
Research Article | DOI: https://doi.org/10.31579/2768-2757/099
1 University Clinic of Traumatology Orthopedics and Reconstructive Surgery (CUTO-CR) of the National Hospital and University Center Hubert Koutoukou Maga (CNHU-HKM) of Cotonou (Bein).
2 University Clinic of Physical Medicine and Rehabilitation (CUMPR) of the National Hospital and University Center Hubert Koutoukou Maga (CNHU-HKM) of Cotonou (Bein).
*Corresponding Author: Goukodadja Oswald, Hervé Djidjoho 01 BP 1455 Cotonou (Bein).
Citation: Goukodadja O, Vodounnon S, Assogba F, Padonou A., Chigblo P., et al, (2023), Mortality, Morbidity and Quality of Life of Patients Operated on By Intermediate Hip Prosthesis for Femoral Neck Fracture in Cotonou, Journal of Clinical Surgery and Research, 4(6); DOI:10.31579/2768-2757/099
Copyright: © 2023, Goukodadja Oswald. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 13 November 2023 | Accepted: 24 November 2023 | Published: 05 December 2023
Keywords: fracture; femoral neck; intermediate hip replacement; quality of life; morbidity level of evidence iv
Introduction: Femoral neck fractures are common in the elderly. Without early, multidisciplinary management, patients are exposed to high morbidity and mortality rates. The use of an intermediate hip prosthesis has emerged as a safe treatment option. Does this surgical procedure improve patients' prognosis and quality of life?
Objective: To study the functional outcome and quality of life of patients operated on with an intermediate hip prosthesis (IHP) for a fracture of the neck of the femur.
Materials and method: This was a descriptive and analytical cross-sectional study with retrospective data collection. The target population consisted of patients who had undergone intermediate hip replacement for femoral neck fracture at the CNHU-HKM in Cotonou over a 13-year period from 1 January 2009 to 01 December 2021. Patients were reviewed. Hip function was assessed using the Postel-Merle d'Aubigné (PMA) score. The Short Form Survey (SF-12) was used to assess quality of life. Data were analysed using Chi-square tests (significance level p < 0.05) and Student's t test. Odds ratios were calculated with confidence intervals using Epi info version 7.2.5 software.
Results: A total of 86 patients were included in the study. The mean age of the subjects was 68.54±13.25 years, with a male predominance (65.1%) and a sex ratio of 1.86. Postoperative complications were observed in 47 patients (54.7%). Death occurred in 15 patients (17.4%). In terms of quality of life, the mean physical SF-12 was 50.28±5.24 (32.09-55.92) and the mean mental SF-12 was 59.54±2.4 (50.76-64.52). The mean PMA score at the last follow-up was 16.54±1.39 (13-18). Statistically significant associations (p-value < 0.05) were found between quality of life and age, quality of life and PMA score at last follow-up.
Conclusion: Placement of an intermediate hip prosthesis reduce the disability resulting from femoral neck fractures, which has a positive impact on patients' quality of life.
In the elderly, femoral neck fractures are mainly continuity fractures, favoured by osteoporosis, and most often occur after a simple, clumsy fall [1]. In young adults, on the other hand, they are caused by high-energy trauma, such as road accidents [2]. The incidence of fractures is increasing, and is expected to double every 20 years as the population ages [3]. The vital prognosis after a femoral neck fracture is poor, with a one-year mortality rate of between 16 percentage and 29 percentage in numerous studies [4]. It is also associated with a high morbidity rate, and disability that significantly affects quality of life [1, 5, 6]. Indeed, many authors have shown that femoral neck fractures have a negative impact on quality of life and activities of daily living in men and women of all ages [10, 11]. This shows that femoral neck fractures are a genuine public health problem [3]. Early, multidisciplinary management of femoral neck fractures could improve prognosis and preserve patients' quality of life [1]. Patients who do not undergo surgery for their femoral neck fracture have a 4-fold higher risk of death at 30 days and 1 year than patients who do undergo surgery for their fracture [1]. This treatment begins with a hemiarthroplasty, which is the technique of choice because of its advantages: rapid intervention, lower cost, stability and early walking ability [7; 8]. Functional re-education also plays an important role in this treatment, as it is an essential complement to optimal functional recovery for patients [9]. In northern countries, the various clinical, therapeutic and prognostic aspects of femoral neck fractures have been widely discussed. We have not found any studies evaluating the quality of life of patients who have undergone surgery. The research hypothesis is that quality of life is impaired in patients undergoing intermediate hip replacement surgery for femoral neck fractures in Cotonou. The aim of this study was to investigate the functional outcome and quality of life of patients operated on for an intermediate hip prosthesis (IHP) after a fracture of the neck of the femur.
