
Research Article | DOI: https://doi.org/10.31579/2578-8965/179
1Medical graduate, School of Medicine, Shahed University, Tehran, Iran
2Department of Pediatrics, Assistant Professor, Faculty of Medicine, , Shahed University, Tehran, Iran
3Department of Obstetrics and Gynecology, Assistant Professor, Faculty of Medicine, , Shahed University, Tehran, Iran.
*Corresponding Author: Maryam Rabiee, Department of Obstetrics and Gynecology, Assistant Professor, Faculty of Medicine, Shahed University, Tehran, Iran.
Citation: Rayhaneh Mahroo, Shiva Rafatie, Maryam Rabiee, (2023), Neonatal Complications in Mothers with Severe Complications or Near-Miss Cases, J. Obstetrics Gynecology and Reproductive Sciences, 7(7) DOI:10.31579/2578-8965/179
Copyright: © 2023, Maryam Rabiee. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 18 July 2023 | Accepted: 28 September 2023 | Published: 18 October 2023
Keywords: severe complications; near miss; neonatal; maternal
Background: Maternal complications, particularly maternal near death, may also contribute to the increase in perinatal complications. Consequently, this study investigated the correlation between neonatal complications in mothers with severe pregnancy complications and near-miss cases.
Methods: This cross-sectional study was conducted on mothers who gave birth between March 2017 and March 2019 at a Medical Training Hospital and a Private Hospital in Tehran and experienced severe maternal complications or life-threatening conditions. The characteristics of mothers and infants were recorded. Statistical tests were employed to analyze the data (p˂0.05).
Resulting: This study evaluated 138 mothers with severe complications, where 32.6% exhibited near-death conditions. The most common causes of severe maternal outcomes were preeclampsia and severe bleeding (50.7% and 36.2%, respectively). Of newborn 48.2% experienced prematurity, 35.6% had low birth weight. 59.9% of the newborns of the mothers who were studied experienced at least one complication. 61.9% infants had respiratory failure, and 14.2% had a severe infection. The neonate mortality rate was 3%, while the stillbirth rate was 3.6%. Although linear/ binomial logistic regression test was not showed the correlation between the mother’s demographic characteristics and perinatal complications but one third of mothers with the underlying disease had neonatal complications and the likelihood of prenatal complications is higher in multiparous women over 30.
Conclusion: In severe maternal complications, neonatal complications, prematurity and low birth weight, are more prevalent. Consequently, it appears necessary to equip hospitals with intensive care units and trained personnel who can provide adequate support for mothers and infants.
Pregnancy is one of the most vulnerable times in a woman’s life, and 15% of pregnant women are at risk of death [1, 2]. Typically, mothers’ and infants’ health are intertwined, and the mother’s condition during pregnancy and childbirth influences perinatal outcomes. Perinatal outcomes refer to the life events that occur to a newborn child between the age of viability (i.e., after 28 weeks of gestation) and the first week of life. According to studies, maternal complications, especially near-miss mothers, are associated with a greater likelihood of adverse perinatal outcomes [2,3].
The World Health Organization (WHO) also reported an increased perinatal mortality risk in maternal complications [4]. Severe pregnancy-related complications, potentially life-threatening conditions, are identified based on the presence of a severe complication, such as severe postpartum hemorrhage, severe preeclampsia, eclampsia, sepsis, or severe systemic infection, ruptured uterus, or receipt of a critical intervention (e.g., admission to intensive care unit, laparotomy, interventional radiography and use of blood products). Based on the identification of organ dysfunction by clinical, laboratory, and management markers, some women are categorized as “near-miss” [5]
Cases of a maternal near-miss, i.e., a complication that occurred during pregnancy, childbirth, or during the 42 days after the termination of pregnancy in which the patient was very close to death but survived, can occur up to 100times more frequently than maternal deaths and are currently used to evaluate the care provided by hospitals [6-9]. Consequently, severe maternal complications, particularly near-misses, may also contribute to the increase in perinatal complications, and its association with adverse perinatal events is anticipated. In addition to an increased risk of stillbirth, newborns of women with near misses have an increased risk of dying within the first week of life, necessitating hospitalization in an intensive care unit (ICU) and asphyxia [2, 7, 10]. However, little is known about the relationship between severe maternal morbidity, serious neonatal complications, and early neonatal death. Similarly, the predictors of neonatal mortality and the prognostic factors of neonatal near-misses remain unknown [7].
