
Research Article | DOI: https://doi.org/10.31579/2578-8965/250
1Programa de Pós-graduação do Departamento de Ginecologia da Escola Paulista de Medicina da Universidade Federal de São Paulo (EPM/UNIFESP). São Paulo – SP, Brasil.
2Programa de Pós-graduação em Enfermagem da Universidade Federal do Piauí (PPGENF/UFPI). Grupo de Estudo, Pesquisa e Extensão na Saúde da Mulher da Universidade Federal do Piauí (GEPESM/UFPI). Piauí – PI, Brasil.
3Prefeitura de Jundiaí, Secretaria Municipal de Saúde de Jundiaí. São Paulo – SP, Brasil.
4Programa de Pós-Graduação em Saúde Coletiva da Faculdade de Medicina da Universidade de São Paulo (FMUSP). São Paulo – SP, Brasil. Ayfa Faculdade de Ciências Médicas de Itacoatiara. Amazonas - AM, Brasil.
5Faculdade de Enfermagem. Universidade Santo Amaro (UNISA). São Paulo – SP, Brasil.
6Faculdade de Enfermagem. Universidade Santo Amaro (UNISA). São Paulo – SP, Brasil.
7Facultad de Enfermería y Fisioterapia de la Universidad de Salamanca (USAL). Salamanca, Espanha.
8Escuela Universitaria de Enfermería de la Cruz Roja da Universidad Autónoma de Madrid (EUE/UAM). Madrid, Espanha.
9Programa de Pós-graduação do Departamento de Ginecologia da Escola Paulista de Medicina da Universidade Federal de São Paulo (EPM/UNIFESP). Faculdade de Medicina de Catanduva (FAMECA/UNIFIPA). São Paulo – SP, Brasil.
*Corresponding Author: Gustavo Gonçalves dos Santos, Gustavo Gonçalves dos Santos - Departamento de Ginecologia da Escola Paulista de Medicina da Universidade Federal de São Paulo. R. Napoleão de Barros, 608 - Vila Clementino, São Paulo – SP.
Citation: Dos Santos GG, Lara Beatriz de Sousa Coelho, Freitas Nascimento MV, Do Nascimento ES, Anderson Lima Cordeiro Da Silva, et al, (2025), Mortality in women of reproductive age belonging to the black and indigenous population associated with COVID-19 infection: integrative literature review, J. Obstetrics Gynecology and Reproductive Sciences, 9(2) DOI:10.31579/2578-8965/250
Copyright: © 2025, Gustavo Gonçalves dos Santos. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 08 November 2024 | Accepted: 18 November 2024 | Published: 05 February 2025
Keywords: literature review; covid-19; health inequalities; ethnic health disparities; maternal mortality
Aim: The study addresses racial and ethnic inequalities in maternal mortality during the COVID-19 pandemic.
Objective: The aim was to review the literature to describe the evolution and outcomes of COVID-19 among black and indigenous women of reproductive age.
Materials and Methods: An Integrative Literature Review was conducted, following six stages, including the definition of the research question, selection of studies in databases, and qualitative analysis using IRAMUTEQ software. Data sources included EMBASE, LILACS, PubMed and others, covering studies published from 2019 onwards.
Results: The results revealed that black and indigenous women had higher rates of serious complications and mortality from COVID-19, influenced by comorbidities such as hypertension and diabetes, as well as inequalities in access to healthcare.
Conclusions: The study addresses racial and ethnic inequalities in maternal mortality during the COVID-19 pandemic. The aim was to review the literature to describe the evolution and outcomes of COVID-19 among black and indigenous women of reproductive age.
The COVID-19 pandemic, caused by the Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) virus, has brought unprecedented challenges to global health, especially affecting vulnerable groups, including women of reproductive age, pregnant women and postpartum women[1]. Physiological and immunological changes during pregnancy may predispose pregnant women to more serious forms of viral respiratory infections, including COVID-19 [1]. Pregnancy is associated with changes in the immune system that can increase susceptibility to infections, and the presence of comorbidities such as gestational diabetes and hypertension can exacerbate the risks [2].
