
Research Article | DOI: https://doi.org/10.31579/2690-8808/167
1 Consultant and Head, Dept. of Microbiology and Infection Control, Dharamshila Narayana Super- speciality hospital
2 Senior Resident, Dept. of Microbiology, Dharamshila Narayana Super-speciality hospital
3 Senior Technologist, Dept. of Microbiology, Dharamshila Narayana Super-speciality hospital
4 Infection Control Nurse, Dept. of Microbiology, Dharamshila Narayana Super-speciality hospital
5 Technicians, Dept. of Microbiology, Dharamshila Narayana Super-speciality hospital
*Corresponding Author: Gitali Bhagawati, Consultant and Head, Dept. of Microbiology and Infection Control, Dharamshila Narayana Super- speciality hospital.
Citation: Gitali Bhagawati, Sania Paul, Rekha Saji Kumar, Anita Bhatia, Mansi, Khusboo. (2023), Multidrug Resistant Fungal Isolates from Blood and Urine Samples in Covid-19 Infected Admitted Patients During the Second Wave of Pandemic in India. J, Clinical Case Reports and Studies, 4(4); DOI:10.31579/2690-8808/167
Copyright: © 2023 Gitali Bhagawati, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 02 February 2023 | Accepted: 10 February 2023 | Published: 20 March 2023
Keywords: coronavirus disease; Covid-19; urinary tract infections
Background: The coronavirus disease 2019 (COVID-19) pandemic engulfed the whole world with far-reaching consequences on overall health across the globe. In India, second wave of Covid-19 was more devastating; bacterial and fungal co-infections were mostly undiagnosed or under reported due to the constant focus on the virus. Our study was to identify the cases of multidrug resistant fungus in blood and urine in Covid-19 infected patients.
Material and Methods: The retrospective study was carried out during the second wave of Covid-19 pandemic in India in the department of microbiology in a 200 bedded tertiary care hospital in Delhi, over a period of two months- April, and May 2021. Truenat Real Time PCR (Molbio diagnostics Pvt., Ltd., Goa, India) was used for confirming the cases of Covid-19 from nasopharyngeal samples. All blood samples for culture were processed in automated blood culture machine (BACTEC FX40, Becton Dickinson, Heidelberg, Germany). For fungal culture, paired tubes of Sabouraud’s Dextrose Agar (SDA) were used. Vitek 2 Compact System 8.01 (bioMérieux, Inc. Durham, North Carolina/USA) was used for the final identification of yeast and yeast like fungus (YYLF) and their antifungal susceptibility pattern (AFSP). Control strains included Candida albicans ATCC (American Type Culture Collection) 14053, Candida parapsilosis ATCC 22019 etc.
Results: During the 2nd wave of pandemic in India, out of total patients undergone testing by Truenat RT-PCR, Confirmed Covid-19 infection (CCI) was found to be 53.09%. Out of this, patients admitted with Severe Covid-19 infection (SCI) was 22.96%. Blood culture positivity rate among admitted cases were 6.72% (54/803); out of this fungemia was seen in 16.67% (9/54). The prevalence of UTI among Covid-19 infected patients was found to be 18.09% (150/829); YYLF relate UTI was seen in 32% (48/150) patients. Fungal urosepsis (FUS) was found in seven cases of Covid-19 infections; causative agents included C. auris 71.43% (5/7), C. albicans 14.28% (1/7) and T. asahii 14.28% (1/7). All the patients with FUS with SCI had history of prolonged intensive care unit (ICU) stay (>10days) with comorbid condition like diabetes mellitus (DM) (57.14%) and hypertension (HTN) (57.14%). All of them (100%) were catheterized and were on central lines. Out of the 7 patients, 5 (71.43%) were on mechanical ventilator. C. auris isolates were 100% resistant to fluconazole (Minimum inhibitory concentration, MIC >32 mg/L) and voriconazole (MIC >1 mg/L); however, 100% sensitive to caspofungin (MIC 0.25) and micafungin (MIC <0.06).