On the other hand, it is noteworthy that most life-threatening obstetrics are unavoidable and unfortunately unpredictable and depend on several variables directly related to the mother and fetus and the quality of care, particularly during prenatal periods (8, 10). In fact, race and socioeconomic status also play a significant role in the occurrence and treatment of pregnancy and newborn complications. African-American women in the United States, for instance, experience more maternal and fetal complications, such as preterm birth and lower birth weight, compared to white-American women. Significant causes of this difference include occupational factors, prenatal control delays, poverty, and language barriers [9, 11, 12] In addition to maternal complications, general socio-demographic and neonatal characteristics also contributed to neonatal survival. Therefore, many factors may be modifiable if efforts are made to improve the socioeconomic status of the community [3].
In recent years, the maternal mortality rate in Iran, a middle-income Asian country, has decreased significantly to 23 per 100,000 live births, and reproductive health indicators have improved. The total fertility rate is 1.9% per woman, antenatal care coverage and skilled attendance at birth are both at 98%, and institutional delivery is prevalent (14). In Iran, studies on maternal mortality and near-death have been conducted, but studies on these mothers’ fetal and neonatal complications are scarce. This study investigated the relationship between neonatal and fetal complications in mothers with severe pregnancy complications and a near miss due to the importance of socioeconomic and other factors. Such communication may serve as a basis for prioritizing the implementation of measures and allocation of financial resources to improve the health of mothers and infants in Iran and other countries with similar conditions.
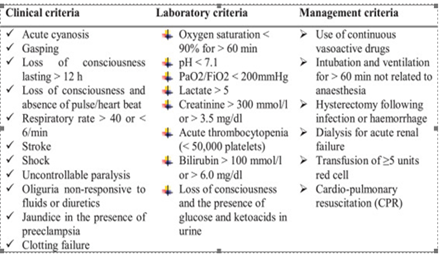
The present study was a retrospective and cross-sectional study. After receiving written approval from the hospital director, data were extracted from the files of patients admitted to Shahid Mostafa Khomeini Hospital and Khatam Al-Anbia Hospital between April 2017 and March 2017 for termination of pregnancy. Mostafa Khomeini Hospital is a general educational and semi-governmental hospital affiliated with Shahed University with over 2,000 births per year, while Khatam Al-Anbia Hospital is a private general hospital with over 3,000 births per year. Inclusion criteria included cases with severe maternal outcomes (Table 1), including severe postpartum hemorrhage and severe preeclampsia (persistent systolic blood pressure of 160 mm Hg or greater or diastolic blood pressure of 110 mm Hg or greater), proteinuria of at least 5 g per 24 hours; oliguria of over 400 ml per 24 hours, HELLP syndrome and pulmonary edema and eclampsia, severe systemic infection or sepsis (presence of fever [a body temperature higher than 38 °C]), confirmed or suspected infection (e.g., chorioamnionitis, miscarriage, endometritis, pneumonia),at least one heart attack greater than 90, a respiratory rate less than 20, leucopenia (white blood cell decrease less than 4000), leukocytosis (white blood cells more than 12000),and rupture of the uterus and the other life-threatening disorders are listed in Table 1 (15):
This evaluation also examined demographic characteristics such as maternal age, number of pregnancies, gestational age, stillbirth, abortion, and ectopic pregnancy, underlying maternal diseases such as diabetes and anemia, type of previous deliveries, prenatal care, premature rupture of the bladder, and induction of labor. The condition of these mothers’ fetuses and infants was evaluated. Apgar score, birth weight, gestational age based on last menstrual periods and obstetric ultrasonography, admission to neonatal intensive care unit, jaundice, neonatal seizures, sepsis, respiratory failure syndrome, stillbirth, and neonatal mortality were recorded from the infant and fetus records of mothers with severe pregnancy complications.
