
Case Report | DOI: https://doi.org/10.31579/2690-1919/283
First Affiliated Hospital of Gannan Medical University Urology Department Ganzhou, China
*Corresponding Author: Henry K. YISA. First Affiliated Hospital of Gannan Medical University Urology Department Ganzhou, China.
Citation: Henry K. YISA, Yun F. LIAO, Guo X. ZHANG, Liu L. WEI. (2023). Multiple Calculi and Clear Cell Carcinoma in Same Kidney Rare Condition with Remarkable Implications for Surgery, Journal of Clinical Research and Reports, 13(1) DOI:10.31579/2690-1919/283.
Copyright: © 2023 Henry K. YISA. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 09 November 2022 | Accepted: 18 December 2022 | Published: 10 January 2023
Keywords: right kidney; laparoscopic; Right renal; lower pole; renal tumour
The main risk factors are tobacco smoking, obesity, hypertension, horseshoe kidneys, acquired renal cysts and genetic factors especially von Hippel Lindau disease (VHL).
Clear cell renal cell carcinoma (ccRCC ) is the most primary renal malignancy in adults with an incidence of 0.04% in the general population [1]. The main risk factors are tobacco smoking,obesity,hypertension, horseshoe kidneys,acquired renal cysts and genetic factors especiallyvon Hippel Lindau disease (VHL) [2] s. The aetiology of ccRCC is linked to a loss of the short arm of chromosome 3 and the tumor arises from the proximal tubules. Microscopically, it has a clear cytoplasm and a low nuclear/cytoplasmic ratio, the cytoplasm is filled with glycogens and lipids which dissolves during tissue processing resulting in a clear cytoplasm.
With respect to the concomitant existence of a clear cell carcinoma and calculus in the same kidney, only 7 previous eases have been reported in the world literature [3]. In all Cases, the tumor was identified at the time of open renal exploration to remove the calculus. In each patient, a total nephrectomy was performed instead of the calculus-removing, nephron-sparing procedure [4]. No underlying etiology to account for the coexistence of the calculus and ccRCC has been identified [5]. The patient reported on herein is unique in that the renal cell carcinoma was diagnosed prior to treatment. Instead of undergoing a percutaneous nephrolithotomy in which the nephrostomy tract could have gone through the tumor, a robot assisted laparoscopic partial nephrectomy was performed first, followed three months later by a two-stage flexibleureteroscope lithotripsy (FURL).
Level of evidence: 4
A 59-year-old man with a BMI of 28.8kg/m2 who was admitted in the hospital for 2 weeks due to intermittent right flank pains for 3 months, a known hypertensive, treated for pulmonary tuberculosis 5 years ago, a chronic smoker, 2-3 packs / day (60-90 pack years), no family history of renal disease, noprevious history of abdominal or pelvic surgery. Non contrast CT KUB showed that the right kidney had multiple stones and hydronephrosis, the largest measuring 3cm in diameter CT contrast revealed a tumor in the lower pole of the right kidney measuring 2.5cm in length with a strong suspicion of a renal carcinoma. A robot assisted suprapubic single port laparoscopic partial nephrectomy was done first followed by a two staged flexible ureteroscope lithotripsy (FURL) three months later. During the robot assisted operation, the advantages of flexibility and precision of robot arm were fully exploited, the renal artery was not clamped and the tumor was completely excised under zero ischemia. The operation time was about 40 minutes. Blood loss during the operation was about 100 ml. The vital signs were stable after the operation. Histopathology results showed clear cell renal carcinoma with tumor negative margins. After a full recovery of this patient after three months a two staged FURL was done with a one- week free interval between the two sessions, a 100% stone free rate was achieved and further stone analysis revealed a Calcium oxalate stone.

