
Research Article | DOI: https://doi.org/10.31579/2690-1919/245
1 Ophthalmology Department, Faculty of Medicine and Health Sciences, Sana’a University, Republic of Yemen.
2 Medical Microbiology and Clinical Immunology Department, Faculty of Medicine and Health Sciences, Sana’a University, Republic of Yemen.
*Corresponding Author: Hassan A. Al-Shamahy, Faculty of Medicine and Heath Sciences Sana'a University P.O. Box 775 Sana'a, Yemen.
Citation: A Alshamahi EY, Al-Shamahy HA, A Al-Moyed KA, Hizam Al-Arosi SA. (2022). National Comprehensive Trachoma Treatment Campaign: Community Monitoring of Mass Drug Administration (MDA) Coverage and Practices. J. Clinical Research and Reports. 11(2); DOI:10.31579/2690-1919/245
Copyright: © 2022 Hassan A. Al-Shamahy, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 24 March 2022 | Accepted: 15 April 2022 | Published: 25 April 2022
Keywords: coverage; mass drug administration (MDA); mass treatment; monitoring; national campaign; trachoma; Yemen
Background: Trachoma is a communicable infection of the eye by certain strains of the Chlamydia trachomatis. It is the principal cause of loss of sight globally. Mass drug administration (MDA) with azithromycin is a foundation stone of World Health Organization (WHO)’s global struggle to eradicate trachoma by 2020.
Aims: The main objectives of the campaign's third monitoring are to check improvement of interventions and improvement of quality across times and activities implemented in seven selected districts of Ibb and Al-Hodeida governorates, Yemen.
Methods: A community based cross-sectional coverage survey was performed. 68 divisions were selected per selected districts of the two governorates. A disconnect Results Entry Form for each district surveyed was finished, saved and uploaded directly into the online Coverage Survey Analysis Tool to check improvement of interventions and improvement of quality across times and activities implemented.
Results: The national campaign for MDA covers 966 villages in 6 districts of Ibb and Al-Hodeidah governorates by 1932 healthcare workers. A total number of beneficiaries who were monitored from 476 homes reached 3,077, of whom 2,755 (90%, coverage rate) took the dose. The availability rates of trachoma medicines were ranged from 82% to 91%. The improper arrangement of treatment sessions rate was 17%, the incorrect position of the dose pole was 6%, while the correct records of drugs scored the rate of 99%, and the proper storage of drugs rate was 70%. The community collaboration during the treatment campaign the acceptable rate was 92%, while 3% exhibited unacceptable behaviors towards the treatment campaign.
Conclusion: In this survey, the national campaign for MDA in the 966 villages reach the target threshold (i.e. 90%) for effective coverage; with proper rates for the availability of trachoma medicines, good people reactions towards taking treatment, and the community collaboration; while bad rates for the improper arrangement of treatment sessions, the incorrect position of the dose pole and the preparation dosages by MDA team. Hence, programmatic enhancement should be made for the future campaign to achieve the estimated thresholds.
Trachoma is an infectious eye infection produced by certain strains of the chlamydia trachomatis bacteria. Active infection frequently starts at some stage in infancy or childhood and can become chronic. The bacteria are distributed by direct connection with eye and nasal secretions from infected individuals, or by contact with fomites (that is, nonliving objects that carry infectious agents, for example towels or washcloths) or by eye-seeking flies (mainly Musca sorbens). It is the main contagious cause of blindness and is endemic in 53 countries. An estimated 325 million people live in areas where they could be exposed to trachoma, and more than 7 million suffer from trichiasis, the last painful stage of this eye disease [1-3]. In the past three years, researchers in Yemen have become more interested in studying and investigating eye diseases, which include the problem of trachoma, as Yemen is one of the regions endemics with trachoma 4-12. From September 2013 to March 2015 a fieldwork was undertaken cluster-sampled survey in each of 42 evaluation units (EUs) including 166 rural districts of nine Governorates (Al Jawf, Al Hodeihah, Adh Dhale’a, Hadramoot, Lahj, Ma’rib, Taiz, Hajjah, Ibb) by means of the Global Trachoma Mapping Project systems and methodologies. The TF prevalence in children aged 1–9 years was ≥10% in two EUs (7 districts) and 5–9.9% in six EUs (24 districts). In adults aged ≥15 years, trichiasis prevalence was ≥0.2% in five EUs (19 districts). The surveys revealed that more than 2.7 million people in 30 districts need public-health interventions to deal with transmission of the trachoma and its associated morbidity [10]. Also, in a study by Al-Shamahi et al. [9], the prevalence of active trachoma (TF) was 10.93%, which is slightly higher compared to the previous study conducted in Yemen [10].
