
case report | DOI: https://doi.org/10.31579/2641-0419/241
1Department of Internal Medicine, Michigan State University, Lansing, MI
2Department of Cardiology, Michigan State University, Lansing, MI
*Corresponding Author: Rohan Prasad, Department of Internal Medicine, Michigan State University, Lansing, MI
Citation: Surya Chennupati, Rohan Prasad, Tyler Kemnic, Abdullah Al-abcha, Manel Boumegouas., et all (2022). Myopericarditis as an Extra-Intestinal Manifestation of Crohn’s Disease: A Case Report. J. Clinical Cardiology and Cardiovascular Interventions, 5(1); DOI:10.31579/2641-0419/241
Copyright: © 2022 Rohan Prasad, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 30 November 2021 | Accepted: 31 December 2021 | Published: 07 January 2022
Keywords: myopericarditis; crohn’s disease; extra-intestinal
Introduction: Myopericarditis is an uncommon manifestation of Crohn’s disease. Interestingly enough, it can present in a patient without any acute bowel symptoms.
Case Presentation: A 21-year-old male with a medical history of Crohn’s disease and eosinophilic esophagitis presented to the hospital with chest pain and fever. Blood work revealed elevated troponin, C-reactive protein, and sedimentation rate levels. Electrocardiogram (EKG) showed diffuse ST elevation in all leads. Transthoracic echocardiogram (TTE) demonstrated a small pericardial effusion without valvular abnormalities. The patient was diagnosed with myopericarditis. Extensive etiological workup was negative, in the absence of other explanations, it was attributed to his Crohn’s disease. The patient was started on colchicine and ibuprofen. Out-patient follow-up revealed resolution of symptoms.
Conclusion: This case reports the rare occurrence of myopericarditis and Crohn’s disease. Inflammatory bowel disease as a cause of myopericarditis has been reported in some cases within the literature; however, there is no definitive mechanism known.
Abbreviations
EKG: electrocardiogram
IBD : inflammatory bowel disease
TTE : Transthoracic echocardiogram
Introduction
Myopericarditis is defined as inflammation of the pericardium with myocardial involvement.[1] Viral infections are considered the most common etiology of the disease.[2] While uncommon, myopericarditis has been associated as an extra-intestinal manifestation of Crohn’s disease.[3,4,5] Myopericarditis can present without acute bowel manifestations of Crohn’s disease.[6] This case report was prepared following the CARE guidelines [7].
Case Narrative
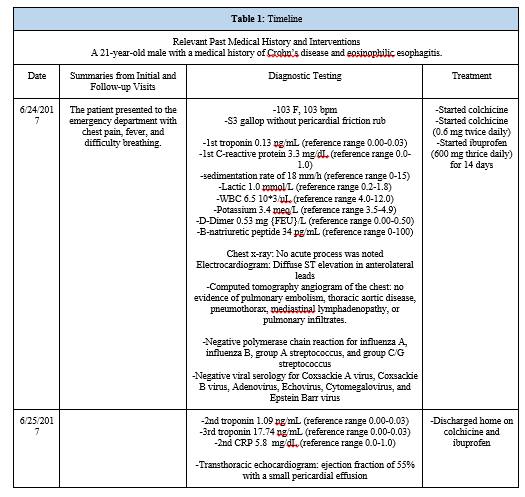
A 21-year-old male with a medical history of Crohn’s disease and eosinophilic esophagitis presented to the emergency department with chest pain, fever, and difficulty breathing. His Crohn’s disease has been controlled with vedolizumab and azathioprine for two years prior to presentation. He had no significant past surgical, social, or family history. His chest pain was sharp, located beneath the bilateral lower ribcage, worsened with deep breaths, and improved by leaning forward. His symptoms started one day prior to presentation. On presentation, his vital signs showed a temperature of 103 Fahrenheit, heart rate of 103 bpm, but otherwise normal. Cardiopulmonary auscultation revealed an S3 gallop without a pericardial friction rub.
