
Research Article | DOI: https://doi.org/10.31579/2690-4861/429
1 Departments of Psychiatry and Neurology, A. Martinos Center for Biomedical Imaging, Center for Morphometric Analysis, Massachusetts General Hospital, Harvard Medical School, Boston, MA, United States.
2 Department of Anatomy and Neurobiology, Boston University School of Medicine, Boston, MA, United States.
3 Psychiatric Neuroimaging Laboratory, Harvard Medical School, Brigham and Womens Hospital, Boston, MA, United States.
4 Department of Neuroscience, Psychology, Drug Research and Child’s Health (NEUROFARBA), University of Florence, 50135 Florence, Italy.
5 IRCSS SYNLAB SDN, 80143 Naples, Italy.
6 Department of Neuroscience and Biomedical Engineering, Aalto University, Helsinki, Finland.
7 Department of Psychiatry, University of Helsinki, Helsinki, Finland.
8 Center for Biomedical Engineering and Rehabilitation Sciences, Louisiana Tech University, LA 71272, USA.
9 Department of Clinical and Experimental Biomedical Sciences “Mario Serio” University of Florence, Florence, Italy.
10 Institute for Neuroscience, Florence, Italy.
11 Department of Psychiatry and Behavioural Science, Albert Einstein College of Medicine, Bronx, USA.
* Authors contributed equally.
# Corresponding Author
*Corresponding Author: Stefano Pallanti, Istituto di Neuroscienze Firenze, Via Alfonso la Marmora, 24, 50121 Florence, Italy
Citation: Nikos Makris, Gioele Gavazzi, Juan G. Prieto, George Papadimitriou, Carlo Cavaliere, et al, (2024), Neural Correlates of Reactive Inhibition in Gambling Disorder: An FMRI Study with Transcranial Magnetic Stimulation (TMS), International Journal of Clinical Case Reports and Reviews, 19(1); DOI:10.31579/2690-4861/429
Copyright: © 2024, Stefano Pallanti. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 26 March 2024 | Accepted: 23 August 2024 | Published: 06 September 2024
Keywords: gambling disorder and tbs; gambling disorder and functional connectivity; reactive inhibition; stop signal task
Gambling Disorder (GD) is a condition characterized by a persistent and recurrent pattern of problematic gambling behavior. Despite significant advances in understanding the neurobiological correlates of Gambling Disorder phenomenological manifestation, there are still several unanswered questions regarding the pathophysiological mechanisms underlying GD. There is substantial evidence from fMRI studies on the role of pre-SMA stimulation in psychiatric conditions with impairments in response inhibition such as behavioral addictions on enhancing the activity of the brain circuitry involving the right inferior (IFG) and middle frontal gyrus (MFG) (two cortical areas are differentially associated with two distinct aspects of control inhibition). In this study we utilized task-related functional Magnetic Resonance Imaging (fMRI) to explore the impact of continuous Theta-Burst Stimulation (cTBS) on the pre-Supplementary Motor Area (pre-SMA) in patients with Gambling Disorder (GD). Four GD patients underwent cTBS on bilateral pre-SMA, administered with the MagVenture MagPro R30 stimulator with add-on theta-burst option (MagVenture INC.) using a Cool D-B80 figure-of-eight coil. cTBS consists of bursts of 3 pulses separated by 20 ms (i.e., 50 Hz) delivered repeatedly at theta frequency on the pre-SMA bilaterally. Changes in Functional Connectivity (FC) were assessed before and after Real or Sham treatment using CONN functional connectivity toolbox and Statistical Parametric Mapping (SPM). The study aimed to determine whether cTBS influences the functional connectivity between pre-SMA and right prefrontal areas, specifically the right Inferior Frontal Gyrus (rIFG) and right Middle Frontal Gyrus (rMFG), and whether these changes correlate with treatment outcomes. Results indicated that real cTBS treatment increased functional connectivity between pre-SMA and both rIFG and rMFG, suggesting enhanced control inhibition. This was associated with a reduction in Gambling Disorder symptom severity, assessed with the Pathological Gambling version of the Yale-Brown Obsessive-Compulsive Scale (PG-YBOCS) and the Gambling Urges Questionnaire (GUQ), indicating a treatment response. Conversely, sham cTBS did not elicit the same positive FC changes in the reactive control inhibition network, aligning with behavioral measures. The study highlighted the potential of cTBS on pre-SMA in modulating inhibitory control circuit. Overall, this preliminary investigation provides a foundation for future investigations into the neurobiological mechanisms underlying GD and the potential efficacy of TMS interventions.
