensory (pain), motor and autonomic disorders [8]. Signs of nerve injury may vary in severity.In case of direct nerve injury with a needle, cannula or thread, acute neuropathy occurs. Compression nerve injury is associated with a delayedsymptoms development.
Neurological complications of thread liftingare associated with an injuryto both sensory and motor nerves. Facial and trigeminal nerves are most often affected, which is shown in the figure with indication of the most common directions of application of the lifting threads (Figure. 1) [4].
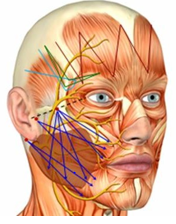
Figure: 1. The most common threadapplication patterns.
An injury to the structures of motor nerves causes partial or complete paralysis of the corresponding muscles [9]. The most serious are injuries to the facial nerve branches, since they cause paresis or plegia of the facialmuscles, facial asymmetryand serious functional and aesthetic defects.
In some cases, the facial nerve injuryis so serious that it can be considered seriousharm to the health and may lead to criminal liability of the doctor [10].Injuries to the frontal, buccal,zygomatic and the marginal mandibular branches of the facial nerve are most common [11]. In cases of an injury to the temporal branch of the facial nerve, the consequences may be permanent, since the frontal muscle does not have additional innervations [12, 13].
Thread lifting is most often performed in the buccal-zygomatic area and injuries to the zygomatic and buccal branchesof the facial nerve are most common [14].
The most dangerous anatomical area of the skin is limited by a triangle with the apex located on the zygomatic buttress and connected to the angleof mouth and the mandibular angle. During manipulations on the lower third of the face, there is a risk of an injury to the marginal mandibular branch, which innervates the depressor muscle of the angle of the mouth,depressor muscle of lower lip and mental muscle (Fig. 2) [2].
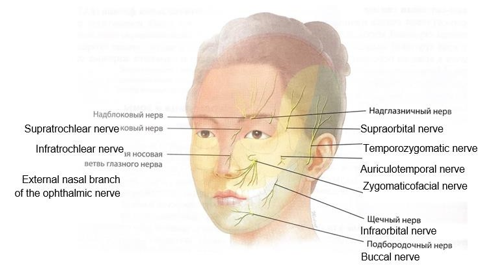
Figure: 2. Facial nervebranches exit points
Signs of an injury to the branchesof the sensitive trigeminal nerve include impaired sensation and pain of various severity [7, 15].
Thus, sensory nerve injuriesmanifest in the following forms:
Resolution of changes after the sensory nerve injuries usually occurs completely due to a sufficient number of sensory nerves over a period from several weeks to 6 months, but in some cases, complications can be catastrophic. A combination of motor and sensory disordersis also possible.
Anatomically, there are 8 dangerous areas associated with the invasiveprocedures (Fig. 3) [1]:

Figure: 3. Dangerousareas of the face.
The most common causes of an injury to the nerve endings during thread lifting are violations of the technique of thread application with non- compliance with the depthof implantation.
In addition, various specific anatomical features of the facial structures are possible — deficiency of subcutaneous fat and superficial course ofnerve trunks.
Threads parameters play an importantrole, since exceedingthe permissible thickness of the threads increases the risk of injury to the nerve trunks (Figure. 4)
Thread thickness can be measuredin the European metric or UnitedStates customary units (USP) systems. Both standards are used in Russia,the ratio betweenthem is as follows:

includes the following:
(Berocca, Neurovit).
As a rule, in case of partial injury to the nerve, its contusion with an instrument or thermal injury by the cautery, after 4 weeks the treatment effectwill be notable.
We present clinicalcases from our practice.
Patient A, 36 years old. Injury to the temporal branch of the facial nerve as a result of the thread lifting. (Fig.)
The patient underwent a procedure of thread lifting of the middle 1/3 of the face. A few days after the procedure, a break/tear of the thread on the rightside occurred, and an attemptto correct this complication resultedin the development of facial asymmetry. According to the doctor’s opinion,this situation was a result of an injury to the soft tissues of the face. He recommended watchfulwaiting for a period during which all undesirable changeswere supposed to resolve without treatment. After 1 month of
follow-up, right-sided facial neuropathy was diagnosed, and neurotropic therapy was started. It should be noted that all doctors with whom the patient communicated a) were professionals and the thread application procedure was technically correct, and b) they did their best to help the patient. Let’s analyse why an injury to the buccal branch of the facial nerve have occurred in this triangle? It is known that the buccal (third)branch innervates zygomaticmajor and minor muscles, levator labii superioris, levator anguli oris, buccal muscle, orbicularis oris, nasal muscle, risorius muscles. Their injury often occurs simultaneously, and given that the zygomatic and buccal branches have mutual connections, muscle paralysis is rarely total. Although, in some cases, persistent deformity is possible, which is difficult to correct. In what cases this situation is possible? Injury to the zygomatic and buccal branches of the facial nerve is possible during SMAS lifting, thread lifting, both at the time of application and extraction of threads, during Radiesse procedure, as well as botulinum neuroprotein injections [11, 14].

Figure: 4. Clinical case of an injury to the zygomatic and buccalbranches of the facial nerve
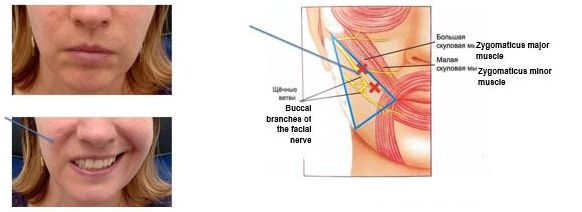
Figure: 5: Neuropathy of the buccaland zygomatic branches of the facialnerve after threadlifting
Patient I, 40 years old. Injury of the temporal branch of the facial nerve as a result of the thread lifting. (Fig.)
The patient underwent a thread liftingof the upper third of the face usingthe ‘Fox-Eye’ technique. 4 hours after the effect of anesthesia was supposed to finally resolve, on one side the eyebrow was mobile, and on the other side, mobility did not recover even within two weeks after the procedure. Upon admission neuropathy of the temporal branch of the facial nerve was diagnosed. The treatment was carried out according to the previously described protocol. Against the background of treatment,partial favourable changeswere noted. Currently, the treatment is ongoing, correction of the iatrogenic persistent deficiency is planned using thread liftingor surgical methods.
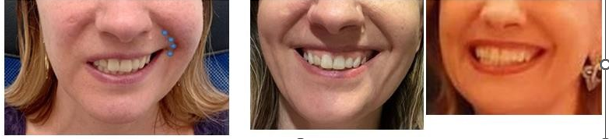
Figure: 6. Beforeand after botulinum toxin injections
Patient I, 40 years old. Injury of the temporal branch of the facial nerve as a result of the thread lifting. (Fig.)
The patient underwent a thread liftingof the upper third of the face usingthe ‘Fox-Eye’ technique. 4 hours after the effect of anesthesia was supposed to finally resolve, on one side the eyebrow was mobile, and on the other side, mobility did not recover even within two weeks after the procedure. Upon admission neuropathy of the temporal branch of the facial nerve was diagnosed. The treatment was carried out according to the previously described protocol. Against the background of treatment,partial favourable changeswere noted. Currently, the treatment is ongoing, correction of the iatrogenic persistent deficiency is planned using thread liftingor surgical methods.

Figure:7: Patient I, 40 years old. Injury of the temporal branch of the facial nerve as a result of the thread lifting procedure
Thus, facial nerve injury during thread lifting is a serious complication. Adequate and intensive treatment should be startedas soon as possible, in the near hours afterthe development of clinical signsto ensure restoration of functions and reduce the duration of the rehabilitation period. It is mandatory to conduct treatment in cooperation with the neurologist.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