Conclusion: Elderly patients with high risk factors and associated comorbidity were mostly succumbed to MDR YYLF infections along with Covid-19 infection; many leading to urosepsis with high mortality rate. Covid-19 virus itself and its management were favourable conditions for IFI. Therefore, looking at the drug resistance, prompt diagnosis and treatment are imperative with respect to secondary infections.
The coronavirus disease 2019 (COVID-19) or severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic engulfed the nations of the world with far-reaching consequences on overall health across the globe. In India, 29.27 million cases had been reported during the pandemic, with a case fatality rate of 1.24% (363,079 deaths) up to June 11, 2021[1, 2]. India was in the grips of devastating second wave of the virus with repeat lock downs in the country. By mid-April, the country was averaging more than 100,000 cases a day. During the second wave, India's healthcare system has been overburdened, causing a dearth of medical oxygen, hospital beds, and other essentialities for the COVID-19 patients [3].
Although COVID-19 was associated with predominantly respiratory symptoms, many literatures suggest multi-organ involvement such as cardiovascular, lower urinary tract etc. [4, 5]. Historically, super-infections have always been associated with poor outcome during viral illnesses [6, 7]. There are various publications suggestive of both bacterial and fungal co-infections and superinfections in Covid-19 infected patients leading to higher mortality rate [8, 9, 10, 11, 12, 13].
Fungal co-infections in COVID-19 patients emerged with higher incidence of acute infections despite anti-fungal treatment. The emergence of multidrug-resistant (MDR) Candida made the situation worse with treatment failure, adverse clinical outcomes, and even disease outbreaks over the pandemic [15,16]. Candida auris became the global health threat during Covid-19 pandemic because of its notorious ability for colonization in skin and in the environment leading to severe disease with high mortality rates [17].
The objective of our study is to evaluate superadded blood stream infection (BSI) and urinary tract infections (UTI) amongst the admitted patients of Covid-19 infection with special reference to MDR fungal infections.
Study Design
The retrospective study was carried out during the second wave of Covid-19 pandemic in India in the department of microbiology in a 200 bedded tertiary care hospital in Delhi, over a period of two months- April, and May 2021. The overall patients’ data were collected from Laboratory Information System (LIS), requisition forms, WHONET 5.6 software and files from the department of Medical Records Department (MRD). Data analysis included patient profile, medical history, laboratory parameters, microbiological findings, concomitant antimicrobial drug use, and treatments.
Inclusion criteria for the study:
Microbiological testing:
Patients admitted with acute respiratory illness (ARI) were included in the study. Nasopharyngeal samples were taken from admitted patients and confirmed for Covid-19 by Truenat real time PCR method.). Samples taken using nylon swab were inserted into the Viral Transport Medium (VTM) provided from the same company (Molbio diagnostics Pvt., Ltd., Goa, India). Samples were transported immediately and processed in in-house molecular laboratory as per manufacturer’s guideline. (Truenat Beta CoV Chip-based RT-PCR test for Beta Coronavirus, Molbio diagnostics Pvt., Ltd., Goa, India). The target sequence for this assay is E gene of Sarbecovirus and human RNaseP (serves as internal positive control). Confirmatory gene used was RdRP gene or ORF1a gene.
Definition:
Blood for cultures were processed by automated blood culture machine (BACTEC FX40, Becton Dickinson, Heidelberg, Germany). Once the machine flagged positive, we performed Gram stain from the positive blood culture bottle. Based on Gram staining, sub-culture was done in Blood agar (BA), MacConkey agar (MA) and/or Sabouraud’s Dextrose Agar (SDA). BA and MA plates were incubated at 370C for 24 hours for growth. Growth is analyzed for colony morphology and further processed for automated identification and antimicrobial susceptibility (AST) pattern. All plates with no growth were further re-incubated at 370 C for 24 hours. SDA tubes were incubated at both 370 C and 250 C for 24-72hours.