Data were recorded in SPSS (v. 22) software. Quantitative and qualitative data were analyzed using the chi-square test, Analysis of Variance (ANOVA), and the t-test, where a statistical significance level of p<0.05 was considered.
Ethical consideration
This research was part of a doctoral research project and was approved by the Research Ethics Committee of Shahed University (IR.SHAHED.REC.1398.059).
Between 2016 and 2018 (three years), Mostafa Khomeini Hospital (M.KH.H) performed 8302 deliveries, and Khatam Al-Anbia Hospital performed 9243 deliveries (KH.AN.H).
According to World Health Organization (WHO) criteria for severe complications and the near-death maternal approach, 138 mothers qualified to participate in the study. The participants’ ages ranged from 17 to 44 years (there was a 60-year-old woman who became pregnant through assisted reproductive technology [ART]), with a mean of 33.95±5.56years. The average age of mothers in the two hospitals did not differ significantly (p>0.05). Of the total population, 105(81.39%) have undergone a cesarean delivery, 55(39.9%) of the mothers were first-time mothers, and 2(1.4%) did
not receive prenatal care. Other case characteristics are shown in Table 2. In total, 44 (32.6%) mothers with severe maternal complications demonstrated near-death complications. Meanwhile, 64(46.4%) mothers in M.KH.H. suffered from severe maternal complications, of which 18(28.1%) were near-miss. In addition, 74 mothers (53.6%) in KH.AN. H. exhibited severe maternal complications, of which 27(36.5%) were near misses, and one woman died. It was determined that the prevalence of severe maternal complications in M.KH.H was 7.7 per 1000 live births and that in KH.AN.H, it was 8 per 1000 births. In this study, heavy bleeding (36.2%) and preeclampsia (50.7%) were the most common causes of severe complications in mothers (Figure 1).
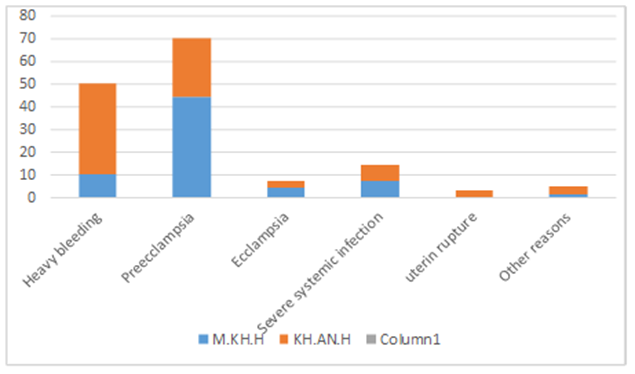
Figure1: Frequency of maternal complications
In addition, there were 4(2.9%) abortions and 5(3.6%) ectopic pregnancies. A total of 45 (32.6%) of the near miss mothers were transferred to the intensive care unit, 31 (22.5%) of them required critical interventions, and blood disorders were the most common organ dysfunction (Table 2).
