
Case Report | DOI: https://doi.org/10.31579/2690-4861/136
*Corresponding Author: Ikrame Boumendil, Faculty of Medicine and Pharmacy, Department of Otolaryngology and Head and Neck Surgery, Mohammed V University, Rabat, Morocco.
Citation: I Boumendil, H Taleb, O Bouanani, K Ayyad, M Boulaades. (2021) Mucormycose Rhino-Orbito-Cerebrale: Bonne Evolution. International Journal of Clinical Case Reports and Reviews. 8(1); DOI: 10.31579/2690-4861/136
Copyright: © 2021 Ikrame Boumendil, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 15 March 2021 | Accepted: 28 July 2021 | Published: 02 August 2021
Keywords: rhino-orbito-cerebral; mucormycosis; fungal infection; rhinosinusitis
Mucormycoses are opportunistic, rare, aggressive, often rapidly fatal infections caused by fungi of the zygomycete class. They are most often associated with decompensated diabetes or immunosuppression. They manifest themselves in different forms, the rhino-cerebral localization of which is the most frequent. The early diagnosis of this affection is essentially based on the histopathological analysis. Therefore, it must be evoked and sought by biopsies in any diabetic or immunocompromised patient suffering from complicated rhinosinusitis. We present in this work the case of a 14-year-old patient who suffered from rhino-orbito-cerebral mucormycosis successfully treated in our department of otolaryngology and head and neck surgery.
First described in 1885 by Paltauf, mucormycosis is a rare and fatal fungal infection. It is due to ubiquitous saprophytic organisms of the class of zygomycetes frequently found in soil and plant compositions [1]. This infection has been described at the pulmonary, gastrointestinal, cutaneous or disseminated level. The rhino-orbito-cerebral localization (ROC) is the most frequent [2], it presents 70% of the cases. ROC mucormycosis is invasive, often with a fulminant course, responsible for high mortality and significant neurological and aesthetic sequelae. It is often observed in diabetic or immunocompromised patients [3]. The diagnosis is based on the pathological examination and the prognosis depends on the speed of treatment. In this article, we report on the case of a 14-year-old girl treated for rhino-cerebral mucormycosis in order to discuss the diagnostic approach and therapeutic modalities in order to improve the prognosis of this infection.
Young patient aged 14, from a family living in a rural area with an unfavorable socio-economic level, with no known medical-surgical history, who for three days showed headaches in helmets with fever and vomiting resistant to symptomatic treatment . The installation of consciousness disorder in children required hospitalization in the emergency department of the provincial hospital where high capillary blood sugar and the presence of glycosuria and ketonuria were in favor of a decompensation in ketoacidosis mode inaugural of a diabetes not known. Faced with the modest improvement under rehydration and insulin therapy as well as the observation of facial asymmetry with the appearance of right periorbital edema, the patient was transferred to our department for treatment.
The ENT examination showed hypoaesthesia and paralysis of the right hemiface grade V according to the House and Brackmann classification, a right para-latero-nasal necrotic ulceration and bulging at the level of the right hemipalais centered on a fistulous path, a painful right periorbital edema; as well as two swelling on the right, painful with inflammatory signs on the temple and cheek (Figure 1). Endoscopic examination revealed the presence of thick purulent secretions, necrosis of the right inferior and middle turbinates, the septum, and the ethmoid-sphenoidal recess.

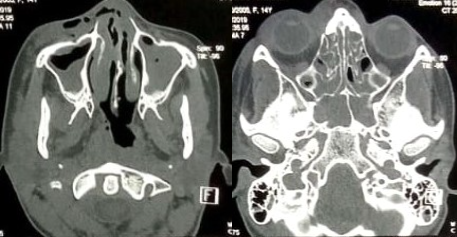
Computed tomography (CT) and magnetic resonance imaging (MRI) were performed showing aggressive pansinusitis with multiple micro-abscesses of the deep spaces of the face and right temporal lobe with thrombophlebitis of the right cavernous sinus (Figure 2).
Biopsy samples revealed mycelial filaments of the mucormycosis type. A nasal swab was carried out several times with negative mycological examinations, the bacteriological examination isolated a Pseudomonas aerogenosa. The diagnosis of mucormycosis following inaugural ketoacidosis decompensation was retained.