Researchers have found that it is possible to eliminate blinding trachoma by apply an integrated package of interventions - the so-called "safe strategy" which means: surgery for trachomatous trichiasis, treatment with antibiotics to clear an ocular infection; facial hygiene to decrease the transmission of chlamydia trachomatis in the eyes; and improving the environment, especially improving access to water and sanitation [1-12]. It has been shown that antibiotic treatment for people with trachoma helps prevent the disease from spreading in the community. Presently, azithromycin (Zithromax) is the optional for mass drug administration (MDA). In trachoma endemic areas MDA should be performed annually for a period of three to five years. A coverage survey is necessary to follow movement towards the goals of the program and to find communities with poor coverage in order to allow for appropriate and timely action [2,3]. It is important that MDA is used for the whole population to prevent, control or eliminate neglected tropical diseases (NTDs) such as trachoma, as the drugs (azithromycin for trachoma) are given periodically - using a campaign approach - to all at-risk populations in the area, and the rate is high. Therapy coverage is very crucial for MDAs: the greater the spread of infection, the more imperative it is to achieve high coverage rate. The World Health Organization commends that 80% of the target population should be reached with MDA at last. Country programs normally report treatment coverage by take from the number of azithromycin doses lasting in stock after MDA from the MDA target group, or by gathering reports from drug distributors. Although both methods are better than doing nothing, it is important to routinely verify the accurateness of reported coverage numbers, as they are subject to management and error [2,13,14].
Estimates of drug coverage from population surveys may raise the comprehension of the factors influence MDA efficacy. The survey results should provide valuable information on the existing gaps for projects aimed at preventing and eradicating the disease. Future MDA rounds will be able to take into account the results of this survey and enable trachoma control programs to reach target populations that may have been missed during previous rounds of MDA [13-15]. The main objectives of campaign monitoring are to verify the improvement of interventions and improvement of quality across times and activities implemented in seven selected districts in Ibb and Al-Hodeida governorates, Yemen.
Survey area and period: This survey was conducted from 18 to 20 February 2021 by 1932 health care workers, in intentionally selected intervention areas suffering from trachoma in Al-Hodeida and Ibb governorates. These areas are endemic to trachoma and the first round of a trachoma survey was conducted in 2015. The intended beneficiaries of MDA are over 2 million people in the 7 districts of trachoma intervention.
Survey design: The study was community based cross sectional observational study.
Survey population: All residents/population living in the selected districts was surveyed population.
Eligible population: Everybody living in the survey area (district) based on drug-specific eligibility criteria.
Ethical approval and consent form: Ethical approval was obtained from the Medical Research and Ethics Committee at the Faculty of Medicine and Health Sciences at Sana'a University in Document No. 713 dated January 11, 2021. All data, including participant identification, were kept confidential and informed consent obtained from the people themselves.
Inclusion criteria: Everybody living in the survey area, where current Trachoma MDA was considered to be included in the study.
Exclusion criteria: Those households which were closed during the survey data collection period. In addition, non-resident individuals who came to visit relatives from other location were excluded.
Sample size: The sample size, n, was established by means of the single population proportion formula:
n= (Z α/2)2 x p x q x DEFF/ d2
Where: α is level of confidence; p is the proportion of the population who is expected to have swallowed the drug is 50%. The expected coverage sample size will increase as the reported coverage approaches 50%, which ensures that the sample size is sufficient to meet study objectives; q is (1-p); Z is standard normal distribution curve value for 95% CI which is 1.96 (where α = 0.05); d is tolerable margin of error, i.e. 5% (0.05); and DEFF is the design effect, a measure that reflects the degree to which respondents in the same subunit are likely to be similar in terms of the information provided in response to; we used the suggested default of 4. The sample size was estimated at 1,530; including 35% margin of non-response, the sample size was estimated at 2,615 individuals but for more accuracy we increased the sample size to 3,077 individuals.
