
Research Article | DOI: https://doi.org/10.31579/2768-2757/048
*Corresponding Author: Gosaye Tekelehaymanot Zewde, Department of Midwifery, Harar Health Science College, Harar, Ethiopia.
Citation: Gosaye T Zewde. (2022). Neonatal Sepsis and Associated Factor among Neonate Admitted in Nicu at Hiwot Fana Specialized University Hospital Harar Town, Eastern, Ethiopia 2020. J Clinical Surgery and Research, 3(4); DOI:10.31579/2768-2757/048
Copyright: © 2022, Gosaye Tekelehaymanot Zewde. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 21 March 2022 | Accepted: 04 April 2022 | Published: 25 April 2022
Keywords: neonate; sepsis; neonatal sepsis; harar; hiwot fana
Background:Neonatal sepsis is a condition defined as a clinical syndrome characterized by signs and symptoms of infection in an infant 28 days of life or younger. Neonatal sepsis is one of the major causes of neonatal morbidity and mortality especially in developing countries. Socio-demographic, maternal, neonatal and medical factors were associated with risk of infection. The clinical signs and symptoms of neonatal Sepsis are nonspecific and the confirmation of diagnosis is challenging and time consuming. Therefore, the diagnostic approach should be depends up on consideration of risk factors.
Objective: This study aimed to assess the prevalence and factors associated with neonatal sepsis among neonates admitted to neonatal intensive care unit at Hiwot Fana Specialize Hospital Harar, Ethiopia 2020.
Methods: Retrospective cross sectional registered data based study was conducted from February 7- February 25/2020 G.C. A total of 292 neonates cards was selected systematically from neonates admitted to Hiwot Fana specialize hospital at NICU. Data was collected using data extraction tool and checked for completeness and consistency then entered in to SPSS windows version 20.0 for analysis. Bivariate logistic and multivariate regression analysis was used to check existence of association of each independent variable with the outcome variable and Variables significant in bi-variate analysis (P< 0.25) was entered to a multivariate logistic regression model and statistical significance was declared at P < 0.05. Odds ratios along with 95% Confidence interval were used to measure strength and to assess the presence of statistically significant association between independent variables and outcome variable.
Result: The prevalence of Neonatal Sepsis was 52.7%. From these 92.2% and 7.8% 0f Neonates developed Early and Late Neonatal sepsis respectively. Among them 59.7% were males. The study found that, Rural residence, delivery place, Meconium stained amniotic fluid, ANC follow up, Gestational age, birth asphyxia and 5th minute APGAR score <7 were significantly associated with neonatal sepsis.
Conclusion: The prevalence of neonatal sepsis was 52.7%. Rural residence, Hospital delivery, Meconium-stained Amniotic Fluid, ANC follow up, Gestational Age <37 weeks, birth asphyxia and 5th minute APGAR score <7 were found to statistically significant with Neonatal sepsis.
Sepsis is defined as systemic inflammatory response syndrome resulting from a suspected or proven infection [1]. Neonatal sepsis is a serious blood bacterial infection in neonate at the age equal to or less than 28 days of life which is manifested by systemic signs and symptom of infection. It was characterized by systemic result from bacterial invasion and multiplication in the blood stream [2, 3]. Based on the onset it can be classified as early-onset infection (if the onset of clinical feature present from birth to 7 days usually <72 hr) and late-onset infection (if it present from 8 to 28days after birth [4]. clinical presentation are non-specific and includes: fever, respiratory distress, lethargy, impaired or refusal of feeding, jaundice, absent Moro reflex, hypothermia, convulsions, bleeding disorder and bulging fontanel [5]. A number of neonatal risk factors were identified those play an important role in the occurrence of neonatal sepsis such as: male sex, preterm delivery, gestational age, birth asphyxia, low birth weight; <2.5kg, APGAR score less than seven in the first one minute, mechanical ventilation, and prolonged rupture of membranes have significant roles in early and late onset neonatal sepsis, as they do in resource-rich countries [6].
