
case Report | DOI: https://doi.org/10.31579/2690-8794/252
1Department of Radiology, Gombe State University, Gombe State, Nigeria.
2Department of Radiology, Modibbo Adama University, Adamawa State, Nigeria.
3Department of Radiology, Usman Danfodiyo University, Sokoto State, Nigeria.
*Corresponding Author: Aminu Umar Usman, Department of Radiology, Gombe State, University, Gombe State, Nigeria
Citation: Usman A. Umar, Dahiru M. Yunusa, Sule M. Baba, (2025), MRI finding of Rathke Cleft Cyst in a 35-Year Old African Woman: A Case Report, Clinical Medical Reviews and Reports, 7(1); DOI:10.31579/2690-8794/252
Copyright: © 2025, Aminu Umar Usman. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 13 February 2025 | Accepted: 20 February 2025 | Published: 27 February 2025
Keywords: Rathke Cleft cyst; Pituitary gland; Magnetic Resonance Imaging
Rathke cleft cysts (RCC) are non-neoplastic cysts arising from the embryonic reminants of Rathke pouch of the pituitary gland primarily occupying the sellar space but can have suprasellar extension. Clinically it poses a diagnostic challenge as the symptoms may mimic other sellar and juxtasellar lesions. Magnetic Resonance Imaging (MRI) is the mainstay imaging modality for its diagnosis.
The case presented is RA, a 35-year old woman with recurrent headache, poor vision, amenorrhoea, loss of libido and occasional galactorrhea. MRI revealed expansion of the sella with a well-defined fairly rounded rim enhancing lesion measuring 15 X 14 X 15mm (width X AP X H) with compression of the optic chiasma. She was placed on homonal theraphy with remarkable improvement of symptoms and referred to Neurosurgeons for definitive treatment.
Rathke cleft cysts (RCC) also known as pars intermedia cysts are non-neoplastic cysts arising from the embryonic reminants of Rathke pouch of the pituitary gland[1]. Thus they develop as cystic lesions located between the anterior and posterior lobes of the pituitary gland[1]. They occupy the sellar space, but can have suprasellar extension.
They are common incidental findings in 11–22 % of autopsies [2-4]. Their peak incidence falls between the fourth and the sixth decade of life. They are three times more frequent among women [5]. It is rarely seen in childhood3.
Usually, vast majority of Rathke cleft cysts are asymptomatic when less than 3mm in size [6]. When large, the typical symptoms include headache, visual loss and endocrinologic dysfunction [7-8].
Magnetic Resonance Imaging (MRI) is the primary diagnostic technique for RCC due to its high soft tissue resolution [9]. It also determines the cystic content and fluidity of the cyst which is useful in for subsequent patient’s management [10].
Symptomatic RCC require surgical excision. Patients should be monitored for at least five years following surgery as the risk of recurrence may even reach 50%1. Radiotherapy may prove effective in the treatment of recurrent RCC [11]. Asymptomatic cases however require observation and serial monitoring [12-13].
Mrs RA, a 35-year woman who was referred from a private hospital facility in Yola for a brain MRI with One-year history of recurrent headache which was dull aching in nature initially frontal and later became generalised with associated poor vision. She also has amenorrhoea for three months with marked reduction in libido. There is occasional galactorrhea. No heat or cold intolerance. No convulsion or loss of consciousness.
Physical examination was within normal limit. Visual examination revealed loss of vision in the outer (temporal) halves of the visual fields. Visual acuity and Fundoscopic examinations done were normal in both eyes.
Other cranial nerves assessment was normal. No lateralising sign or loss of muscle power.
Breast examinations revealed bilateral well developed breasts. No area of tenderness or palpable mass. However, breast milk was expressed on gentle pressure more on the right.
Hormonal assessment revealed hyperprolactinaemia with serum prolactin of 380ng/dl (normal value is 5 – 40ng/dl). Other systemic examinations were also normal.
Complimentary skull x-ray (Occipitofrontal and lateral views) show normal cranial vault, sutures and sella tursica. No craniofacial disproportion is noted.
Magnetic Resonance Imaging (MRI) revealed expansion of the sella with a well-defined fairly rounded lesion measuring 15 X 14 X 15mm (width X AP X H). It is hypointense on T1W, hyperintense on T2W and suppressed on FLAIR sequence. Rim enhancement is seen post contrast. The mass is inseparable from the optic chiasma suggestive of compression.