This was a descriptive and analytical study with retrospective data collection in two departments of the Centre National Hospitaller et Universitaire Hubert Koutoukou MAGA de Cotonou (CNHU-HKM) in Cotonou: The University Clinic of Traumatology-Orthopedics and Reconstructive Surgery (CUTO-CR), and the University Clinic of Physical Medicine and Rehabilitation (CUMPR). The population consisted of all subjects who had undergone an intermediate hip replacement for a fracture of the neck of the femur over a 13-year period from 1 January 2009 to 1 December 2021. About inclusion criteria, all patients with a complete medical file including pre- and post-operative X-rays, biological work-up, outpatient, CUTO-CR and CUMPR follow-up forms were included in our study. A minimum post-operative follow-up of six (06) months was retained. Patients with comprehension problems that made assessment difficult, patients with associated musculoskeletal injuries (fractures, dislocations, nerve or vascular injuries) or patients with pathological femoral neck fractures were not included. In this study, the only dependent variable was quality of life. This was assessed by the Short Form Survey (SF-12). It combines two global health scores: the Physical Component Smmary (PCS) and the Mental Component Summary (MCS), each scored out of 100. The SF-12 consists of twelve (12) items divided into eight dimensions: physical function, physical limitations, physical pain and general state of health help to determine the PCS, while life and relationships with others, mental health, limitations due to emotional state and vitality determine the MCS. A score above 50 corresponds to average quality of life, a score between 40 and 49 to mild disability, a score between 30 and 39 to moderate disability and a score below 30 to severe disability [10]. The Postel-Merle d'Aubigné (PMA) score was used to assess pain, joint mobility and walking function. Overall results were considered as follows: excellent = 18; very good = 17; good = 16 or 15, fair = 14 or 13; poor = 12, 11 or 10; bad = less than 9 [11]. Chi-square test (significance level p less than 0.05) was used to compare frequencies and means respectively. From an ethical point of view, a complete file was also submitted for the opinion of the Ethics and Research Committee in Health Sciences of the Faculty of Health Sciences in Cotonou.
Of the 101 files listed, only 94 were found in the archives of the CNHU-HKM. Among them, eight patients were excluded because of the comprehension problem and associated injuries, thus reducing the series to 86 patients. The average age of the patients was 68.54±13.25 years, with extremes of 31 and 96 years. The most common age group was 65 and over. Males were the most represented, with 56 men (65.1percentage) and 30 women (1.86 gender ratio). Retired people were the most numerous in our series, with 44 (51.2percentage). Arterial hypertension was the most common comorbidity in 38 patients (44.2percentage). The mean Body Mass Index (BMI) was 22.64±4.10 kg/m², with extremes of 18.14 kg/m² and 33.17 kg/m². The most common range was between 18.5 kg/m² and 25 kg/m². The most frequent etiological circumstance was a fall at home in 54 patients (62.8percentage). The average age of patients who fell at home was 73.68±11.18 years. This was followed by accidents on the public highway in 28 patients (32.6percentage). The average admission time was 29.09±50.94 days, with extremes ranging from 0 to 321 days. According to the Garden classification, the most common type of femoral neck fracture was type IV in 70 patients (81.4percentage). The average operating time was 41.18±51.28 days, with extremes of four and 326 days. Almost half the patients had undergone surgery after the first month following hospitalisation (41.9percentage). Post-operative functional rehabilitation was followed by 68 patients (79.1percentage). The average number of rehabilitation sessions was 17.73±14.20, with extremes of five and 90 sessions. Postoperative complications occurred in 47 patients (54.7percentage). Table 1 shows the complications of the patients in our series. The most frequent complication was surgical site infection. The mean time to onset of this surgical site infection was 20.25±43.39 days, with extremes ranging from seven to 180 days. Pressure sores were the most frequently encountered decubitus complication. The mean time to onset was 15.57±14.36 days, with extremes ranging from three to 45 days.
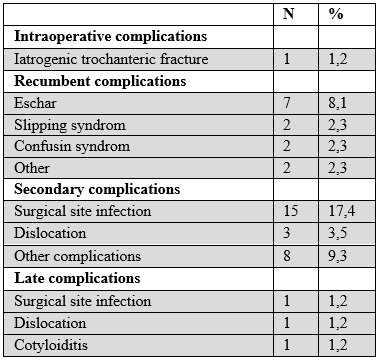
Table 1: Distribution of complications recorded in patients operated on by PIH for a fracture of the neck of the femur
Mortality
Death occurred in 15 patients (17.4percentage). The mean postoperative time to death was 1.68±1.66 years, with extremes ranging from 14 days to 1760 days, i.e., four years and nine months. The death rate at one year post-operatively was 9.3percentage.