Gambling Disorder (GD) is a condition characterized by a persistent and recurrent pattern of problematic gambling behavior [2]. As a behavioral addiction, it can have significant negative consequences for individuals and their loved ones. Gambling is characterized by craving, altered functioning of the reward system and deficient inhibitory control [28]. Since the mid-1990s, several neuroimaging studies have shown structural and functional brain alterations in behavioral and substance-related addictions [5; 20; 21].
Functional MRI (fMRI) studies in particular, have identified dysregulation of reward processing in Gambling Disorder in core circuitry in the ventral striatum (VS, i.e., nucleus accumbens septi), medial prefrontal cortex (PFC) and orbitofrontal cortex (OFC), and other structurally and functionally affiliated regions such as the insula and dorsolateral PFC (DLPFC) [7]. In patients with GD, relative glucose metabolic rates (rGMR) in the OFC and medial frontal cortex were shown to be significantly increased at baseline compared to normal control [14]. Patients with GD had a decrement of the rGMR in the ventral parts of the striatum and thalamus, and an increment of the rGMR in the dorsal striatum and dorsal thalamus as compared to controls [26].
Despite significant advances in understanding the neurobiological correlates of Gambling Disorder phenomenological manifestation, there are still several unanswered questions regarding the pathophysiological mechanisms underlying GD. Recent studies have shown how Transcranial Magnetic Stimulation (TMS) can modulate various brain circuits [e.g., 3; 11]. Pre-supplementary cortex (Pre-SMA) in particular is currently used widely as an anatomical target for stimulation in psychiatric conditions with impairments in response inhibition such as behavioral addictions.
There is substantial evidence from fMRI studies on the role of pre-SMA in response inhibition as part of a brain circuitry involving the right PFC, namely the right inferior (IFG) and middle frontal gyrus (MFG) [e.g., 3; 10; 11]. It has also been proposed that these two cortical areas are differentially associated with two distinct aspects of control inhibition. Namely, the right IFG (rIFG) is associated with proactive inhibition, whereas the right Middle Frontal Gyrus (rMFG) is associated with reactive inhibition [e.g., 10]. Whereas there is substantial literature in basic neuroscience on this topic, clinical response inhibition studies using fMRI in GD are scant. A recent repetitive Transcranial Magnetic Stimulation (rTMS) fMRI study investigated the level of task-related pre-SMA activity and the propensity for impulsive risk-taking behavior in the context of sequential gambling and showed the importance of pre-SMA in integrating prefrontal and corticosteroid centers in motor control [19].
A pilot study by our group [28] has shown the efficacy of Theta-Burst Stimulation (TBS) of pre-SMA in reducing central Gambling Disorder symptoms, at least in the short term. More recently, in an original randomized, double-blind study [27] assessing the effect of MRI-guided continuous TBS (cTBS) of the pre-SMA for the treatment of GD, we reported a reduction in symptom severity among those receiving cTBS as compared to the placebo group; this was shown by the significant reduction of the Yale Brown Obsessive Compulsive Scale adapted for Pathological Gambling (PG-YBOCS) score after only 10 sessions of cTBS on the pre-SMA area along with that of Gambling Urges Scale (GUS) [28] .
In the present study, we used task-related fMRI functional connectivity (FC) to assess whether cTBS applied to pre-SMA bilaterally, has an effect on the right prefrontal network involving Inferior Frontal Gyrus (rIFG) and right Middle Frontal Gyrus (rMFG). We investigated task-related fMRI FC before and after TBS treatment applied on pre-SMA in a subsample of our larger cohort of patients affected by Gambling Disorder. Our guiding hypothesis was that TBS would affect the FC between pre-SMA and the two right hemispheric prefrontal areas, i.e., rIFG and rMFG, and that these changes would correlate with TBS treatment outcome in GD patients.