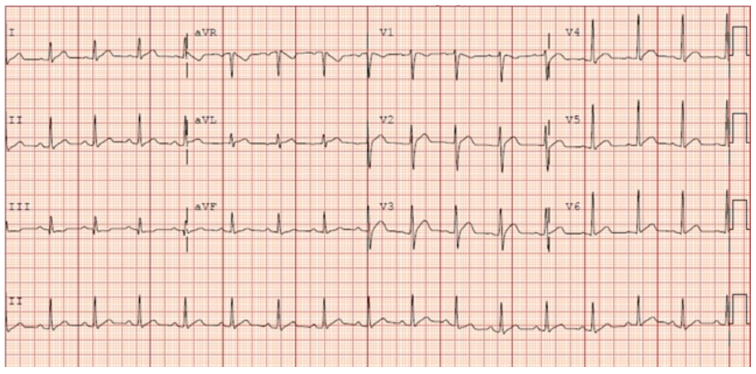
On admission, laboratory work-up revealed a troponin level of 0.13 ng/mL that trended to 17.74 ng/mL, C-reactive protein of 3.3 mg/dL that trended to 5.8mg/dL, and sedimentation rate of 11 that trended to 18 mm/h. The patient had a normal white blood cells count and brain natriuretic peptide. The polymerase chain reaction was negative when the nasopharyngeal specimen was tested for influenza A, influenza B, group A streptococcus, and group C/G streptococcus. Viral serology was negative for Coxsackie A virus, Coxsackie B virus, Adenovirus, Echovirus, Cytomegalovirus, and Epstein Barr virus. Electrocardiogram (EKG) showed diffuse ST elevation in the anterolateral leads (Figure 1).
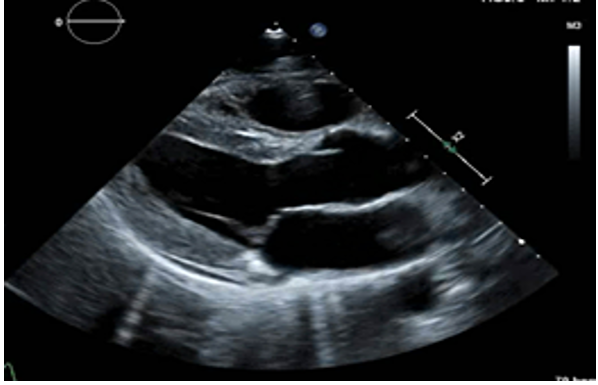
Computed tomography angiogram of the chest showed no evidence of pulmonary embolism, thoracic aortic disease, pneumothorax, mediastinal lymphadenopathy, or pulmonary infiltrates. Transthoracic echocardiogram (TTE) showed an ejection fraction of 55% with a small pericardial effusion (Figure 2).
The patient was diagnosed with myopericarditis. After consulting with the patient’s gastroenterologist, it was decided that the benefits of a fourteen-day non-steroidal anti-inflammatory with Crohn’s disease outweighed the risks. The patient was then discharged on colchicine (0.6 mg twice daily) alongside ibuprofen (600 mg thrice daily) and was instructed to return if his symptoms worsened or did not resolve. Repeat TTE and pericardial/endomyocardial biopsy were discussed with the patient, but due to the resolution of symptoms with medical management, the patient declined further investigations. During follow-up appointments with his primary care physician, the patient did not report a recurrence of these symptoms (Table 1).
