
Review Article | DOI: https://doi.org/10.31579/2690-8808/122
Neonatal intensive care unit, Mohammed VI University Hospital, Marrakech.
*Corresponding Author: F.Bennaoui, QSB Tirana (University Hospital Center
Citation: K.Saadi , F.Bennaoui, N.Slitine and FMR maoulainaine. (2022) Multiple brain abscesses in a newborn with Down syndrome: heart disease or meningeal infection? Journal of Clinical Case Reports and Studies 3(8); DOI: 10.31579/2690-8808/122
Copyright: © 2022 F.Bennaoui, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 21 April 2022 | Accepted: 30 April 2022 | Published: 13 September 2022
Keywords: brain abscess; cyanogenic heart disease; trisomy; meningitis
Introduction: Cerebral abscess is a rare pathology in the newborn, most often secondary to meningeal involvement, but congenital heart disease is to be feared.
Objectives: To review a case of multiple cerebral abscesses in the newborn with a doubtful diagnosis through a clinical case.
Observation: Newborn at D6 of life, from a fullterm pregnancy, with a negative infectious anamnesis, admitted for fever at 38. The first one appeared at D4 of life, in whom the clinical examination found an icteric newborn, with a trisomic face, tachycardia at 180bpm, axial hypotonia, FANT and RS+, systolic cardiac murmur and light sub-costal draught. In front of this picture, a lumbar puncture was carried out objectifying a lymphocytic meningitis, At J8 of life, the newborn presented a convulsion, An ETF was carried out objectifying a hypoechogenic image with hyperchogenic border in cocarde evoking an abces confirmed by CT. The echocardium performed as part of the etiological workup, objective a single ventricle, CIA ostium primum large, IVC admission, single atrio ventricular valve, complete atrio ventricular canal, persistence of the ductus arteriosus and Coarctation of the aorta. The newborn was put on parenteral antibiotic therapy based on C3G meningeal dose + vancomycin + metronidazole by intravenous route then oral relay, with a scannographic control and neurological clinical evaluation. In front of this case, the question that arises: are his abscesses secondary to meningitis or to congenital heart disease?
Conclusion: Brain abscess is a rare pathology, with heavy after-effects, and the prognosis of patients has improved thanks to the progress of imaging techniques, the use of ATB treatments, and minimally invasive neurosurgery. It is to be feared in front of congenital cardiopathies with right-left shunt.
Brain abscess is a rare pathology in newborns, most often secondary to meningeal involvement, but congenital heart disease is to be feared.
Objectives
To review a case of multiple cerebral abscesses in the newborn with a doubtful diagnosis through a clinical case.
Observation
Newborn at 6 days of age, from a pregnancy at term 39SA according to DDR and 37.1SA FARR, with a negative infectious anamnesis, delivery by VB without notion of perinatal asphyxia. Admitted for fever at 38.1°
appeared at D4 of life associated with a non cholestatic icterus, in whom the clinical examination finds an icteric newborn, with a trisomic face, tachycardia at 180bpm, axial hypotonia, FANT and RS+, systolic cardiac murmur and light sub costal draught.
In front of this picture, a lumbar puncture was performed, showing a xanthochromic aspect, leukocytes =800, red blood cells =320, lymphocyte predominance = 70%, absence of germs, sterile culture (performed after two doses of ceftriaxone), meningeal PCR was negative.
An infectious workup was requested, showing a CRP=31.9 and WBC=11510 PNN=9110, with a sterile blood culture. The chest X-ray (Figure 1) showed cardiomegaly with a TIA of 0.6 associated with right alveolar-para cardiac foci.

Figure 1: Chest X-ray with ICT=0.6
At this stage, the diagnosis retained was an IPN with meningeal and pulmonary localization in a trisomic newborn, the patient was put on bi ATB = C3G100mg/kg/d + gentamycin 5mg/kg/d.
At 8 days of age, the newborn presented a nystagmus-like convulsion that rapidly resolved without any sign of localization or anisocoria. An ionogram was requested and came back without any abnormalities. A FET was performed showing a hypoechogenic image with a hyperchogenic cocardial border suggestive of an abscess (Figure 2).
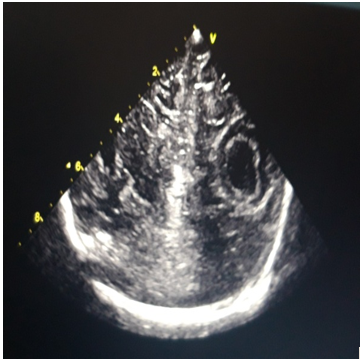
Figure 2: hypoechogenic image with a hyperchogenic border suggesting an abscess
The brain CT showed 2 left frontal formations measuring 15.6*12.2 mm, and left fronto-parietal 33.5*24.3 mm, surrounded by peri-lesional edema, exerting a mass effect on the homolateral lateral ventricle without subfalcoral involvement, the aspect was in favor of brain abscesses + meningitis (figure 3).