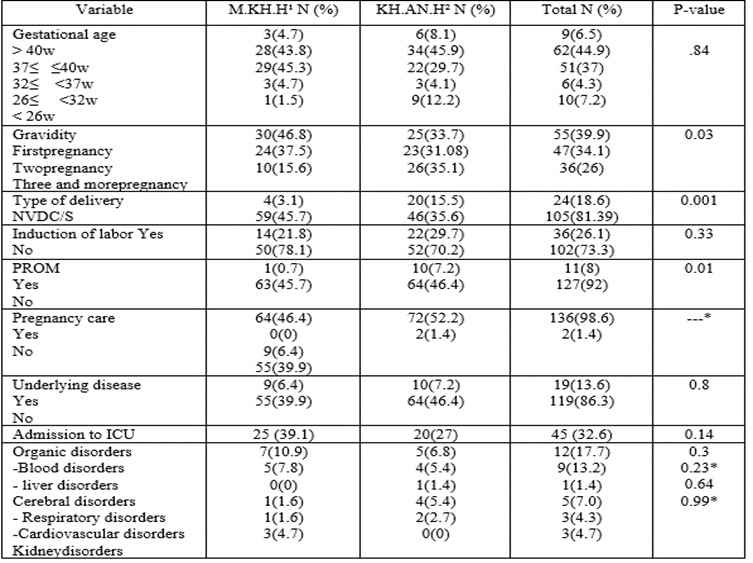
Table 2: Comparing the characteristics of the mothers studied in the two hospitals under study
The mean weight of neonates in the study group was 2719.27±711.57 grams, and the mean weight of neonates in the two hospitals did not differ significantly (p=0.198) (Figure 2).
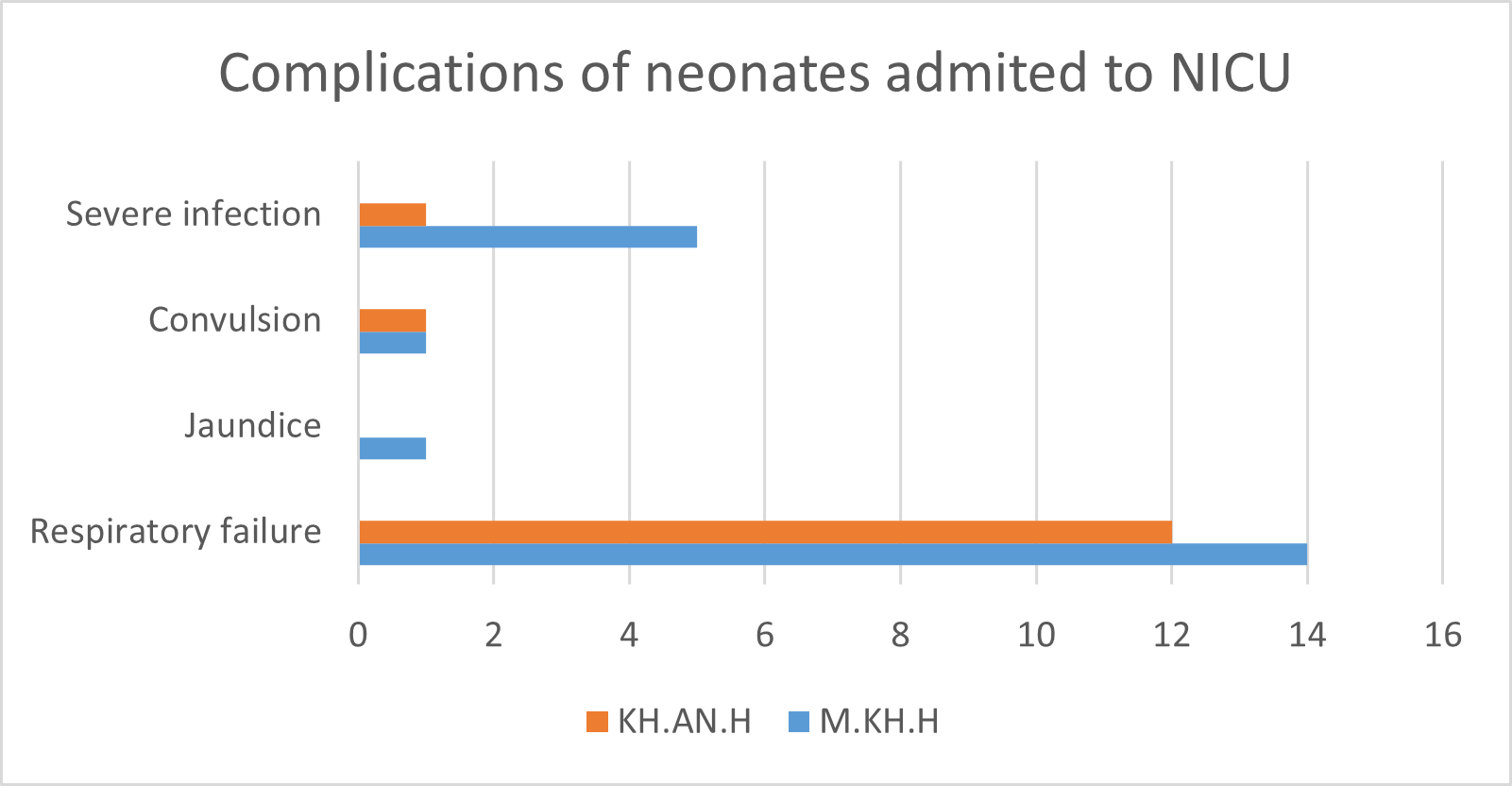
Figure 2: Complications frequency of neonates admitted to NICU in KH.AN.H and M.KH.H
Out of 131 births (departure of pregnancy after 20 weeks), 46 (35.11%) infants weighed less than 2500 g, of which 13 (30.95%) were born to mothers who were close to death (Table2). Furthermore, 57 (44.5%) infants were born prematurely (55.1% of neonates in M.KH.H and 41.2% of neonates in KH.A.H) with a birth age of 37 weeks or less. There were 13 (32.5%) cases of preterm births among women belonged near-miss mothers. Overall, 50% of neonates of near-miss mothers were preterm.
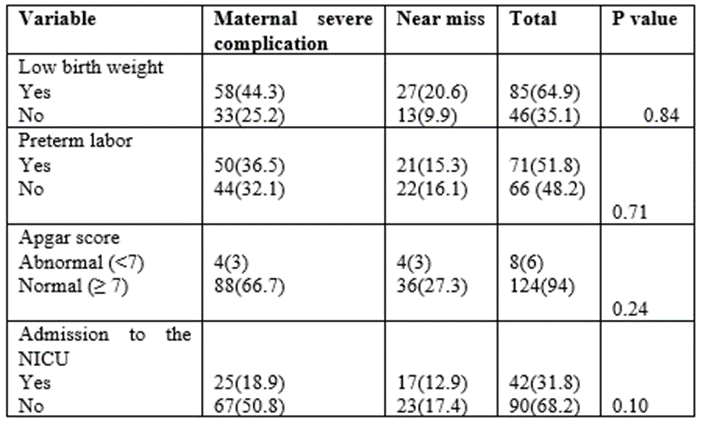
Table 3: Prevalence of neonatal complications in mothers with severe pregnancy complications
There was no statistically significant difference (p = 0.21; Table3) between the two hospitals (does not calculate the rate of abortion and ectopic pregnancy). Forty-two infants (31.8%) were admitted to the intensive care unit, with 17.4% and 14.4%at M.KH.H and KH.A.H, respectively. Of these infants, 17 (42.5%) were related to near miss mothers. Notably, there were 4 cases of neonatal death (3%) and 5 cases of intrauterine death (3.6%), resulting in a prenatal mortality rate of 58.2 per 1000 births. Eighty-eight (59.9%) of the fetuses and newborns of the mothers who were studied experienced at least one complication. Twenty-six (61.9%) infants had respiratory failure, and 6 (14.2%) had a severe infection. Figure2 depicts the other complications of these infants. The correlation between average maternal age and gravidity with fetal complications was compared with the correlation between maternal background factors and fetal complications using t-tests and linear regression. The average age of mothers whose fetus-newborn experienced complications was 33.5±0.98, and the average number of pregnancies was 2.06±1.11. Although it was demonstrated that the likelihood of prenatal complications is higher in multiparous women over 30, this correlation was not statistically significant.