Globally neonatal sepsis is one of the most significant causes of morbidity and mortality among neonates during the neonatal period (0-28 day). Out of 5.9 million child deaths in 2015, almost 1 million occur in the first day of life and close to 2 million occurs in the first week of life. The main causes of neonatal deaths were preterm birth complications (35%), intrapartum related complications (24%), and (15%) sepsis [7]. Approximately four million global neonatal deaths occur per year, of which about 98 % occurs in developing countries especially in sub-Saharan Africa [8]. According to 2011 unique report neonatal deaths accounted for 52% of all under five child mortality, in South Asia, 53% in Latin America and Caribbean 34% in sub-Saharan Africa [9]. According to EDHS 2019 the neonatal mortality rate (NMR) in Ethiopia was 30/1000 live births, which has not shown significant reduced from the 2005 EDHS report of 39/1000 live births. Neonatal conditions which were causing under-five mortality in 2004 have currently increased to 43%. Out of these conditions which cause under five mortality, neonatal sepsis accounts 9% [10]. Identification of the bacteria and treatment was often unsatisfactory due the non-specific clinical presentation of sepsis and the lack of reliable diagnostic tests [11]. so that, if there was a delay in diagnosis, there will be dalliance in starting the treatment which increases the mortality rate by 50 %. Therefore, to avoid this problem, knowledge about common risk factors of neonatal sepsis in a given area becomes essential in guiding local empirical choice of antibiotics and to prevent drug resistance [12]. As indicated by many studies conducted in developed and developing country show that sepsis become highly varies geographically, from Hospital to Hospital in developed and developing country and even from room to room. So there must be periodic assessment of the problem in each location, due to this reason assessment of prevalence and associated factors of neonatal sepsis among neonates admitted in neonatal intensive care unit at Hiwot Fana Specialized University Hospital is needed.
Significance of the study: The result of this study will be help the Programmers /planner and other responsible body in order to produce reference-based plan to prevent neonatal sepsis and it will be used as a base line data for other researchers. The study will provide insight to health care provider in identification common risk factors of neonatal sepsis and to overcome the Challenge of early diagnosis and management of sepsis.
General objective
To assess Neonatal sepsis and associated factor among neonate admitted in NICU at Hiwot Fana Specialize University Hospital Harar Eastern Ethiopia 2020.
Specific objective
To determine prevalence of neonatal sepsis among neonate admitted in NICU at Hiwot Fana Specialize University Hospital Harar Eastern Ethiopia 2020
To identify factor associated with neonatal sepsis among neonate admitted in NICU at Hiwot Fana Specialize University Hospital Harar Eastern Ethiopia 2020
Study area and period: Harar Town is one of the ten regional states of the Federal Democratic Republic of Ethiopia located in the Eastern part of the country at 526 km away from Addis Ababa, the capital city of Ethiopia. The study was conducted in HFSU which was established in 2006 and providing service for more than 5 million people in the catchment area. It is the only teaching and referral hospital in Harar city. It had major clinical departments like internal medicine, surgery, pediatrics, and gynecology/obstetrics and also has other clinical departments like, dentistry, ophthalmology, psychiatry, anesthesia, and dermatology. The study was conducted from February 7- 25/2020 G.C.
Study design: An institutional based retrospective cross sectional study design was
Source population
The source population was all neonates card who were admitted and treated in Hiwot Fana Specialize University Hospital Neonatal intensive care unit from July 2018 to June 2019 G.C.
Study population
Study population was randomly selected neonatal cards who were admitted and treated in Hiwot Fana Specialize University Hospital Neonatal intensive care unit from July 2018 to June 2019 G.C.
Inclusion criteria: All neonates admitted cards and age equal to or less than 28 days who was admitted to the NICU of HFSUH.
Exclusion criteria: Neonates card with incomplete patient chart information.
Sample Size Determination: Sample size was determined by the formula of single (P = Prevalence of neonatal sepsis at Shashemene, study 77.9%) [37]. And double population proportion formula (P1=33.1 % and P 2= 51.6%, 95%, margin of error of 5 % and power of 80%, and using Open Epi Info7) [34] then comparing the first and second objective after adding 10% for missing data the final sample size was 292.