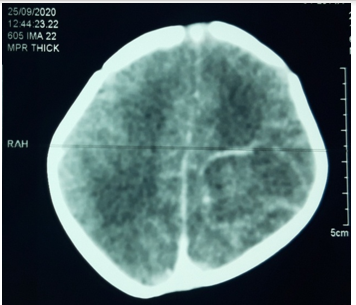
Figure 3: first CT scan: 2 brain abscesses
As part of the etiological work-up, an echocardiogram was performed, showing a single ventricle, a large ostium primum AIC, an admission IVC, a single atrio ventricular valve, a complete atrio ventricular canal, persistence of the ductus arteriosus, and coarctation of the aorta (Figure 4).
The newborn was put on parenteral antibiotic therapy based on C3G meningeal dose + vancomycin + metronidazole for 4 weeks then oral relai of ciprofloxacin and mitronidazole under scannographic control each month, there was no indication for surgery in view of the cardiopathy terrain, and the multiplicity of abscesses.
In this case, the question that arises is whether his abscesses are secondary to meningitis or to congenital heart disease.
Brain abscess is a rare condition in neonates and infants under 6 months of age [3]. Large case series of brain abscesses in the neonatal population have not been reported in the literature. [3]
For infants and newborns, the cause is mainly neonatal meningitis or sepsis [4]. even though brain abscess is an unusual complication of bacterial meningitis (1.3-4%) +++ [5].
It should be noted that meningeal involvement is not essentially present in cerebral abscesses (hematogenous involvement). Colonization of the cerebral parenchyma during sepsis can be explained by the DG shunt [5].
The first case of brain abscess associated with congenital heart disease was reported in 1814 by Farre. And since then, it has been reported in the literature as a rare disease ...|1] The incidence of brain abscesses in the population with congenital heart disease varies between 5 to 18.7%, with an increased mortality rate for cyanogenic heart disease [2].
Several theories have been proposed: because of the DG shunt, venous blood passes through the arterial system without being filtered into the pulmonary circulation, or because of a cerebral predisposition to localized infections in hypo-perfused areas due to emboli or polycythemia [1].
The usual presentation of brain abscesses during the neonatal period: irritability, bulging fontanel, rapid increase in PC with separation of the sutures, refusal to suckle, vomiting [5], and because of hemodynamic instability, and coagulation disorders, these brain abscesses may rupture into the ventricles [2].
The most frequent germs are the BGN especially citrobacter diversus, proteus, pseudomonas due to their necrotizing effect, unlike klebsiella pneumoniae [5] with localizations of which predominate in the frontal, temporal, and parietal lobes [2], and an abscess capsulation that can be seen from 10-13th days [4].
Management depends on the anatomical location, number, size and nature of the abscess, age and neurological status of the patient [5]. It combines medical and surgical treatment. The duration of antibiotic therapy is 6 to 8 weeks, to be prolonged in immunocompromised patients [5]. Surgical intervention reduces the abscess mass, improves the efficacy of TBA treatment, and allows intrathecal/intraventricular or intracavity administration of TBAs.
For patients with brain abscesses secondary to hematogenous dissemination, treatment consists of a tri-TAB: C3G+Mitronidazole to cover anaerobes, vancomycin will be added to treat a possible staph infection, pending the results of identification [6]. In front of abscesses secondary to congenital heart disease, streptococcus and hemophilus are targeted [6].
Glucocorticoids can reduce the passage of germs to the CNS, but their use should be limited to patients with significant cerebral edema +++, The use of hyperbaric oxygen has been cited in some case series [6].
Surgical intervention decreases the mass of the abscess, improves the effectiveness of TBA treatment, allows intrathecal/intraventricular or intracavity administration of TBAs, An abscess > 2.5cm requires surgical drainage, No surgical indication in front of small multiple abscesses [5], it should also be noted that the association of medical treatment with surgical treatment has decreased the mortality rate by 40 to 60% [2].
The criteria for evaluating treatment are based on the neurological state and the diameter of the abscess on imaging, and brain imaging is then repeated in the event of neurological deterioration, after 1 to 2 weeks if there is no clinical improvement, and every 2 weeks to 3 months until clinical healing is evident. Surgery is then indicated in the event of clinical deterioration with an increase in the size of the abscess on imaging, despite the use of TBAs [6].
The outcome of patients with brain abscesses has improved over the last 50 years, following the improvement of brain imaging techniques, the use of antibiotic treatment regimens, and the introduction of minimally invasive neurosurgical procedures. Mortality has decreased from 40% in 1960 to 15% in the last decade. Currently, 70% of patients with brain abscesses have a good outcome, with no or minimal neurological sequelae, despite this, functional and neuropsychological evaluation after brain abscesses remain poorly contributing [6].
Brain abscess is a rare pathology, with heavy after-effects. The prognosis of patients has improved thanks to the progress of imaging techniques, the use of ATB treatments, and minimally invasive neurosurgery. It is to be feared in front of congenital cardiopathies with D-G shunt.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