(i) Inclusion criteria:[20]
(a)Positive Paired blood culture
(b)Same species in paired samples,
(c)Single blood culture with significant pathogen.
(ii) Exclusion criteria:
All the urine samples were inoculated on Cystine Lactose Electrolyte Deficient (CLED) agar. For YYLF, based on significant colony count, Gram stain and cultural morphology, colonies were inoculated on two Sabouraud’s Dextrose Agar (SDA) slants, one was incubated at room temperature whereas, other was kept at 37°C for 24 - 72 hrs.
Inclusion criteria:
(a) Non-duplicate urine sample,
(b) Wet mount showing ≥ 10 White blood cells (WBC)/cubic mm,
(c) Significant growth with colony count ≥ 100,000 Colony Forming Unit (CFU)/ml [20]
(d) Colony count with < 100>
Exclusion criteria:
The growth on the slope was processed for identification of the fungus. To differentiate between Candida albicans and Non-albicans Candida (NAC), germ tube test was done.
Usually Yeast and yeast like fungus (YYLF) grows within 24-72hours; which were analyzed for colony morphology. Gram stain and/ Lactophenol cotton blue (LPCB) were carried out to see the structure and arrangement under microscope. Vitek 2 Compact System 8.01 (bioMérieux, Inc. Durham, North Carolina/USA) was used for the final identification and AFST. Control strains for YYLF included Candida albicans ATCC (American Type Culture Collection) 14053, Candida parapsilosis ATCC 22019 and Candida krusei ATCC 14243. MIC of Fluconazole, Voriconazole, 5-flucytosine, Amphotericin B, Micafungin, Caspofungin were standardized as per CLSI guidelines (2017) [22].
Covid-19 positivity rate during peak of 2nd wave in India (April and May 2021):
Total non-duplicate samples received for molecular confirmation of Covid-19 during the peak of 2nd wave of Covid-19 pandemic were 2679 and 1316 in April and May 2021 respectively. CCI in April and May were 62.71% (1680/ 2679) and 33.5% (441/1316) respectively; overall CCI being 53.09 %.
Patients with SCI were admitted during the 2nd wave of Covid-19 pandemic in India. Patients admitted with CCI with SCI were 350 (20.8%) and 137 (31%) in April and May 2021 respectively; overall admitted cases being 22.96%.
Results of blood cultures in patients with CCI:
Total number of non-duplicate blood samples received were 1147. Out of these samples, 344 were paired blood culture sets, from 344 patients; 459 were single blood cultures with significant growth with corresponding clinical history. The total number of patients undergone blood culture were 803.
Overall, blood culture positivity rate was 12.45% (100/803). Out of these, Coagulase negative Staphylococcus (CONS) comprised of 7% (56/803). On clinical correlation, CONS were found to be contaminants in 46 cases (5.73%). So, excluding contaminants, the positivity rate of blood culture was 6.72% (54/803).
Out of all pathogenic bacterial and fungal isolates in blood culture comprised of 83.33% (45/54) and 16.67% (9/54) respectively. The causative agent of fungemia was -C. auris 77.77% (7/9); rest were C. albicans 11.11% (1/9) and T. asahii 11.11% (1/9)
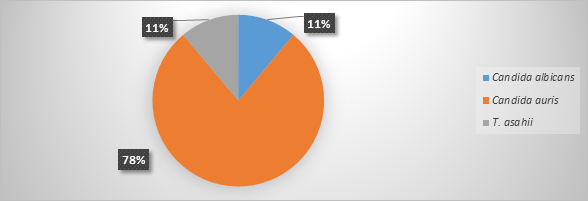
Figure 1: Causative agents of Fungemia in patients with CCI
Results of urine cultures in patients with CCI:
Total number of non-duplicate urine samples received during the peak of 2nd wave were 829. The prevalence of UTI among Covid-19 infected patients was found to be 18.09% (150/829). Prevalence of UTI by YYLF was found to be 32% (48/150). Growth with double isolates were 11 (7.33%), while the rest 139 (92.66%) had single isolate. Out of all fungal isolates, the predominating one was C. auris, 35.42% (17/48) followed by Trichosporon asahii, 25% (12/48).