Four patients with a diagnosis of Gambling Disorder, assessed according the criteria of the 5th edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) [1] through a clinical interview with a licensed physician, were consecutively admitted at the Institute of Neuroscience (Florence, Italy). Participants were randomly assigned to active (continuous TBS over the pre-SMA bilaterally on the interhemispheric sulcus) or sham conditions. Random assignment was done by computerized random number generator. cTBS consists of a continuous sequence of bursts of 3 pulses separated by 20 ms (i.e., 50 Hz), which are presented at a theta frequency. Stimulus intensities were set at 80% of the resting motor threshold (rMT). Two trains of 600 pulses (a total of 1200 pulses) were given with an 8-second intertrain interval [29]. The bilateral pre-SMA was targeted using individual MRI and a neuronavigational system (SofTaxic Optic 2.0) (see Fig.1). The TBS treatment consisted of ten sessions of cTBS on bilateral pre-SMA. For further details on methods, see [29].
Participants were assessed by expert clinicians blinded to the treatment condition at the baseline and at the end of the treatment with the Pathological Gambling version of the Yale-Brown Obsessive-Compulsive Scale (PG-YBOCS; [25]) and the Gambling Urges Questionnaire (GUQ). In the PG-YBOCS scores of 0 through 4 are assigned according to the severity of the response (0 = least severe response, 4 = most severe response). Each set of questions is totaled separately as well as together for a total score. Whereas, in the Gambling Urges Questionnaire (GUQ) participants rate the six items using a scale ranging from 0 (“strongly disagree”) to 7 (“strongly agree”); scoring consists in adding up the values, so that higher scores indicate stronger gambling urges. Furthermore, participants were scanned before and after the ten-session TBS treatment.
All analyses were carried out with the software R. The Shapiro-Wilk test was performed to assess the normality of the data. Associations were assessed with the Pearson correlation analysis. All results were quoted as 2-tailed p values, with statistical significance set at p < 0 xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed>
For the fMRI Stop Signal Task, we employed a T2*-weighted echo-planar imaging (EPI) sequence (TR/TE = 3000/35 ms, FA = 90°, slice thickness = 3 mm, FOV = 240 mm × 240 mm). Two hundred two scans were acquired, for a total acquisition time of about 9 minutes [e.g. 34; 9]. Task- related fMRI: We used the stop-signal paradigm [18] to investigate response inhibition in a controlled laboratory setting. The Stop-Signal Task (SST) is a highly suitable and widely used paradigm for the study of response inhibition in clinical populations [34]. The time needed for the individual to process the stop response (stop-signal reaction time, SSRT), or stop-process latency, has been shown to be an important measure of the cognitive control processes involved in halting an action. The Stop Signal Task was based on Sharp et al [8]. Each trial started with a fixation cross for 350 ms, followed by some arrows pointing to the left or right direction for 1,400 ms and then a fixation cross for 3650 ms. Participants were requested to press one of two buttons depending on the Go stimulus direction (arrow). At irregular intervals and unpredictably for the participants, a Stop signal (red circle) was presented. In this case, participants were requested to attempt to inhibit their response to the Go signal. For the Stop trials, the initial delay between the Go and Stop signals was 300 ms. This delay was adaptively varied according to a staircase adaptive procedure every two Stop trials. If the cumulative accuracy exceeded 50%, the delay was increased by 34 ms; if it was less than 50%, the delay was decreased by 34 ms. The lower limit was set to 100ms. The entire protocol consisted of 100 trials: 70% Go, 20% Stop and 10% Rest trials [34]. fMRI functional connectivity (FC) was performed using CONN functional connectivity toolbox [36, 22] and Statistical Parametric Mapping (SPM) [30]). Anatomical localization of fMRI activation was performed using the Harvard-Oxford Atlas (HOA) [32]. In Figure 1, the pre-SMA (color-coded in turquoise green) is shown in a midsagittal section of HOA. In this study, cTBS was applied on bilateral pre-SMA.
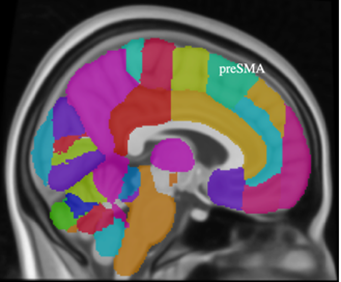
Figure 1: Anatomical localization of the pre-SMA shown in a midsagittal section of the Harvard-Oxford Atlas (HOA) [27].
