
Research | DOI: https://doi.org/10.31579/2642-973X/025
Emeritus Professor of Psychiatry, New York USA.
*Corresponding Author: Saeed Shoja Shafti, Emeritus Professor of Psychiatry, New York USA
Citation: Saeed Shoja Shafti. (2022). Neuroleptic Malignant Syndrome: Typical Antipsychotic Drugs Versus Atypical Antipsychotic Medications. Brain and Neurological Disorders 5(2); DOI:10.31579/2642-973X/025
Copyright: © 2022, S Shoja S, this is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 18 March 2022 | Accepted: 10 June 2022 | Published: 17 June 2022
Keywords: typical antipsychotic; atypical antipsychotic; neuroleptic malignant syndrome; schizophrenia
Introduction: Neuroleptic malignant syndrome is an idiosyncratic reaction and a severe disorder caused by an adverse reaction to drugs with dopamine receptor- antagonist properties and is characterized by a tetrad of rigidity, fever, altered mental status, and autonomic instability. In the present assessment, typical or conventional antipsychotics have been contrasted with atypical antipsychotics with respect to recorded cases of neuroleptic malignant syndrome among a sample of nonwestern psychiatric inpatients.
Methods: For assessment, all the cases with a diagnosis of neuroleptic malignant syndrome during the last sixty-two months, after exclusion of other conceivable differential diagnoses, were incorporated in the current retrospective, record-based evaluation. The clinical diagnosis was based on the Diagnostic and Statistical Manual of Mental Disorders, 5th edition. The valuation of independent variables was analyzed by ‘Compression of proportions. Statistical significance is defined as p value ≤0.05.
Results: Amongst 19814 psychiatric inpatients, in the course of sixty-two months, eighteen cases received the diagnosis of neuroleptic malignant syndrome. As said by the findings, neuroleptic malignant syndrome was meaningfully more frequent among males, in comparison with females, and it was importantly more prevalent among cases suffering from schizophrenia, in comparison with bipolar disorder. Also, the highest risk of neuroleptic malignant syndrome was found in the age group of 30-39. In the current assessment, only one of the patients, who had received haloperidol, died due to aspiration pneumonia and respiratory failure, and the most prevalent symptom was fever, which was observable in one hundred percent of cases. In addition to a similar clinical profile, ‘Compression of proportions’ did not show any significant difference between the conventional (typical) antipsychotics versus the atypical antipsychotic medications with respect to the occurrence of neuroleptic malignant syndrome.
Conclusion: As said by the findings, no significant difference was evident between the typical antipsychotic drugs versus the atypical antipsychotic medications, with respect to incidence and clinical profile of neuroleptic malignant syndrome.
Neuroleptic malignant syndrome (NMS) is an idiosyncratic reaction and a severe disorder caused by an adverse reaction to drugs with dopamine receptor-antagonist properties or the quick withdrawal of dopaminergic drugs [1]. It is characterized by a tetrad of rigidity, fever, autonomic instability, and altered mental status, ranging from confusion to coma, and later complications like renal and respiratory failure [2]. Moreover, it may be presented by leukocytosis, low serum iron levels and elevated creatine phosphokinase (CPK) levels [3, 4]. So, failure to diagnose NMS early and beginning of suitable management can result in serious medical complications and, finally, death. On the other hand, while diagnostic criteria for NMS are present, atypical presentations that lack one or more typical features pose a diagnostic problem to clinicians. Consequently, though controversial, the concept of atypical NMS has been suggested for such cases [5]. While there is no specific check able to diagnose NMS, serum creatine phosphokinase (CPK) elevation has been reported in over 90% of cases [6]. NMS happens most often during the first week of treatment or after increasing the dose of the antipsychotic drug [7]. The incidence of NMS is not well -known, but the rate of it's happening with typical antipsychotics has been reported to vary from 0.02% to 2.44% [8, 9]. In recent times, the frequency of NMS has declined from around 0.01% to 0.02% due to more alertness of clinicians and accessibility of newer antipsychotic drugs [10]. Primary reports of mortality rates from NMS were in excess of thirty percent, but increased physician attentiveness and institution of newer antipsychotic drugs over the last few years have reduced them to closer to ten percent [11]. While the underlying pathophysiologic mechanisms of NMS are complex and still under examination, perhaps a marked and sudden reduction in central dopaminergic activity resulting from D2 dopamine receptor blockade within the nigrostriatal, hypothalamic, and mesolimbic/ cortical pathways may explain the clinical features of NMS including rigidity, hyperthermia, and altered mental status, respectively [12]. The main risk factors for developing NMS are the commencement or escalation in dosage of an antipsychotic drug and the potency and administration form of that medication (13). Often complicating the diagnosis of NMS is the great number of drug-induced conditions that can have motor and cognitive features