The patient underwent wide surgical removal of necrotic tissue with anteroposterior ethmoidectomy and right middle meatotomy via endoscopic endonasal approach associated with drainage of the collected abscesses. Faced with the unavailability of Amphotericin B, the patient was put on intravenous Voriconazole at a rate of 6 mg/kg / 12h on the first day, then 4 mg/kg/day associated with antibiotic therapy adapted to the antibiogram.
The patient was in intensive care for a week until the blood sugar levels normalized. After a total of 14 weeks of treatment, a marked clinical and biological improvement was observed and the young patient was discharged from the hospital. 12 months later, she was re-hospitalized for reconstruction of the loss of nasal substance.
Under general anesthesia, we performed a jugal advancement flap with nasal symmetrization plasty. The intraoperative result was satisfactory with placement of 2 merocel wicks under antibiotic cover (Figure 3a). We performed daily vaseline care and the wicking was maintained for a period of 15 days (Figure 3b).

After an 8-month follow-up, the postoperative aesthetic result was deemed satisfactory and the patient did not show signs of reinfection.
Mucormycosis is a rare, opportunistic and often fatal condition. It can occur at any age without gender preponderance [4]. It occurs preferentially in a field of immunosuppression: chronic renal infection (14%), corticosteroid therapy (5-6%), leukemia, cancer, AIDS, cirrhosis, system disease and mainly during unbalanced diabetes (60-80%). diabetes is sometimes discovered during infection, as is the case with our patient. Healthy subjects are exceptionally affected [5].
The natural history of the disease is well known. After inhalation of the spores, the germ first develops at the rhino-sinus level, then orbital and the deep spaces of the face and finally the cavernous compartment [6]. The mode of propagation can be by contiguity, perivascular or peri-neural. Fungal agents (phycomycetes) have angio-invasive potential. They cause tissue infarction and thus hypoxia and acidosis, further promoting fungal proliferation [7].
The orbit is invaded early by contiguity or by damage to the ethmoid and sphenopalatine vessels. This localization is manifested by periorbital edema of elastic consistency, quickly complicated by ophthalmoplegia, chemosis and reduced vision leading to blindness [8].
Several modes of propagation are responsible for brain damage. It has a very poor prognosis, manifested by restlessness, confusion, euphoria, seizures, and drowsiness that can progress to coma [8].
Bone invasion is late and rare in ROC mucormycosis [7].
At an early stage the diagnosis is difficult. The symptoms are non-specific: fever, headache and rhinorrhea. The rapid development over a few hours or days with the appearance of necrotic pressure ulcers in the ENT sphere are very suggestive [5].
Imagery is nonspecific, nonetheless it is crucial. Computed tomography (CT) and magnetic resonance imaging (MRI) make it possible to evoke the diagnosis, to specify the extension of the infection as well as to look for complications at a distance such as infarction, hemorrhage, aneurysms or abscesses [7].
The definitive diagnosis is based on microbiological and pathological examination. Cultures are done on Sabouraud media but they are difficult and rarely positive. Thus, early diagnosis is based on microscopic examination, large and deep biopsies, revealing typical mycelial filaments obstructing arteries, veins and sometimes nerve structures [7].
The treatment of rhino-orbito-cerebral mucormycosis is medico-surgical. The removal of all necrotic tissue involves an endonasal approach by endoscopic route or; in advanced forms; radical mutilating surgery extended to the base of the skull with orbit exenteration if necessary [10]. Medical treatment is based on high dose intravenous antifungals; Amphotericin B is the treatment of choice at 1-1.5 mg / kg / day for a minimum of 12 weeks. The treatment of contributing factors, in particular the control of diabetes, is essential [7]. In our patient, we had recourse to voriconazole which is ineffective in cases of mucormycosis according to the literature. Hyperbaric oxygen therapy has been proposed but has not yet been validated [11].
The prognosis depends on the early diagnosis and the initiation of treatment. Therapeutic progress has made it possible to reduce the mortality from this infection. Nevertheless, the prognosis remains poor in brain damage with a high frequency of neurological sequelae and a death rate between 20 and 50% [7].
Rhino-orbito-cerebral mucormycosis (ROC) is a serious and potentially fatal fungal infection. These infections occur most often in immunocompromised patients and can progress rapidly. Although rare, ROC Mucormycosis should always be considered in the event of rhino-sinus, orbital or cerebral symptoms, especially in a patient with unbalanced or immunocompromised diabetes. Only early diagnosis by pathological examination followed by appropriate medico-surgical treatment will improve the prognosis of this formidable infection.
The authors declare no conflict of interest.
All the authors contributed to this work. They read and approved the final version of the manuscript.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