Table 4: The relationship between some pregnancy characteristics and neonatal complications using Fisher's exact test and binomial logistic regression
As shown in Table 4, Fisher’s exact test and binomial logistic regression test were used to assess the relationship between mode of delivery, prenatal care, premature rupture of amniotic fluid, and labor induction with fetal complication; 34% of mothers with the underlying disease had fetal-neonatal complications, and the cesarean rate among these women was 48.3%. However, there was no correlation between the mother’s demographic characteristics and perinatal complications.
In the past several decades, the world has made progress in reducing maternal and child mortality [15]. A possible correlation between maternal morbidity/mortality and potential adverse effects on child health may serve as a basis for establishing action execution priorities and allocating financial resources to support these actions [16] This study investigated the causes and perinatal outcomes of severe maternal complications and near-miss cases. This study estimated the prevalence of severe maternal complications to be approximately 8 per 1000 live births. In a few studies conducted in Iran, this index ranges from 25.2 cases per thousand live births in Kerman to 4.97 cases per thousand births in Alborz [5,17]. This difference may be attributable to the study population, the quality of hospitals (private versus public) and training, and the quality of midwifery care. This study was conducted in a semi-private teaching hospital (M.KH .H) and a private hospital (KH.AN.H).Almost all patients are immediately seen by a midwife and gynecologist, and if they are in distress, decisions are made more quickly. It should be noted, however, that because the cost of hospitalization in these centers is higher than that of government education centers, some complicated pregnancies are not referred to this hospital; therefore, if more research is conducted in these hospitals, the index figure above will likely change. This study revealed that preeclampsia and severe bleeding are among the most common causes. This is comparable to the findings of other Iranian and international studies [14, 17-19]. About one-third of mothers were hospitalized in the intensive care unit (a relatively high rate), the most common complication of their organ disorders is blood and coagulation disorders, and one in five mothers in this study required critical interventions such as blood transfusion and returned to the operating room for laparotomy.
These results are comparable to those of other studies. Obviously, economic and cultural factors must always be considered [5, 17, 20]. Unfortunately, approximately 60% of the newborns in the study population had prenatal complications. In the studies by Nakimoli et al.in Uganda [6] and Firdawek et al. (10), conducted in developing countries, 63.3% and 72.9% of infants and fetuses, respectively, had complications. The incidence of infants with complications is significantly higher than the incidence of infants without complications. In general, the risk factors for adverse maternal and perinatal outcomes are remarkably similar. Efforts to ensure maternal health will therefore have a multiplier effect on reducing infant mortality and neonatal and fetal complications [2, 21, 22]. Prematurity and low birth weight were our greatest perinatal complications. According to statistics, the incidence of prematurity and low birth weight infants ranges between9.5%-12%. [22, 23].
Approximately half of the neonates in this study were premature, and more than a third of them weighed less than 2500 grams, which is nearly five times higher than the average and demonstrates the significance of these complications among infants of mothers with severe complications. Identical to these findings, other studies found that between 45 and 54% of infants were born prematurely before 37 weeks of age [3, 20, 21, 24]. This high rate and similarity between societies are typically attributable to maternal complications, particularly preeclampsia. To save the lives of the mother and fetus, termination of pregnancy were performed prior to 37 weeks, which increases the risk of preterm and premature birth. Two-thirds of infant deaths occur in infants with low birth weight, and approximately 36% of infant deaths occur in premature infants. In premature infants, respiratory and necrotizing enter colitis are more prevalent [3, 25]. Various comparable studies have reported neonatal mortality rates ranging from 25 to 162 per thousand live births [7, 26, 27].