Figure 1: XRAY- KUB showing multiple right renal calculi
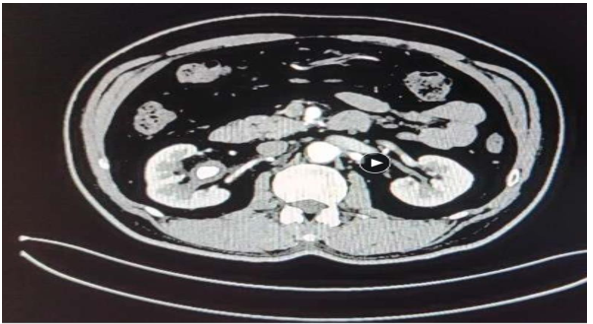
Figure 2: Abdominal CT Showing multiple right renal calculi
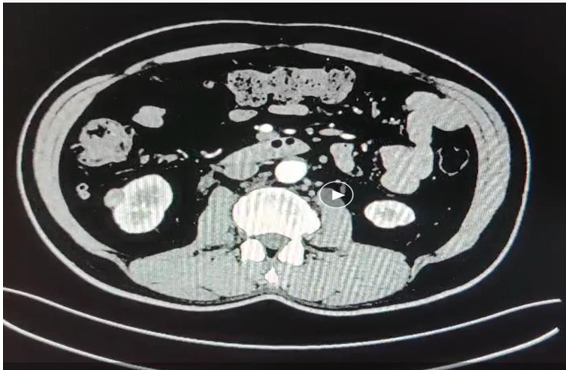
Figure 3: CT right kidney showing a renal tumor in the lower pole

Figure 4: Port position for robot assisted laparoscopic partial nephrectomy
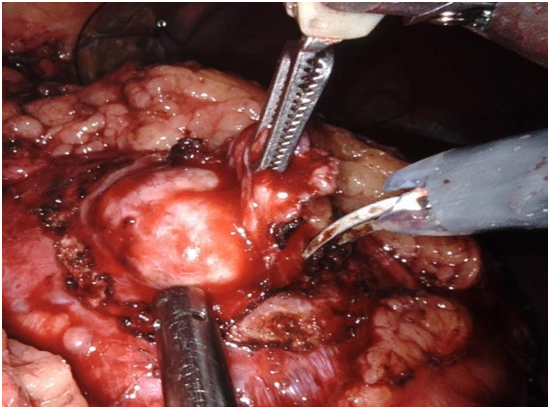
Figure 5: Intraoperative findings during robot assisted laparoscopic partial nephrectomy

Figure 6: Right renal lower pole after excision of renal tumor
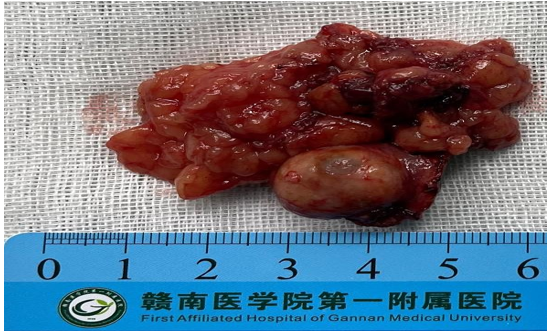
Figure 7: Excised renal tumor with a wide margine

Figure 8: Histopathology results of resected tumor revealing clear cell renal cell carcinoma
Patients beyond the fifth decade with a renal calculus have an increased likelihood of a coexisting malignancy and, as a result, should be carefully evaluated by critically evaluating the renal parenchyma before treatment of calculus especially PCNL to avoid dissemination of a renal malignant tumor and to prevent hematoma. If a tumor is suspected, further investigations should be carried out, a contrast computed tomography (CT), and/or magnetic resonance imaging (MRI) should be done. The concomitant presentation of a small renal mass with stone disease is uncommon, with an incidence of 3% but when it occurs it presents a treatment challenge especially in deciding which pathology that should be managed first. In this particular case the tumor was first excised through a robotic assisted laparoscopic partial nephrectomy without clamping of the renal artery followed by a staged flexible ureteroscope lithotripsy resulting in a favorable outcome.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