The two patients in the active (‘REAL’) group, (i.e., patients NAP105 and NAP110) showed a reduction in Yale Brown Obsessive Compulsive Scale adapted for Pathological Gambling (PG-YBOCS) scores of at least 7 points (35%) (Table 1 and Table 2).
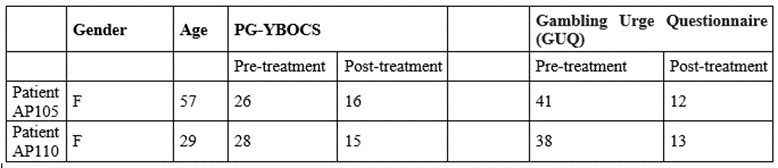
Table 1 – Neuropsychological assessment of patients assigned to the REAL condition.

Table 2 – Neuropsychological assessment of patients assigned to the SHAM condition.
Functional connectivity analysis showed that symptom severity, measured with PG-YBOCS was in agreement with fMRI-based functional connectivity observations in the cortical network involving the Inferior Frontal Gyrus (IFG) and Middle Frontal Gyrus (MFG) of the right prefrontal cortex. Specifically, both patients who received REAL TMS treatment targeted at bilateral pre-SMA showed an increase in FC between pre-SMA and IFG as well as MFG. This pattern of FC was observed in both the pre-TMS and post-TMS conditions (Figure 1). Furthermore, reduction in craving, measured with the Gambling Urges Questionnaire (GUQ), correlated with an increase in FC between bilateral pre-SMA and both right IFG and right MFG in the same patients. The two patients in the ‘SHAM’ group (i.e., patients NAP101 and NAP104) showed a different pattern of functional connectivity.
More specifically, whereas pre-SMA correlated positively with IFG and MFG in the pre-TMS treatment condition (Figure 2), a negative correlation (anticorrelation) was observed in the post-TMS condition concerning the right MFG (Figure 2). Thus, in the pre-TMS condition, pre-SMA correlated positively with right IFG in all patients, receiving ‘REAL’ and ‘SHAM’ treatment. Furthermore, in the pre-TMS condition, the pre-SMA correlated positively with right MFG in all patients, receiving ‘REAL’ and ‘SHAM’ treatment (Figure 2). Nevertheless, importantly, the FC of pre-SMA with the right MFG showed the opposite pattern in the ‘REAL’ (i.e., positive correlation) as compared to the ‘SHAM’ (i.e., negative correlation) group in the post-TMS condition.
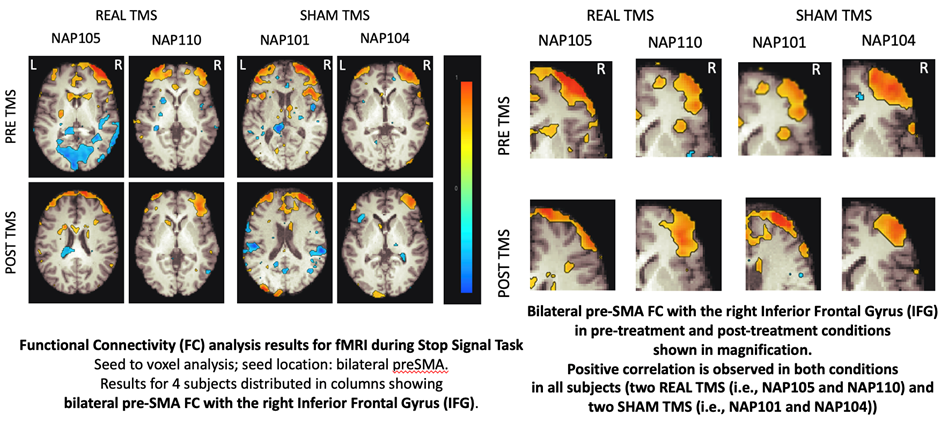
Figure 2
In this pilot study, we investigated changes in fMRI-based functional connectivity (FC) in gamblers treated with Theta-Burst Stimulation (TBS) on both left and right pre-Supplementary Motor Area (pre-SMA). We found that a reduction in symptoms severity was associated with an increase in FC in the prefrontal cortical network involving the Inferior Frontal Gyrus (IFG) and Middle Frontal Gyrus (MFG) of the right hemisphere.