that are like NMS [14]. Also, though usage of antipsychotic medications is connected with a variety of adverse motor effects, several other classes of medications at toxic levels may cause symptoms similar to NMS [15]. Despite the fact that the risk of developing NMS due to atypical antipsychotics looks less than conventional neuroleptics, now the usage of atypical antipsychotics is increasing, so the frequency of NMS due to these medications may also increase [16, 17]. On the other hand, the introduction of atypical antipsychotics has further complicated the diagnosis of NMS, and it is supposed that atypical agents might cause atypical forms of NMS because of their different pharmacological properties [18]. Case reports and reviews propose that the clinical features of NMS associated with atypical medications differ from those precipitated by typical antipsychotics [19]. Atypical NMS is reported with the use of atypical antipsychotics such as clozapine, risperidone, aripiprazole, and olanzapine [20]. Therefore, the diagnosis of NMS remains controversial and presents an important challenge to physicians [5]. Nonetheless, while NMS is a diagnosis of exclusion, as a variety of medical disorders can present with analogous symptoms [21], early recognition and intervention are crucial because NMS can lead to severe complications, such as respiratory failure, rhabdomyolysis, seizures, acute kidney injury, and death [22]. In the present assessment, typical or conventional antipsychotics are compared with atypical antipsychotics with respect to recorded cases of NMS among a sample of non-western psychiatric patients.
Razi psychiatric hospital in the south of Tehran was selected as the field of research in the current retrospective evaluation. For appraisal, all the patients with a diagnosis of NMS during the last 62 months, after exclusion of other conceivable differential diagnoses, like serotonin syndrome, meningitis and encephalitis, were incorporated in the current examination. The clinical diagnosis, as well, was in line with the ‘Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5)’ [23].
Analysis of independent variables was performed by ‘comparison of proportions. Statistical significance is defined as P-value ≤0.05. ‘Med-Calc’ statistical software, version 15.2, was the statistical software tool for analysis.
As stated by results, among 19814 psychiatric patients hospitalized in the above-mentioned hospice, in the course of 62 months (April of 2013 - August 2018), 18 cases received the diagnosis of NMS. While 38.88% (n=7) of cases had received parenteral antipsychotics (haloperidol, IM or IV), 61.11% (n=11) of them had used only oral medications. According to the findings, NMS was meaningfully more frequent among male cases, in comparison with female patients, and it was importantly more prevalent among patients suffering from schizophrenia, in comparison with patients with diagnoses of bipolar I or II disorder (Table 1).

Also, while it was considerably more widespread amid the 18-65-year-old age-group, in comparison with adolescents or elderly patients (Table 1), the highest risk of NMS was found in the age group of 30-39, in comparison with 20-29 and 40-49 (Table 2). In the current assessment, only one of the patients, who had received haloperidol, died two weeks after the appearance of NMS due to aspiration pneumonia and respiratory failure (5.55%). Moreover, the most predominant clinical symptom was fever, which was palpable in all cases (mean total average = 39.71 ± 0.58 Celsius) (Table 3). The mean total days between admissions to the psychiatric ward and diagnosis of NMS was around 3.05 ± 2.54 days, and the mean total days of treatment for NMS was around 7.83 ± 6.11 days. Comparing the prescribed typical antipsychotics [haloperidol (n=9), thioridazine (n=1), chlorpromazine (n=1)] and atypical antipsychotics [olanzapine (n=4), risperidone (n=3)], ‘Compression of proportions’ did not display any statistically important difference between the conventional (typical) antipsychotics versus the atypical antipsychotic medications with respect to incidence of NMS (z = 1.33, p<0 xss=removed>
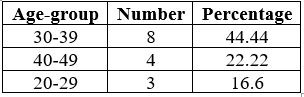
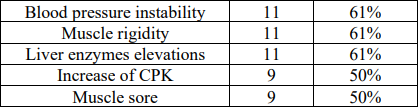
Table 3: Frequency of medical symptoms in NMS cases
Though NMS happens only infrequently, it remains an unpredictable and potentially deadly neurologic situation that clinicians must be able to diagnose as soon as possible, since early diagnosis and correct medical management are crucial to make sure of improved conclusions [24]. While incomplete or extraordinary NMS cases have been reported due to atypical agents, it should always be kept in mind that all atypical antipsychotic drugs, including clozapine, have the probability of inducing NMS, even though not a common phenomenon [25]. If NMS is not quickly identified and treated, it can be deadly due to cardiac arrest, pneumonia, pulmonary embolism, renal failure, disseminated intravascular coagulation or permanent damage, such as neurological sequels [3, 11]. Along with the findings of the present evaluation, there was no substantial difference between conventional and atypical antipsychotics with reference to prompting NMS, a finding which was rather in accord with the outcomes of Khouri et al. [7], Ananth et al. [26], Trollor et al. [18], Croarkin et al. [27], and Teo et al. [5]. Also, while