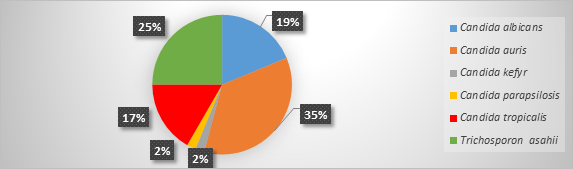
Figure 2: Causative agents of Yeast and Yeast like fungus in patients with CCI
Common isolates in Blood and Urine in patients with CCI:
Out of total 487 admitted cases, 16 (3.28%) patients had common isolates in both blood and urine samples.
Out of these, samples with common fungal and bacterial isolates were 56% (9/16) and 44% (7/16) respectively. The predominant fungus causing common infections include C. auris 78% (7/9).
Out of total nine cases with common causative organisms for BSI and UTI, seven had line related UTI prior to BSI which can be labelled as fungal urosepsis (FUS). Causative agents of FUS include C. auris 71.43% (5/7), C. albicans 14.28% (1/7) and T. asahii 14.28% (1/7).
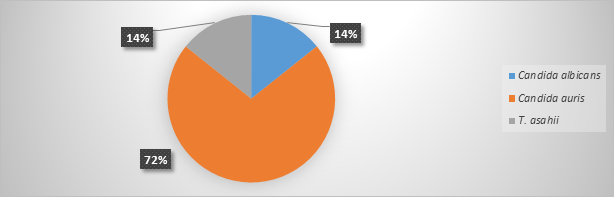
Figure 3: Causative agents of fungal urosepsis in patients with SIC
Demographic profile of CCI with urosepsis:
Out of seven cases, six (85.71%) belonged to elderly age group >=60 years with male to female ratio 5:2. All the patients with FUS with SCI with history of prolonged intensive care unit (ICU) stay (>10 days) with comorbid condition like diabetes mellitus (DM) (57.14%) and hypertension (HTN) (57.14%). All of them (100%) were catheterized and were on central lines. Out of the 7 patients, 5 (71.43%) were on mechanical ventilator. All the seven patients were given prolonged broad-spectrum antibiotics, steroids and immunomodulators. The mortality rate, 71.43% (5/7) was high among these patients.
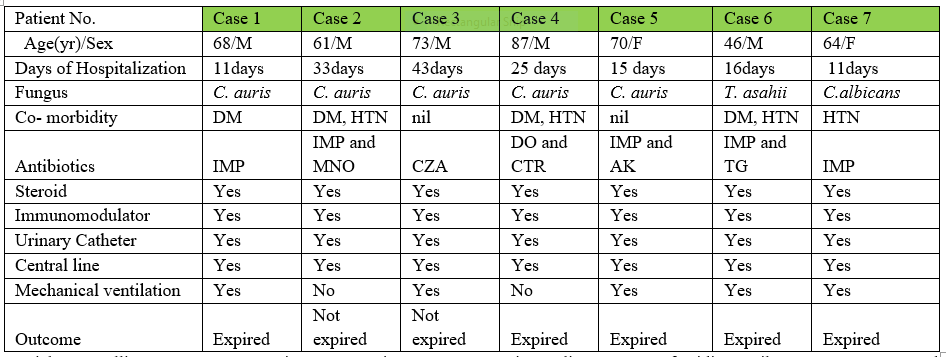
Table 1: Demographic profile of patients with SIC with FUS
| Patient No. | Case1 | Case2 | Case 3 | Case 4 | Case5 | Case 6 | Case7 |
| Lymphocytes (20-40%) | 4.7 | 30.9 | 21.6 | 13.9 | 7.2 | 3.9 | 6.3 |
| TLC (4.2-11.0 10x3/mm3) | 18.6 | 6.7 | 3.6 | 11.9 | 3.8 | 15.4 | 18.6 |
| Hb (13-17 g/dl) | 14 | 9.6 | 8.9 | 11 | 8.8 | 13 | 10 |
| D. Dimer(< 500ng/ml) | 1449 | 502.30 | 4295.61 | 3108 | 1617.45 | 4246 | 3019 |
| LDH (120-246 U/L) | 955.6 | 980 | 736.1 | 888 | 671 | 699.6 | |
| Ferritin (6.24-246 U/L) | 3110 | 537 | 429 | 699 | 734 | 2240 | 293 |