Overall, all patients who received REAL TMS treatment targeting bilateral pre-SMA, showed an increase in FC between pre-SMA and IFG as well as MFG in both, the pre- and post-TMS conditions. This observation can be interpreted as an increase of both aspects of control inhibition. Specifically, proactive control inhibition was associated with the rIFG and reactive control inhibition was associated with the rMFG. These results indicate a treatment response in these patients in agreement with their behavioral measures. On the contrary, our fMRI-based FC observations in the patients receiving SHAM TMS showed that the reactive control inhibition network was negatively correlated in post-treatment, indicating a lack of treatment response. This is in agreement with the behavioral measures of these patients. Interestingly, the network related with proactive response inhibition involving the rIFG was similar in both the REAL and SHAM groups; it could be that proactive response inhibition may be related to craving, which is present in all patients, independently of receiving REAL or SHAM treatment.
Previous studies have shown that continuous Theta-Burst Stimulation (cTBS) over the pre-SMA modulates inhibitory control circuitries [23], by increasing cognitive shifting ability or improving decision-making [14]. Indeed, cTBS applied to the pre-SMA has been shown to increase the efficiency of inhibitory control over prepotent ongoing responses in healthy subjects [23] and in improving decision-making [34].
While research on the use of TMS, specifically TBS on the pre-SMA, in the treatment of Gambling Disorder has produced promising results, the etiological mechanisms and the associated brain structural and functional changes need to be deeply investigated. Further research is needed to better understand the optimal parameters such as target location, coil orientation and intensity, as well as long-term effects of TMS in this context. Nonetheless, the potential of TMS as a non-invasive and targeted treatment approach for GD offers hope for individuals seeking effective interventions for this challenging condition.
It should be pointed out that the present study is preliminary, given that the small size of the sample does not allow for meaningful statistical analyses. Nevertheless, in this case report, we tested a hypothesis that appears to have a reasonable basis in terms of the functional neuroanatomy of the prefrontal brain circuitry for control inhibition associated with the neural network involving the pre-SMA in patients affected by GD, which is an understudied clinical condition using fMRI functional connectivity. Although the sample size of the present study is low, the observations identified are consistent with published observations in basic and clinical neuroscience regarding response inhibition and motor control [e.g. 3; 10].
A recent review by Gavazzi and colleagues [10] with a large meta-analysis exploring the neural correlates of reactive inhibition emphasized the relevance of a model involving two distinct networks of control inhibition. These networks are contiguous areas in the right PFC, namely in the rIFG pertaining to proactive inhibition and in the rMFG associated with reactive inhibition. The presence of these two separate neural networks allowed the proposal of a novel model of cognitive control which is applicable in the cases of GD patients presented herein. In the two subjects with a reduction of the Yale Brown Obsessive Compulsive Scale adapted for Pathological Gambling (PG-YBOCS) score, the response to TMS activated only the network involved in reactive inhibition. It is important to point out, moreover, that another one limitation and potential bias of the study is related to gender. In fact, subjects in our study were all male. This, despite making our sample representative of the population of subjects with Gambling Disorder (predominantly male [13; 7]), makes it unrepresentative of the female gender. These preliminary results should be interpreted with caution; further studies on larger populations are needed before confirming this model; furthermore, different TMS targeting might work on a different dimension of GD. At any rate, this investigational strategy appears to have great potential in the understanding the GD and further improvement of the treatment approach. These preliminary case series results will serve as a pilot for future studies in larger patient populations testing the proposed hypotheses herein.
The increased activity of frontal areas, especially in the right hemisphere, found in the present study is in agreement with what has already been found in patients with Substance Use Addictions (SUDs) [38] and is consistent with a model that considers behavioral addictions similar to substance use addictions, in which reduced inhibitory control is a marker of vulnerability and severity of the disorder. However, although our study found effects only in the right hemisphere, in other works changes have been found bilaterally or in the left emisphere [16; 17]. This could be related to a specificity of Gambling Disorder to SUDs, however, it cannot be ruled out that it could also be due to the small sample size of our sample.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