Evaluation
Patients were reviewed at a mean follow-up of 2.84±2.78 years, with extremes ranging from seven months to 12 years and 11 months. The mean PMA score at the last follow-up was 16.54±1.39 with extremes ranging from 13 to 18. A good to excellent score was found in 88.2% of patients. Figure 1 shows the results of the Short Form Survey (SF-12) assessment of patients' quality of life after PIH. The mean SF-12 mental score was 59.54±2.43 with extremes ranging from 50.76 to 64.52. All patients in the series had a mental score above 50. The mean SF-12 physical score was 50.28±5.24, with extremes ranging from 32.09 to 55.92. The highest proportion of patients had a mental score above 50.
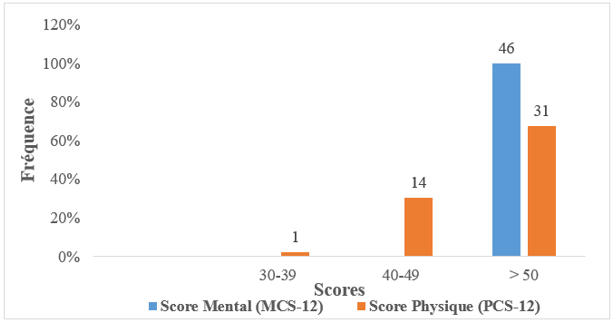
Figure 1: Distribution of patients operated on by PIH for a fracture of the neck of the femur according to their quality of life using the Short Form Survey (SF-12).
There was a statistically significant association between age and the physical dimension of quality of life (p-value=0.002) and between the PMA score at the last recoil and the physical dimension of quality of life (p-value less than 0.001). On the other hand, there was no statistically significant association between comorbidity and the physical dimension of quality of life (p value=0.1560), between post-operative complications and the physical dimension of quality of life (p value=0.3825), between the existence or not of post-operative complications and the operating time (p value=0.7763), between the occurrence or not of death and the operating time (p value=0.4915).
The sex ratio of our study population was 1.86, indicating a male predominance. Our results are similar to those of Chigblo et al [12] who found a gender ratio of 1.7. The same is true of Kardali et al [13] and Monk M. et al [3] who found gender ratios of 1.2 and 1.5 respectively. The majority of our patients were elderly, with an average age of 68.54 ± 13.25 years. This could be explained by the fact that this part of the population has osteoporotic bone fragility. This result is in line with the observations of many authors who have stated that femoral neck fracture is a pathology of the elderly [1, 3]. Chigblo et al. in Benin in 2017 [12] and Monk M. et al. in 2016 in Congo [3] found mean ages of 64 and 71 years respectively. These results are lower than those found by Kardali et al. in 2012 in Morocco, who obtained an older population with a mean age of 75 years [13]. Most of the patients were retired. This could be related to the main aetiology of femoral neck fractures, which is falls at home, mainly affecting elderly subjects. In terms of co-morbidities, arterial hypertension was the most common. This could be linked to ageing and a poor lifestyle. Chronic pathologies are more likely to recur in old age. However, our result is much higher than that of Jameson et al (36.0%) in 2012 in the United Kingdom [14] and lower than that of Diaz et al (55.9%) in 2018 in Spain [15]. In our series, the mean BMI was 22.64 ± 4.10 kg/m², with a predominance of subjects with a normal BMI. BMI is an indicator of health status. An increase in BMI (BMI⋝ 25 kg/m²) indicates poor dietary habits and poor health. Health professionals therefore strongly recommend maintaining a normal BMI. On the one hand, this is to limit the rate of repeat operations linked to overloading of the prosthesis and peri- and post-operative complications, and on the other, to preserve the new joint in order to guarantee the best day-to-day results, the best quality of life and the longest survival of the hip prosthesis. The predominance of normal BMI in our series suggests that patients were informed of the risks of gaining weight on the prosthesis and therefore applied this advice. The mean BMI in our study is superposable with that of the studies by Matsumoto et al (20.86 kg/m²) in 2017 in France [16] and Ozaki et al (23.3 kg/m²) in 2018 in Japan [17]. In our series, falls at home were the main cause of fracture, accounting for 62.8% of cases. This aetiology could be explained by senile osteoporosis, gait disorders and balance problems, which are frequently found in elderly subjects. Our results are similar to those of Bergeron et al (58.2%) in 2006 in Canada [18]. Sanz-Reig et al [19] in Spain in 2012 found much better results than ours, with 82% of falls occurring at home. The long delay in admission could be explained by the usual itinerary in Benin of people injured on public roads in Cotonou, which is characterised by initial recourse to peripheral health establishments and more often to traditional therapists [12]. In our series, the fractures were very displaced overall (Garden type IV) in 81.4% of cases. This frequency is much higher than that of Kardali et al (51.02%) in 2012 in Morocco [13] and Foal S et al (64.3%) in 2005 in France [20]. However, it is lower than that found by Monk M. et al (87%) in 2016 in Congo [3]. Long operating times are a constant