Monitoring variables: This component covered total number of beneficiaries who were monitored from 476 houses (surveys) during field visits reached 3,077. Data collected including: the availability of medication and facial cleaning supplies with the MDA team, treatment sessions arrangement in monitor areas, the recipients, preparation, time required for treatment and acceptance of medications, the status of the beneficiaries of accepting used medicines. It also includes: the preparation of beneficiaries for drug dosing according to standard methods by healthcare teams, prior knowledge of the campaign by community members, community collaboration during the treatment campaign and the availability of additional supplies during the comprehensive treatment campaign for trachoma.
Data entry and Analysis: Data were collected by using Android tablets, where all the forms were pre-installed Survey CTO platform. The data were uploaded to our servers using 3G or Wi-Fi internet connections. Then, follows a process of data review, cleaning and verification at the central level. The early handling of data ensured instant quality checks and corrections. Microsoft Excel was used for analysis. Results are presented as frequencies and proportions in tables.
Table 1, shows the names of the directorates and governorates participating in the national campaign for mass treatment of trachoma: Mass drug administration (MDA) in Yemen 2021. The national campaign for mass treatment of trachoma covers 966 villages in 6 districts of Ibb governorates and Al-Hodeidah from 18 to 20 February 2021.
| Governorate | Districts | No of villages |
| Ibb | Al-Sobrah | 94 |
Al-Sayani | 163 | |
Al-Odain | 126 | |
Di- Sifal | 150 | |
subtotal | 533 | |
| Al- Hodeida | Al-Zohra | 189 |
Al-Qanawis | 125 | |
Al-Lohayah | 119 | |
Sub-Total | 433 | |
total | 966 |
Table 1: The number of villages and names of districts and governorates involved in the national campaign for the mass treatment of trachoma: Mass drug administration (MDA) in YEMEN 2021
The total number of beneficiaries who were monitored from 476 homes (surveys) during field visits reached 3,077, of whom 2,755 (90%) took the dose, and the rest 10% did not take medicines for various reasons, including for example (the example is not limited to); being outside the house when visiting or having a chronic disease etc. Table 2 shows the frequency of pre-camping training sessions for the 1932 healthcare workers participating in MDA for the treatment of trachoma in Ibb and Al-Hodeida. 1912 (99%) of healthcare workers attended a one-day training course, while 0.5% attended a two-day training course and 0.5% attended a 3-day training course. Table 3 shows the number of randomly selected house for the monitoring survey in the two governorates, as 186 random homes were selected in Al-Hodiada and 290 homes in Ibb governorate. Table 4 shows the availability of medication and facial cleaning supplies with the MDA team in the selected villages. Azithromycin tablets, azithromycin syrup, tetracycline ointment and facial cleansing kits were available in 90%, 91%, 91% and 82% respectively.
| Course time | number | percentage |
| One day training | 1912 | 99 |
| 2 days training | 10 | 0.5 |
| 3 days training | 10 | 0.5 |
| Total | 1932 | 100 |
Table 2: The frequency of pre-camping training courses for the health care workers (HCW) involved in the mass campaign of trachoma treatment in Ibb and Al-Hodiada.
| Governorates | number | percentage |
| Al-Hodiada | 186 | 39 |
| Ibb | 290 | 61 |
| Total | 476 | 100 |
Table 3: The number of selected houses for the monitoring survey in the 2 governorates
Table 5 shows status of treatment sessions arrangement in monitor areas. The improper arrangement of treatment sessions rate was 17%, the incorrect position of the dose pole was 6%, the return rate of drug application methods was not in 2%, the correct records of drugs scored the rate of 99%, and the proper storage of drugs rate was 70% only. Table 6 shows the recipients, preparation, time required for treatment and acceptance of medications among selected persons on the monitoring survey. In 65% of the cases selected, the task was completed in less than 10 minutes, and in 6% of the cases in 10 minutes, while 6% of the cases the tasks were completed in more than 10 minutes. Table 7 shows the status of the beneficiaries of accepting used medicines. 92% of the selected subjects had a good reaction to taking the medications, 7% had an acceptable reaction while 1% (27 people) had a bad reaction to the drugs used.