In the present study, 3% of newborns died, resulting in a neonatal mortality rate of 30 per one thousand live births. Although the infant mortality rate in our study was not particularly high, the overall infant mortality rate is 8.9 per thousand live births [23], which has nearly tripled in this study. On the other hand, the infant’s death has numerous psychological effects on the parents; therefore, efforts are being made to reduce this mortality rate [7, 28]. In this study, 3.9% of intrauterine deaths were also accompanied by a major complication. In the study by Mohammadi et al. at a public hospital in Iran, the rate of stillbirths was 12%, which is higher than the current study [14] . The study which was done in Nigeria by Adeoye and his friends, the result showed that the odds of still birth was around 5 times higher in those who developed maternal near miss when compared to those who delivered without complication [2] and there were 20.3% of stillbirths among women with severe maternal complications in Ethiopia(11). The lower rates of stillbirth and infant mortality in this study were likely due to the semi-private and private nature of the hospitals analyzed in this study. In these hospitals, the decision to terminate the pregnancy and save the life of the mother and fetus was made more quickly due to the higher quality of infant care and the NICU staff’s training and experience. Delays in obstetric care increase the risk of neonatal near-miss morbidity events and death [16].
Of the born infants, 31.3% were transferred to the intensive care unit, which is consistent with other studies such as Mohammadi et al. (31%) [14], and Adeoye I et al. (29.4%) [2]. Although approximately 30% of infants were transferred to the care unit, only 6.1% of infants had a low Apgar score; thus, it appears that low birth weight and prematurity are important causes of being in the NICU.
Relationship between maternal demographic characteristics and perinatal complications
Low maternal education, lack of family support, marital status, maternal age, and lack of health service confidence are risk factors for adverse maternal and neonatal outcomes [10, 17, 22]. Historically, these factors have been responsible for the worst neonatal outcomes. However, the factors were insignificant in our analysis, most likely due to the population’s homogeneous socioeconomic status [16]. A significant factor is the absence of inadequacy of prenatal care. Researches have shown that adequate prenatal care is an effective intervention in improving pregnancy outcomes and provides opportunity for consulting and reducing complications associated with pregnancy and child birth. A lot of percentage of maternal and fetal mortality, preterm births, or low-weight births is due to inadequate and inappropriate prenatal care during pregnancy [29, 30]. Our research was conducted, however, in two private and semi-public hospitals. The patients referred to these two hospitals were individuals with moderate and high social status, and more than 98% of them had prenatal control).
The prenatal care situation in Iran has significantly improved and now exceeds the global average. One of the specific objectives of the National Maternal Health Program was to increase the coverage of pregnancy care providers (at least six times) by more than 93% by the end of 2015. The improvement in the trend of pregnancy care coverage over the past two decades is the result of efforts and interventions made in the country’s health system in recent years [14, 30-32]. Sixty percent of our mothers were multiparous and over 35. This demonstrates the significance of monitoring older pregnant women, who are more likely to develop gestational hypertension and preeclampsia [17]. In developing countries such as the United Kingdom
also understand a strong association between emergency caesarean section and near misses therefore they concluded the increased odds of closed to death may be associated with the outcome or survival of mother rather than being a risk factor due to the temporal sequence of the accidents. This is because such treatment modalities are employed after the occurrence of a complication and not vice-versa. In spite of, this increased risk associated with emergency caesarean section may be related to the dislike of women and their family members towards caesarian delivery [2]. However, the complications of cesarean section and its role in increasing maternal complications in a country like Iran, where the statistics of cesarean section, especially requested cesarean section, are very high, may be even more important.
The present study had some limitations. The most important limitation is that the study was carried out in two hospitals (private and semi-private) in Tehran, the capital of Iran. Therefore, it does not represent cases of sever maternal complications occurring in other childbirth facilities in Iran.
Neonatal complications, particularly prematurity and low birth weight, are more likely in the presence of severe maternal complications. Due to the high prevalence of preeclampsia, training mothers to control blood pressure and preparing the necessary hospital facilities to assess and care for at-risk patients should be a priority in health planning. Additionally, due to the high prevalence of severe postpartum hemorrhage, it appears necessary to provide the necessary facilities for the care of these mothers. Consequently, it appears necessary to equip hospitals (level 3) with intensive care units for mothers and infants and trained personnel who can provide adequate support for mothers and infants.
This research was supported by Shahed University. We appreciate the cooperation of the staff at the Archive Offices of the Mostafa Khomeini and Khatam Al-Anbia hospitals.
The authors have no conflicts of interest to declare.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