Sampling technique and procedure:
List of one year admitted neonates were taken from the database and K value was calculated as, K=N/n→1461/292=5 and systematic random sampling techniques was used to select the sample by every kth interval according to the registration order and the first number was selected by lottery method.
Dependent Variable
Neonatal Sepsis
Independent Variables: Socio-demographic [Age, Sex, Residence, Place of delivery]
Maternal factors/delivery factors [Parity, Mode of delivery, maternal diseases] Neonatal factors [Birth weight, Prematurity]
Operational definitions
Inborn: Neonate who was born at maternity ward of HFSUH and admitted to NICU of hospital.
Out born: Those neonates born out of HFSUH and admitted to NICU ward from other hospital
Neonatal Sepsis: It is serious blood bacterial infection in neonate at the age equal to or less than 28 days of life admitted in NICU of HFSUH.
Data collection tools and procedures: After reviewing of relevant literature, data extraction tool was developed which was used to obtain information on socio-demographic factors, maternal/neonatal factors and disease distributions. Three diploma nurses who had trained were used as data collectors and data’s was extracted by reviewing patient’s chart.
Data Processing and Analysis: After data collection each questionnaire was checked its completeness, consistency on daily bases. Epi-Data version 3.1 and SPSS version 21 were used for data entry and analysis. P value < 0>
Multiple logistic regression analysis were used for better prediction of determinants and P - value less than 0.05 was declared as statistically significant.
Data Quality Assurance: To assure the quality of the data, pretest was done and training was given for data collector’s supervisor and data entry clerks prior to the study. Every day, the collected data were reviewed for completeness, consistency and legibility. Supervision was frequently made by supervisors together with the principal investigator.
Ethical consideration: Ethical clearance letter was obtained from Harar Health science College ethical research review committee and submitted to HFSUH CEO and consent was obtained from hospital CEO and Permission was obtained from study institution and confidentiality of information had been maintained.
Socio-demographic Characteristics: A total of 292 cars were reviewed out of this 181 (62%) were male neonates and 264 (90.4%) were admitted in less than 7 days of their birth. Majority 228 (67.1%) and 176 (60.3%) of neonates lives outside of Harar town and delivered at hospital (Table 1).
| Characteristics | Frequency | Percent | |
| Age | 0-7 days | 264 | 90.4 |
| 8-28 days | 28 | 9.6 | |
| Sex | Male | 181 | 62 |
| Female | 111 | 38 | |
| Place of Residence | In Harar Town | 96 | 32.9 |
| Out of Harar Town | 196 | 67.1 | |
| Place of delivery | In born | 176 | 60.3 |
| Out born | 116 | 39.7 | |
Table 1: Socio-demographic Characteristics of neonates admitted in NICU of HFSUH, Harar, Eastern Ethiopia, 2020 (n=292).
Prevalence of Neonatal Sepsis
The major morbidity profile among all neonates was Neonatal sepsis which accounted 154 (52.7%) followed by Perinatal Asphyxia 65 (22.3%) and Meconium Aspiration Syndrome 27 (9.2%) (Figure 1)
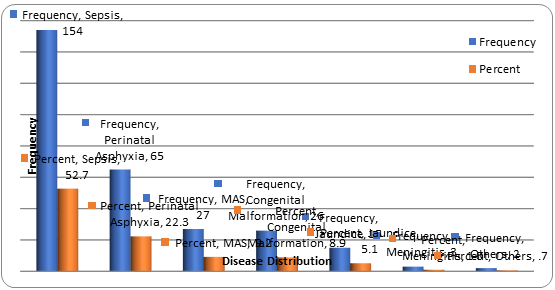
Figure 1: Distributions of diseases of neonates admitted in NICU of HFSUH, Harar, Eastern Ethiopia, 2020 (n=292).
Maternal Factors: From 292 samples included in the study nearest to half, 123 (42.1%) were born from mothers age between 25-30 years. One hundred seventieth 170 (58.2%) of mothers were multigravida and 174 (59.6%) of mothers had ANC follow up during their pregnancy. Concerning mode of delivery 173 (59.2%) was gave birth through SVD and 80 mothers had faced meconium stained amniotic fluids.