Radiological diagnosis of Rathke cleft cyst was made with a differential of Cystic pituitary macroadenoma.
Patient was placed on Bromocriptin tablets with remarkable improvement of the galactorrhea and normalisation of the prolactin level. She was also referred to the gynaecologist for the menstrual irregularity and a private Neurology centre in Lagos for definitive treatment of the primary Rathke’s cleft cyst.

Figure 1: Axial T1W image of the brain showing a hypointense rounded intrasellar mass lesion (white asterisk).

Figure 2: Axial T2W image of the brain showing a hyperintense rounded intrasellar mass lesion (black asterisk).

Figure 3: Axial T1W post contrast image of the brain showing a marginal (rim) enhancement of the hypointense rounded intrasellar mass lesion (white arrows).
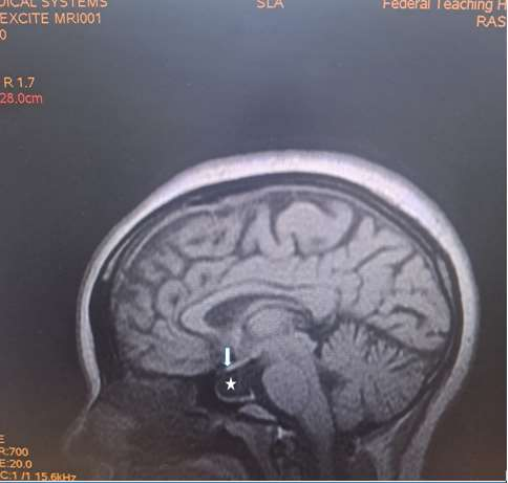
Figure 4: Sagittal T1W image of the brain showing a hypointense rounded intrasellar mass lesion (white asterisk) with obliteration of the optic chiasma (white arrow).
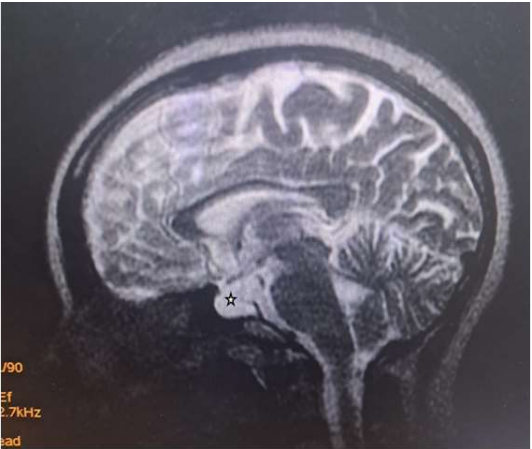
Figure 5: Sagittal T2W image of the brain showing a hyperintense rounded intrasellar mass lesion (black asterisk).
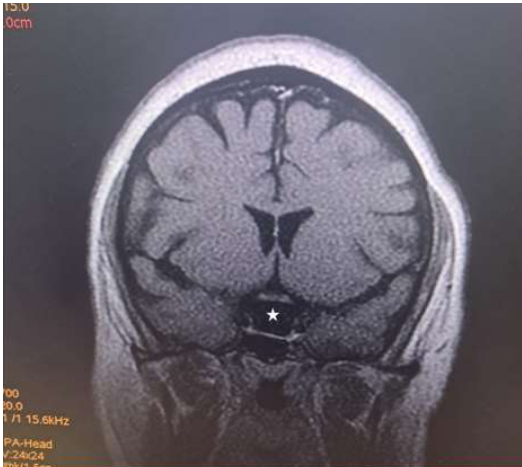
Figure 6: Coronal T1W image of the brain showing a hypointense rounded intrasellar mass lesion (white asterisk).
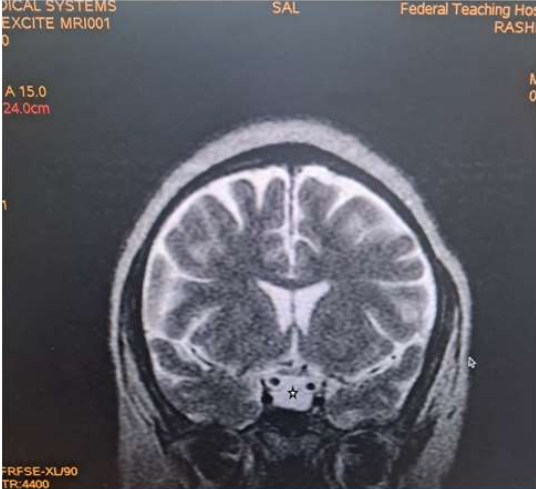
Figure 7: Coronal T1W image of the brain showing a hyperintense rounded intrasellar mass lesion (black asterisk).