The term myopericarditis indicates a primary pericarditic syndrome with myocardial involvement.[2] It is precipitated by multiple etiologies including infections, malignancy, and autoimmune diseases. Viral infections are the most common etiology.[2] The differential diagnosis of myopericarditis is broad. Viral etiologies were excluded by negative viral serologies. Bacterial pericarditis is very rare in developed nations. Neoplastic etiologies were unlikely due to the patient’s age, clinical presentation, lack of risk factors, and lack of other signs or symptoms associated with malignancies. Autoimmune etiology was high on the differential due to the patient’s age and his history of Crohn’s disease. The presence of two or more out of the following features are needed for the diagnosis of acute pericarditis: chest pain, pericardial friction rub, EKG changes of diffuse ST elevation or PR depression, and pericardial effusion.[8] The clinical diagnosis of myopericarditis requires establishing the diagnosis of pericarditis at first, in addition to elevation of cardiac markers and the absence of new-onset focal or global left ventricular wall motion abnormalities.[8]
Extra-intestinal manifestations of inflammatory bowel disease (IBD) are common and can present before or after the diagnosis of IBD.[9] Joints, eyes, and skin are the most commonly involved organs.[9] Cardiac involvement is rare in IBD, but can include pericarditis, myopericarditis, arrhythmias, and conduction disorders.[10] Pericarditis is the common cardiac complication of IBD.[11] The relative risk of myopericarditis in Crohn’s is 8.3%.[12] Myopericarditis has been linked to IBD and specifically Crohn’s disease in multiple case reports (Table 2). There are two proposed mechanisms to explain the relationship between myopericarditis and Crohn’s disease. The first is an autoimmune-mediated inflammatory response against autoantigens and the second mechanism is related to the toxicity of 5-aminosalicylic acid and its derivatives.[13,14]
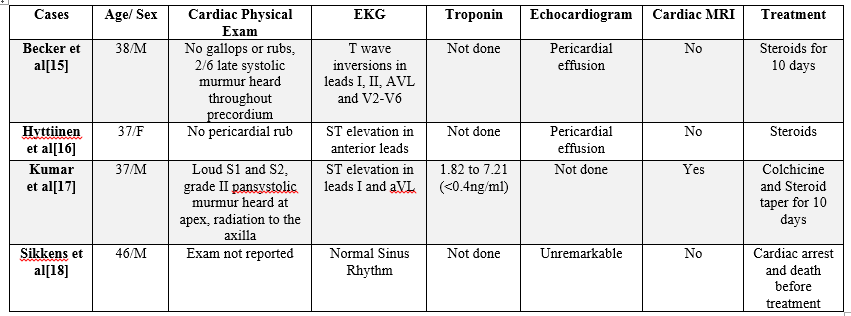
similarly to acute pericarditis. For viral or idiopathic pericarditis, non-steroidal anti-inflammatory drugs are the treatment of choice, specifically ibuprofen at 1200-1800 mg daily for days to weeks. Colchicine has been shown to be helpful for acute and recurrent pericarditis as it can decrease the recurrence rate by 50%. Corticosteroids, initially used in the past, are now avoided due to the increased risk of future recurrences. Additionally, intravenous immunoglobulins are not used because of insufficient data to support their use.[2] A case report from 1981 illustrates how corticosteroids were the backbone of the treatment for myopericarditis.[15] A recurrent myopericarditis in 2003, however, was not able to be controlled despite treatment consisting of prednisone, azathioprine, and sulphasalazine.[16] Finally, a 2019 case of acute myopericarditis presented during a Crohn’s flare-up, the treatment used was colchicine with an increase of the patient’s home steroid dose, which resulted in symptomatic relief.[17] Based on current recommendations, we treated our patient with ibuprofen and colchicine.
Conclusion
This case reports the rare occurrence of myopericarditis and Crohn’s disease. Patients with IBD have been reported to present with myopericarditis; however, the definitive mechanism is unknown. Our patient was diagnosed with myopericarditis after a thorough investigation and diagnostic work-up. After discussing risks versus benefits, the patient was started on colchicine and ibuprofen, which saw a resolution in symptoms in two weeks. In conclusion, a wide differential should be made for patients who present with myopericarditis.
Conflict of Interest
The authors have no conflicts of interest to disclose.
Funding
No funding was sought in writing this case report.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