Neonatal Factors: In the study 262 (90.4%) neonates were developed Early Onset of Sepsis and 185 (63.4%) new born had developed birth asphyxia among this 160 (54.8%) were with 5th minute APGAR < 7 and resuscitated. Concerning their gestational age, 203 (69.5%) were delivered at term. Majority 180 (61.6%) of them birth weight was between 2.5 – 4kgs.
Factors Associated with Neonatal Sepsis: In multivariate analysis rural residence, place of delivery, Meconium stained amniotic fluid (MSAF), ANC follow up, GA, birth asphyxia and 5 th minute APGAR score <7 were significantly associated to neonatal sepsis. Neonates come from rural area were 2times times [AOR=2.908 95% CI: (1.718, 4.920)] more likely acquired neonatal sepsis than to those who live in urban. The risk of having neonatal service among neonates who delivered in the hospital were 2 times [AOR= 1.778 95% CI: (1.079, 2.930)] more likely than out born. Neonates born from mothers who have no ANC follow up were 2 times [AOR= 2.291, 95% CI: (1.267, 4.145)] more likely having neonatal sepsis than Having ANC follow up. Neonate whose delivery less than 37 weeks had 62% less likely [AOR= 0.038, 95% CI: (0.014, 0.103)] having the risk of acquiring sepsis. The odds of having neonatal sepsis is 7 times [AOR= 6.851, 95% CI: (1.720, 27.291)] more likely among Neonates with 5th minute APGAR score < 7 than their encounters. (Table 2)
| Characteristics | Neonatal Sepsis | Crude OR (95%) | P Value | Adjusted OR (95%) CI | |||||||||
| No | Yes | ||||||||||||
| No (%) | No (%) | ||||||||||||
| Age of Neonate | |||||||||||||
| 0-7 days | 122 (88.4) | 142(92.2) | 1.552 (0.707,3.408) | 0.581 | 1.268 (0.546, 2.947) | ||||||||
| 8-28 days | 16(11.6) | 12(7.8) | 0.75 | ||||||||||
| Sex of Neonate | |||||||||||||
| Male | 89 (64.5) | 92 (59.7) | 0.817 (0.508-1.313) | 0.577 | 0.866 (0.522, 1.436) | ||||||||
| Female | 49 (35.5) | 62 (40.3) | 1.265 | ||||||||||
| Place of Residence | |||||||||||||
| Urban | 64 (46.4) | 32 (20.8) | 0.500 | ||||||||||
| Rural | 74 (53.6) | 122 (79.2) | 3.297 (1.974, 5.509 )* | 0.000 | 2.908 (1.718,4.920)** | ||||||||
| Place of Delivery | |||||||||||||
| Inborn | 70 (50.7) | 106 (68.8) | 2.145 (1.331,3.457)* | 0.024 | 1.778 (1.079,2.930)** | ||||||||
| out born | 68(49.3) | 48 (31.2) | 0.706 | ||||||||||
| Maternal Age | |||||||||||||
| <19> | 8 (5.8) | 8 (5.2) | 1.105 (0.347, 3.526) | 0.531 | 0.629 (0.147, 2.684) | ||||||||
| 20-24 years | 49 (35.5) | 51 (33.1) | 1.150 (0.552, 2.397) | 0.556 | 0.754 (0.295, 1.929) | ||||||||
| 25-29 years | 55 (39.9) | 68 (44.2) | 1.367 (0.668, 2.794) | 0.794 | 1.114 (0.495, 2.505) | ||||||||
| 30-35 years | 5 (3.6) | 8 (5.2) | 1.768 (0.493, 6.348) | 0.327 | 2.225 (0.450, 11.003) | ||||||||
| >35 years | 21 (15.2) | 19 (12.3) | 0.905 | ||||||||||
| History of ANC follow up | |||||||||||||
| No | 71 (51.4) | 103 (66.9) | 1.906 (1.187, 3.060)* | 0.006 | 2.291 (1.267, 4.145)** | ||||||||
| Yes | 67 (48.6) | 51 (33.1) | 0.761 | ||||||||||
| History of maternal fever | |||||||||||||
| No | 124 (89.9) | 136 (88.3) | 1.097 | ||||||||||