in countries with limited resources. It is related to the time needed to raise the financial means, as patients do not have health insurance or mutual health insurance. Early surgery (within 48 hours) after hip fracture would reduce mortality and decrease the risk of post-operative complications [21]. In the present study, although the operative delay was longer than that found in the literature, no statistically significant association was found between the operative delay and the occurrence or non-occurrence of death (p=0.4915) or postoperative complications (p=0.7763). Although long, this operating time is shorter than that found by Monk M. et al (305 days) [3] in 2016 in Congo. It is longer than that of Kardali et al [13], who obtained a mean operating time of 6.5 days. The majority of the population in the present study had undergone functional rehabilitation sessions, i.e., 79.1% of cases. About proprioceptive impairment after hip replacement, rehabilitation programmes after total hip replacement (THR) should be started as early as possible to prevent complications, which include deep vein thrombosis and dislocation, reduce pain levels, recover joint movement, muscle strength, tissue elasticity and start weight bearing early [22]. Hans-Moévi et al have argued that functional rehabilitation is an essential adjunct to surgery to restore satisfactory hip function after THR [23]. In terms of post-operative complications, the frequency of surgical site infections (SSI) could be explained by the presence of co-morbidities such as diabetes, but also by the long period of pre-operative hospitalisation. Our SSI rate is higher than that of Liu et al. in 2019 China [24] and Svenoy et al. in Norway in 2017 [25], who obtained SSIs in 7.58% and 6% of cases respectively. The same is true for de Jong et al (10%) [26] in 2017 in the Netherlands. This difference could be explained by their short operating time. As for mortality related to HSP after femoral neck fracture, our results are lower than those of Sanz-Reig et al. in 2012 in Spain (24.2%) [19] and Foal S. et al. in 2005 in France (18.2%) [20]. Similarly, Masoni et al. obtained a much higher result than our own, with 25.5% of deaths in 2021 in Italy [27]. The high death rates recorded elsewhere could be explained by the very advanced age of the subjects, who are at greater risk of postoperative complications, thus favouring the occurrence of death. The mean Postel et Merle d'Aubigné score at final follow-up was 16.54 ± 1.39. This result could be explained by the fact that fitting the prosthesis would reduce pain in the hip and allow the patient to regain joint mobility and walking ability. Our results are similar to those of Chigblo et al [12] and Poulain et al [20], who found a mean PMA score of 16.5 and 16.04 respectively. The same is true of Kassimi et al. in 2014 in Morocco [28], who found a mean PMA score of 14.8. Our results are superposable with those of Rahman et al. in 2013 in Canada [29] who found a mean mental SF-12 score of 57 ± 6 and a mean physical SF-12 score of 54 ± 6. Palazzo et al. in 2014 in France [30] obtained lower results than ours with mean mental and physical SF-12 scores of 44.1 ± 5.7 and 45.8 ± 6.8 respectively. The same is true for Gonzalez et al. in 2014 in Spain [31] who found mean mental and physical SF-12 scores of 43.34 ± 14.23 and 29.80 ± 7.08 respectively. About association between age and quality of life, our results are similar to those of Sprague et al (p<0.001) in 2018 in Canada [32] and Buecking et al (p<0.001) in 2014 in Germany [33]. The same is true of Rohde et al. in 2010 in Norway [34], who found a correlation between age and quality of life (p=0.015). In the present study, no statistically significant association was found between comorbidities and quality of life (p=0.1560). This could be explained by the fact that comorbidities are systematically monitored and managed by doctors from the moment patients are admitted in order to limit complications. This result is similar to that of Rohde et al (p=0.999) in Norway in 2010 [34].
Fractures of the neck of the femur have a poor prognosis. The aim of this study was to investigate the functional outcome and quality of life of patients who underwent intermediate hip replacement surgery for femoral neck fractures. The patients who underwent intermediate hip replacement after femoral neck fracture were mainly elderly retired people. Males were the most common. Arterial hypertension was the most common comorbidity. After PIH insertion, 88.2% of patients regained good hip function. This had a positive impact on their quality of life. However, advanced age was a prognostic indicator of poor quality of life after PIH. The most frequent post-operative complications were surgical site infections and pressure sores. The mortality rate in our series was 17.4%. It was 9.3% at one year follow-up.
none.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