| Supplies | Available | Partially available | Unavailable | |||
| No | % | No | % | No | % | |
| Azithromycin Tablets | 428 | 90 | 38 | 8 | 10 | 2 |
| Azithromycin syrup | 433 | 91 | 43 | 9 | 0 | 0 |
| Tetracycline ointment | 433 | 91 | 43 | 9 | 0 | 0 |
| Face cleaning supplies | 390 | 82 | 15 | 3 | 71 | 15 |
| Total 476 | ||||||
Table 4: The availability of medications and face cleaning supplies with the MDA team in the selected villages
| Number | percentage | |
| Proper Arranging of treatment sessions | ||
| Yes | 395 | 83 |
| No | 81 | 17 |
| Proper Position of dose pole | ||
| Yes | 447 | 94 |
| No | 29 | 6 |
| Applying Medicine return methods | ||
| Yes | 466 | 98 |
| No | 10 | 2 |
| Proper records of medicines | ||
| Yes | 471 | 99 |
| No | 5 | 1 |
| Proper storage of medicines | ||
| Yes | 333 | 70 |
| No | 143 | 30 |
Table 5: Status of the arrangement of treatment sessions in the monitoring areas
| Time | Number | percentage |
| Less than 10 min | 1791 | 65 |
| 10 min | 799 | 29 |
| More than 10 min | 165 | 6 |
| Total | 2755 | 100 |
Table 6: Beneficiaries, preparation and time required for treatment and acceptance of medicines
| Number | percentage | |
| Good | 2535 | 92 |
| Acceptable | 193 | 7 |
| Bad | 27 | 1 |
| Total | 2755 | 100 |
Table 7: Beneficiaries status towards acceptance to used the medicines
| Characters | Number | percentage |
| Preparing Beneficiaries for drug doses by MDA teams | ||
| Acceptable | 1570 | 57 |
| Partially Acceptable | 744 | 27 |
| unacceptable | 441 | 16 |
| Advance knowledge of the campaign by the communities members | ||
| Acceptable | 831 | 27 |
| Partially Acceptable | 1077 | 35 |
| unacceptable | 1169 | 38 |
| Community co-operation during the treatment campaign | ||
| Acceptable | 2831 | 92 |
| Partially Acceptable | 154 | 5 |
| unacceptable | 92 | 3 |
Table 8: Preparing Beneficiaries for drug doses by MDA teams, advance knowledge of the campaign by the communities members and the community co-operation during the treatment campaign
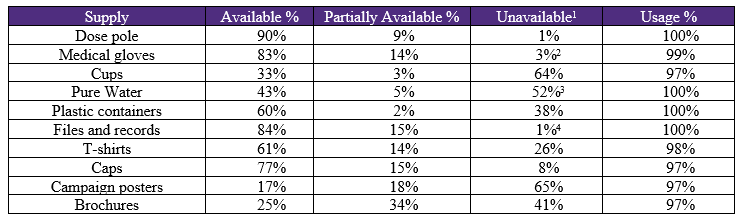
Table 8 shows the preparation of beneficiaries for drug dosing according to standard methods by healthcare teams. In 57% of the cases the preparation dosages were acceptable, 27% partially acceptable and 16% unacceptable (wrong doses). Also, Table 8 shows prior knowledge of the campaign by community members. The acceptable rate was only 27%, the partially acceptable rate was 35%, while in 38% the prior knowledge was unacceptable. In addition, Table 8 shows community collaboration during the treatment campaign. The acceptable rate was 92%, the partial acceptable rate at 5%, while 3% (92 respondents) exhibited unacceptable behaviors towards the treatment campaign. Table 9 shows the availability of additional supplies in selected areas during the comprehensive treatment campaign for trachoma. There was a significant shortage of campaign posters (65%), cups (64%), clean water (52%), brochures (41%) and plastic containers (38%).
This inspection was performed to assess the coverage and achievements of post-MDA trachoma in Ibb and Al-Hodeida governorates. In this survey, the total number of beneficiaries that were monitored from 476 homes (surveys) during field visits was 3,077, of whom 2,755 (90%) took the dose, and the rest 10% did not take medication, i.e. coverage rate of the treatment was 90% which is more than 80% the target threshold for effective coverage recommended by the World Health Organization [16]. The current coverage rate is better than that reported by Bekuma et al. in Ethiopia [17], the coverage rate is 80%. However, the figure cited here is much higher than in Kenya where 65.7% and 64.1% of the respondents had treated for 18. This coverage is also higher than a study in Northern Tanzania which was 76% in 2005 and 76.9% in 2011 19, also higher than study conducted in Nigeria in 2013 reported a coverage of 60.3 . When coverage is greater than 90%, there will be less chance of a recurrence of trachoma until the next round of annual mass drug administration begins; and management may gain higher acceptance over time. Additionally, this may also be due to the great effort made to mobilize and increase access to information as reflected from the qualitative study [21]. The discrepancy between studies may be due to the reason for the current study being conducted in the high rate of drug availability as in the case of azithromycin tablets, azithromycin syrup, tetracycline ointment, and facial cleansing tools available in 90%, 91% and 91% and 82%, respectively (Table 4). Also due to the high rate of pre-camping training sessions for 1932 healthcare workers participating in MDA which was 99% (Table 2). Also in Kenya and Ethiopia surveys, access is more difficult than Yemen due to the presence of damage to roads and bridges caused by the rainy season in these countries during MDA campaigns [16-18,22].