| Yes | 14 (10.1) | 18 (11.7) | 1.172 (0.560, 2.456) | 0.884 | 1.072 (0.422, 2.724) | ||||||||
| History of foul smelling liquor | |||||||||||||
| No | 128 (92.8) | 146 (94.8) | 1.141 | ||||||||||
| Yes | 10 (7.2) | 8 (5.2) | 0.701 (0.269, 1.831) | 0.564 | 0.675 (0.177, 2.569) | ||||||||
| History of Chorioamniotis | |||||||||||||
| No | 128 (92.8) | 147 (95.5) | 1.148 | ||||||||||
| Yes | 10 ( 7.2) | 7 (4.5) | 0.610 (0.225, 1.648) | 0.138 | 0.320 (0.071, 1.443) | ||||||||
| Meconium Stained Amniotic Fluid | |||||||||||||
| No | 111 (80.4) | 101 (65.6) | 0.91 | ||||||||||
| Yes | 27 (19.6) | 53 (34.4) | 2.157 (1.262, 3.688)* | 0.001 | 2.752 (1.508, 5.023)** | ||||||||
| History of Prolonged Rupture of Membrane | |||||||||||||
| No | 121 (87.7) | 129 (83.8) | 1.066 | ||||||||||
| Yes | 17 (12.3) | 25 (16.2) | 1.379 (0.710, 2.680) | 0.09 | 2.047 (0.893, 4.694) | ||||||||
| Duration of Rupture of Membrane | |||||||||||||
| < 18> | 30 (21.7) | 43 (27.9) | 1.359 (0.786, 2.349) | 0.89 | 1.047 (0.549, 1.997) | ||||||||
| > 18 hours | 17 (12.3) | 15 (9.7) | 0.836 (0.395, 1.773) | 0.462 | 0.720 (0.300, 1.727) | ||||||||
| Intrapartum | 91 (65.9) | 96 (62.3) | 1.055 | ||||||||||
| Parity | |||||||||||||
| Primigravida | 58 (42.0) | 64 (41.6) | 0.981 (0.616, 1.563) | 0.854 | 0.939 (0.480, 1.836) | ||||||||
| Multigravida | 80 (58.0) | 90 (58.4) | 1.125 | ||||||||||
| Mode of delivery | |||||||||||||
| Spontaneous Vaginal Delivery | 80 (58.0) | 93 (60.4) | 3.487 (0.913, 13.324) | 0.097 | 3.371 (0.803, 14.143) | ||||||||
| Cesarean Section | 49 (35.5) | 58 (37.7) | 3.551 (0.911, 13.847) | 0.07 | 3.816 (0.896, 16.258) | ||||||||
| Instrumental | 9 (6.5) | 3 (1.9) | 0.333 | ||||||||||
| Duration of Labor | |||||||||||||
| <6> | 53 (38.4) | 65 (42.2) | 1.226 | ||||||||||
| 6-12 hours | 41 (29.7) | 34 (22.1) | 0.676 (0.378, 1.210) | 0.152 | 0.611 (0.311, 1.200) | ||||||||
| Previous maternal use of medication | |||||||||||||
| No | 43 (31.2) | 44 (28.6) | 0.871 (0.524, 1.450) | 0.526 | 0.835 (0.147, 2.684) | ||||||||
| Yes | 9 (6.5) | 9 (5.8) | 0.851 (0.324, 2.241) | 0.654 | 1.336 (0.377, 4.734) | ||||||||
| Unknown | 86 (62.3) | 101 (65.6) | 1.174 | ||||||||||
| Previous maternal use of medication | |||||||||||||
| No | 43 (31.2) | 44 (28.6) | 0.871 (0.524, 1.450) | 0.526 | 0.835 (0.147, 2.684) | ||||||||
| Yes | 9 (6.5) | 9 (5.8) | 0.851 (0.324, 2.241) | 0.654 | 1.336 (0.377, 4.734) | ||||||||
| Unknown | 86 (62.3) | 101 (65.6) | 1.174 | ||||||||||
| Diagnosis on Admission | |||||||||||||
| EONS | 122 (88.4) | 142 (92.2) | 1.552 (0.707, 3.408) | 0.44 | 1.517 (0.526, 4.371) | ||||||||
| LONS | 16 (11.6) | 12 (7.8) | 0.750 | ||||||||||
| Birth weight | |||||||||||||
| LBW <2> | 30 (21.7) | 64 (41.6) | 10.667 (2.869, 39.662) | 0.118 | 3.248 (0.742, 14.217) | ||||||||
| NBW 2.5-4 kg | 93 (67.4) | 87 (56.5) | 4.677 (1.309, 16.716) | 0.173 | 2.665 (0.652,10.900) | ||||||||
| Macrosomia >4kg | 15 (10.9) | 3 (1.9) | 0.200 | ||||||||||
| Gestational Age | |||||||||||||
| Preterm <37> | 5 (3.6) | 83 (53.9) | 0.032 (0.012, 0.082)* | 0.000 | 0.038 (0.014,0.103)** | ||||||||