Rathke cleft cysts (RCC) are non-neoplastic cysts arising from the embryonic reminants of Rathke pouch of the pituitary gland. They occupy the sellar space, but can have suprasellar extension1.
Their peak incidence falls between the fourth and the sixth decade of life and are three times more frequent among women [5]. It is rarely seen in childhood3. RCC are common incidental findings in 11–22 % of autopsies [2-4]. The case presented was a 35- year old female which falls in the frequent age group of the disease.
Clinically, majority of lesions less than 3mm are asymptomatic6. However, when large, the typical symptoms include headache, visual loss and endocrinologic dysfunction7,8. The case presented had recurrent headache, poor vision, amenorrhoea, loss of libido and occasional galactorrhea. No heat or cold intolerance. No convulsion or loss of consciousness. The headache seen is due to raised intracranial pressure from the mass which is non-specific. It may also be due to cyst wall infarction, haemorrhage or leakage of inflammatory contents14. The poor vision seen is due to compression of the optic chiasma by the cyst, while the amenorrhoea, loss of libido and galactorrhea are the result of the endocrine dysfunction usually seen in the disease [16].
Differential diagnosis of The differential diagnoses of Rathke’s cleft cyst includes: Cystic pituitary adenoma, craniopharyngioma, empty sella syndrome and metastasis [17].
Skull radiographs usually show non-specific features of raised intracranial pressure which include widening of the sella tursica, increased convolutional markings, sutural widening and increased head size due with craniofacial disproportion in favour of the cranium. The skull x-ray of the case presented was however normal.
RCC on Computed Tomography (CT) typically present as a Hypodense sella or suprasellar mass. Cyst wall giving ring enhancement may be present especially with inflammation of the cyst [18]. Wall calcification is seen in 10-15% of cases.
Rathke’s cyst is visualised on magnetic resonance imaging as a lesion located in the intermediate lobe of the pituitary. Its largest diameter usually does not exceed 20 mm9. The cyst may have varying intensity against the cerebrospinal fluid, although it is more often hypointense in T1-weighted images and hyperintense in T2-weighted images. RCC image captured on MRI is described as “an egg in a shell [9]. The enhancement of the cyst wall following contrast administration suggests inflammation or metaplasia [11].
Due to its high soft tissue resolution, Magnetic Resonance Imaging (MRI) is the primary diagnostic technique for RCC9. It also determines the cystic content and fluidity of the cyst which is useful in planning for subsequent patient’s management10. Fifty percent are hyperintense on T1W (due to high protein content) while 50% are hypointense. On T2W, 70% are hyperintense, 30% iso or hypointense and 20% have hypointense rim. T1W Post contrast images usually show no enhancement. However, a thin enhancing rim may be seen when cyst wall infection is present [19-20]. The case presented revealed expansion of the sella with a well-defined fairly rounded lesion measuring 15 X 14 X 15mm (width X AP X H). It is hypointense on T1W, hyperintense on T2W and suppressed on FLAIR sequence. Rim enhancement is seen post contrast. The mass is inseparable from the optic chiasma suggestive of compression. The appearance of the cyst confirmed no haemorrhage or debris within the cyst. However, the rim enhancement suggest inflammation of the cyst as explained in the text. The finding of optic chiasma compression may explain the visual impairment and the bitemporal hemianopia seen in the patient.
Definitive treatment modalities for large symptomatic RCC include surgical excision and Radiotheraphy11. Hormone replacement therapy is used in patients with endocrine dysfunction. Asymptomatic cases however require observation and serial monitoring [12-13]. The presented patient was placed on Bromocriptin tablets with remarkable improvement of the galactorrhea and normalisation of the prolactin level.
Rathke cleft cysts (RCC) are non-neoplastic cysts of the sellar which may extend to the suprasellar region presenting with features of raised intracranial pressure, optic pathway compression and endocrine dysfunction. MRI due to its high soft tissue resolution plays an important role in its diagnosis and follow up. Most cases in our environment are under reported or missed due to non-availability of functional MRI or high cost of the study.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