Concerning the status of the treatment sessions arrangement in the control areas in the current study. The improper arrangement of treatment sessions rate was 17%, the incorrect position of the dose pole was 6%, the return rate of drug application methods was not in 2%, the correct records of drugs scored the rate of 99%, and the proper storage of drugs rate was 70% only. These results are almost identical to those reported from Ethiopia and Kenya where improper arrangement of treatment session rate occurred more frequently17,18,22. This indicates that more training is needed for the team of healthcare workers participating in the MDA trachoma campaign.
The incorrect position of the dose pole (dose by height) in the current study was 6%, and as a result, there was a fear that some children might take more than they should. Some participants even stated that it is better to give medication to children based on their age rather than their height. This was also confirmed by the current results in monitoring the preparation of beneficiaries for drug doses according to standard methods by health care teams. In 57% of the cases, the dosages of the preparation were acceptable, 27% partially acceptable and 16% unacceptable (wrong doses) (Table 8). Concerning prior knowledge of the campaign by community members in the current study. The acceptable rate was only 27%, the partially acceptable rate was 35%, while at 38% the prior knowledge was not acceptable. Mass drug administration must be preceded by appropriate mobilization activities for its successful implementation. In this study, among those who received the Zithromax group therapy, 38% had unacceptable prior knowledge and this could lead to obstacles to the MDA campaign.
According to community cooperation during the treatment campaign. The tolerable rate was 92%, the acceptable partial rate 5%, while 3% (92 participants) exhibited unacceptable behaviors toward the treatment campaign (Table 8). This could improve their understanding of the benefits of the drug and contribution in azithromycin (Zithromax) mass drug administration campaign, consequential in improved treatment coverage. Throughout the campaign, health extension workers trained the community on personal hygiene, and to swallow the drug as it prevents from eye disease. Even though the information presented is not inclusive to tackle all the SAFE strategies for trachoma elimination, it could improve the community’s belief for the mass treatment. This is consistent with the health belief model, which says that knowledge, awareness and attitudes about the diseases positively affect the acceptability of the mass treatment [23].
Considering the recipients, preparation, time required for treatment and acceptance of medications among selected persons on the current monitoring survey. In 65% of the cases selected, the task was completed in less than 10 minutes, and in 6% of the cases in 10 minutes, while 6% of the cases the tasks were completed in more than 10 minutes. From a qualitative finding, one of the frequently reported issues was crossing the entire population on the same day. Because large populations may come to intervention sites imposing a disproportionate burden on service providers to administer and register and result in service users complaining about the potentially long waiting hours to get drug administration. Taking a lesson from these results complete the task in less than 10 minutes in a location convenient for most community members. The literature has indicated that detect obstacles that persist across diverse health behaviors for instance lack of time (due to family, household and professional responsibilities), admittance issues (transportation and facilities), established attitudes, limitations in the physical environment and lack of understanding can be useful in designing successful community-based interventions [24].
In this survey, the national campaign for MDA in the 966 villages reach the target threshold (i.e., 90%) for effective coverage; with proper rates for the availability of trachoma medicines, good people reactions towards taking treatment, and the community collaboration; while bad rates for the improper arrangement of treatment sessions, the incorrect position of the dose pole and the preparation dosages by MDA team. Therefore, programmatic improvements should be made for the future campaign to reach the expected thresholds of coverage and managements. Furthermore, health extension workers should be involved in delivering messages that focus on SAFE strategies for eliminating trachoma that can enhance community acceptance of mass treatment.
No conflict of interest associated with this work.
This research work is part of the round 1 monitoring of the national campaign for MDA that done under the supervision of the Ministry of Health and Population, Sana'a, Yemen, and WHO, Sana’a office. All authors were members of this work.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