| Term 37-42 wks | 133 (96.4) | 70 (45.5) | 16 | ||||||||||
| Post term >42 wks | 0 (0.0) | 1 (0.6) | 1.000 | ||||||||||
| Birth Asphyxia | |||||||||||||
| No | 71 (51.4) | 36 (23.4) | 0.507 | ||||||||||
| Yes | 67 (48.6) | 118 (76.6) | 3.473 (2.105, 5.731)* | 0.000 | 12.979 (3.240,51.996)** | ||||||||
| 5th minute APGAR score | |||||||||||||
| >= 7 normal | 74 (53.6) | 58 (37.7) | 1.500 | ||||||||||
| < 7resuscitation> | 64 (46.4) | 96 (62.3) | 0.523 (0.328, 0.834)* | 0.006 | 6.851 (1.720,27.291)** | ||||||||
Table 2: Bivariate and Multivariate analysis of variables and Neonatal Sepsis of neonates admitted in NICU of HFSUH, eastern Ethiopia, 2020 (n=292)
This study showed that sepsis was the frequently occurring disease among neonates admitted in NICU the finding was similar with study conducted at BPKIHS, Tamale, Nepal and Mandaya [13, 14, 16, 19] but not in line with study conducted in Pakistan and St. Paul’s [17, 21], Imperial college England [15] and Haryana [18]. This deference might be due to deference in socio-demography as well as study area. In this study, the dominant sex was Male 59.7 % and 92.2% of cases were age between 0-7 and the remaining 7.8 % were age 8-28 days. This finding was similar with the study conducted in Tamale, Mandaya, kwazulu-Natal, Shashemene, India, and Wolaita Sodo, [14, 19, 20, 23, 24, 33]. Rural residence was found significantly associated with Neonatal Sepsis in this study this is consistent with study conducted at Gonder referral hospital [26]. Neonates delivered with meconium-stained amniotic fluid was found significantly associated with Neonatal sepsis this is consistent with study conducted at Washington DC, Mexico and Karachi hospital of Pakistan [27, 29, 31] where as regarding delivery site Neonates delivered in the hospital (Inborn) were found significantly associated with Neonatal sepsis. This is in line with study conducted at Cairo hospital of Egypt [22]. Neonates delivered from mothers who had not ANC follow up were found significantly associated with Neonatal sepsis. This is in line with study conducted at Texas and Gitwe of Rwanda [28, 32]. Regarding gestational age Neonates of gestational age < 37>
The study revealed that neonatal sepsis (52.7%), Perinatal Asphyxia (22.3%) and Meconium Aspiration Syndrome (9.2%) were the frequently occurring neonatal diseases. Rural residence, place of delivery (inborn), Meconium stained Amniotic Fluid, ANC follow up, Gestational Age < 37 weeks, birth asphyxia and 5th minute APGAR score < 7 were found to statistically significant for the prevalence of Neonatal sepsis. Recommen
For Health Institutions
For Those Health Professionals Who Are Working in NICU and Obstetric Unit
The findings of this study should be interpreted in the light of a number of limitations. Firstly, since it is a retrospective study institutional and health professional factors were not included. Secondly the study was cross-sectional it did not address the cause and effect of the factors. Thirdly the study reviewed data of one year only.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