| PCT (<0> | 0.49 | 0.18 | 0.41 | 0.21 | 13.5 | 0.07 | 0.91 |
| CRP (<10> | 44.7 | 40.88 | 249 | 59.7 | 323.9 | 22.97 | 3.12 |
| Urea (15-36 mg/dl) | 103.4 | 57.4 | 44.8 | 35.8 | 37.7 | 105 | 138 |
| Creatinine (0.5-1.04 mg/dl) | 0.88 | 0.54 | 0.21 | 0.7 | 0.68 | 1.59 | 0.95 |
| Alk phosphatase (38-126 U/L) | 69.7 | 84.9 | 90.5 | 111.5 | 215.5 | 159.5 | 60.8 |
Ct- value of ORF-1a genein PCR for Covid-19 test |
17 |
21 |
29 |
24 |
22 |
24 |
23 |
Table 2: Laboratory parameters of patients with SIC with FUS
Note: Covid markers (serum ferritin, CRP, D. Dimer, LDH, Alkaline phosphatase) were elevated in all the patients.
Antifungal susceptibility pattern (AFSP) of Fungal isolates:
C. auris isolates were 100% resistant to fluconazole (Minimum inhibitory concentration, MIC >32 mg/L) and voriconazole (MIC >1 mg/L); however, 100% sensitive to caspofungin (MIC 0.25) and micafungin (MIC <0>T. asahii was susceptible Amp B and C.albicans was sensitive to all antifungals.
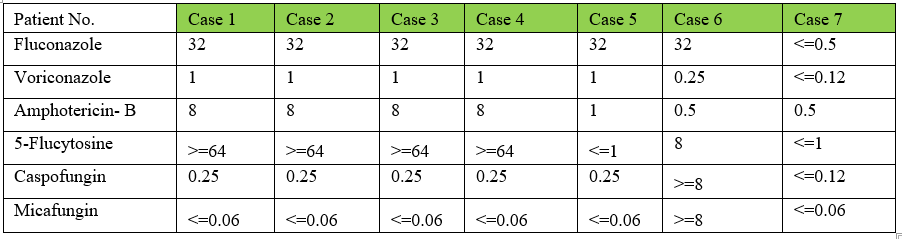
Table 3: MICs Antifungals for YYLF causing urosepsis in patients with SIC
SARS- CoV positive patients had 20
Secondary BSIs and UTIs were quite common in SARS-Cov-2 infected patients. Prevalence of coinfections and superinfections were negligible in literatures in the early part of the pandemic. This may be because of the scare associated with the disease, burden on human resource in health care, improper guideline to process secondary infections apart from Covid-19 itself, drawbacks of donning of PPE for prolonged period etc. Elderly patients with high risk factors and associated comorbidity were mostly succumbed to MDR YYLF infections; many leading to urosepsis with high mortality rate. Covid-19 virus itself and its management were favourable conditions for IFI. Therefore, prompt diagnosis and treatment are imperative with respect to secondary infections. Diagnostic stewardship associated with antibiotic stewardship along with proper infection measures are the tools to decolonize the MDR YYLFs in health care.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