the outcome of the current assessment was in agreement with the results of Khaldi et al. [28], who indicated that atypical antipsychotics can cause NMS even when prescribed in monotherapy, it was not in harmony with the outcome of Anzai et al. [29], who said that monotherapy or combination therapy with most atypical antipsychotic agents without typical antipsychotic agents was not likely to cause NMS as an adverse reaction compared to haloperidol monotherapy. So, as said by Ananth et al. [26], induction of NMS by clozapine, though not common and in incomplete or extraordinary forms [25], indicates that low incidence of extrapyramidal symptoms (EPS) and low EPS-inducing potential do not stop the happening of NMS, and D2 dopamine receptor blocking potential does not have direct association with the incident of NMS. In addition, in contrary to Teo et al. [ 5]) and Trollor et al. [18], who supposed that the advent of atypical antipsychotics has further complicated the diagnosis of NMS and atypical medications might cause atypical forms of NMS owing to their different pharmacological properties, and Sarkar et al. [19] and Pileggi et al. [30], who had stated that case reports and reviews suggest that the clinical features of NMS associated with atypical antipsychotics differ from that precipitated by typical antipsychotics, and drug re-challenge and follow-up care have not been underlined in many reports of NMS, in the current examination no uncommon exhibition of NMS that lacks one or more distinctive features was implicitly manifest due to atypical antipsychotics. Nevertheless, while the suggestion of Teo et al. [5] was concerning atypical NMS precipitated by quetiapine and clozapine overdoses, in the current evaluation, NMS was discernible with standard amounts of risperidone and olanzapine, which may show different symptomatology in comparison with the aforesaid medicines. So, our conclusion is a bit in accord with Trollor et al. [18], who believed that NMS accompanying atypical antipsychotic medications displays in a characteristic mode, except that clozapine-induced NMS, which appears less probable to present with extrapyramidal features, including rigidity and tremor [31, 32]. Also, in the present estimation, no delayed type of NMS, which, in the words of Suzuki et al. [33], might be relatively more frequent in senior and pre-senior patients than in younger patients, was manifest, and the mean total period between admission in the psychiatric ward and transmission to the ICU was around one week, which was in agreement with the outcomes of Chen et al. [3], who stated that two-thirds of cases of NMS develop within the first week. Similarly, since the only teenager in the current estimation had received olanzapine, so again our result is a little in harmony with the suggestion of Croarkin et al. [27], who indicated that adolescents can develop NMS during treatment with atypical antipsychotics and its symptoms are similar to those described in adults. Furthermore, in the present study, there was only one death due to NMS, which was induced by haloperidol; an outcome that was compatible with the finding of Ananth et al. (26), who believed that the mortality rate of NMS with atypical antipsychotic medications was lesser than conventional antipsychotic drugs. Nevertheless, the death rate may basically be a reflection of physicians' awareness and resulting from early treatment. Anyhow, while NMS is a life-threatening complication of antipsychotic drugs, and it is often assumed to be infrequent, observations suggest that, rather than overestimating its incidence, we are more likely to underrate it [34]. Even though less common now than in the past, because of greater alertness, it remains a risk in susceptible patients receiving typical or atypical antipsychotic medicines. Accordingly, decreasing the risk factors, early identification of suspected cases, and rapid management can meaningfully decrease mortality and morbidity in this hazardous situation. Cooperation between psychiatry and other medical fields may be the key to a fruitful consequence [34]. On the other hand, while routine examination of serum CPK in patients on antipsychotic medications who demonstrate features of NMS is endorsed to help diagnosis [35], diagnosis and appropriate treatment can be delayed when a patient does not present with classical signs of NMS [5]. So, the diagnosis of NMS should mainly be determined by clinical symptoms [2]. Though NMS can be hard to diagnose and it is a diagnosis of exclusion, we should remember that, since there is a great changeability re its clinical presentation, clinicians should not exclude this syndrome too quickly in a patient treated with neuroleptics [7]. Narrow periods of study, due to inapt recordings in the last span, and unsatisfactory cases with the diagnosis of NMS, as available samples, despite the size of the field of investigation, do not permit generalization of the results to more than a pilot study.
As said by the findings, no significant difference was evident between the typical antipsychotic drugs versus the atypical antipsychotic medications, with respect to incidence and clinical profile of neuroleptic malignant syndrome.
The author acknowledges physicians and personnel of Razi Psychiatric Hospital for their valuable support and assistance.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