Maternal mortality associated with COVID-19 has been a growing focus of concern, given the potential adverse effects of the infection on maternal and neonatal health [3]. A study showed that women of reproductive age infected with SARS-CoV-2 have an increased risk of serious complications, including the need for intensive care and ventilatory support, and an increased likelihood of developing serious complications, including acute respiratory failure [4].
In the public health context, maternal mortality related to COVID-19 has highlighted significant disparities, with ethnic minority and socioeconomically disadvantaged women facing greater risks [5,6].
During the pandemic, the need for hospitalization and intensive care among women of reproductive age varied substantially, with peaks associated with outbreaks of more contagious variants, such as Delta and Omicron [7]. Data from a multicenter study indicate that the presence of comorbidities, such as obesity, hypertension and diabetes, significantly increases the risk of severe complications and Mortality [8].
In addition to comorbidities, socioeconomic and healthcare access factors play a crucial role in COVID-19 mortality among women of reproductive age. Inequalities in access to healthcare, including early diagnosis and timely treatment, have exacerbated disparities in health Outcomes [9]. Studies carried out in the United States and the United Kingdom have shown that black women and other ethnic minorities are disproportionately more likely to suffer serious complications from COVID-19 during pregnancy, reflecting systemic inequalities in access to quality healthcare [10].
The COVID-19 pandemic has had a disproportionate impact on several vulnerable populations, including Black and Indigenous women of reproductive age. Studies show that these women have faced higher rates of serious complications and mortality due to SARS-CoV-2 compared to their white counterparts. This disparity is attributed to a combination of pre-existing social, economic and health factors that amplify the risks associated with COVID-19 [10,11]. Black women of reproductive age have been particularly affected by the pandemic, with higher rates of hospitalization and Mortality [10-12]. The research by Lokken et al. (2021) indicated that black pregnant women are more likely to develop severe complications from COVID-19, such as the need for mechanical ventilation and intensive care [12]. This vulnerability is exacerbated by factors such as structural racism and economic inequalities that limit access to healthcare resources and exacerbate underlying conditions, such as hypertension and diabetes, that exacerbate COVID-19 infection [13]
Likewise, indigenous women of reproductive age have faced significant challenges during the pandemic. Studies show that indigenous communities have been disproportionately impacted by SARS-CoV-2, with infection and mortality rates substantially higher than the national Average [14]. The lack of adequate healthcare infrastructure in many indigenous areas, along with cultural and language barriers, contributes to lower quality and accessibility of healthcare [15]. The intersection of skin color, ethnicity, and socioeconomic factors is critical to understanding disparities in COVID-19 mortality among Black and Indigenous women of reproductive age. The literature highlights the urgent need to address these inequalities through public policies that guarantee equitable access to high-quality healthcare [16].
The mortality of women of reproductive age associated with SARS-CoV-2 highlights deep systemic inequalities that require immediate action, representing a public health crisis that demands immediate attention. Understanding the risk factors and consequences of infection during pregnancy is crucial to developing effective interventions, thus justifying this study, with the aim of carrying out an integrative review of the literature to describe the evolution and outcomes of COVID-19 among black and indigenous women of reproductive age.
Ethical considerations
As this was a review study that did not involve the collection of primary data, submission to the Research Ethics Committee was not necessary. However, ethical principles were respected when conducting the review. The procedures carried out to approach the object and operationalize the review are registered in Figshare (https://figshare.com/)under the identification of the Digital Object Identifier (DOI) accessible at: https://doi.org/10.6084/m9.figshare.26112769.
Type of study
Integrative Literature Review with a qualitative approach [17]. For its operationalization, six steps were followed, being: 1 - elaboration of the guiding question; 2 - definition of the sample, based on the establishment of criteria for inclusion/exclusion of studies and the search in scientific literature; 3 - data collection, with description of the characteristics of the selected studies; 4 - critical analysis of studies, carried out based on the definition of the level of evidence; 5 - interpretation of results and 6 - presentation of the review.
Research question
The definition of the study's guiding question was formulated, using the PICOT strategy, an acronym for Patient, Intervention, Comparison, Outcomes (outcome) and Type of study, in which: “P” – black and indigenous women of reproductive age with COVID- 19; “I” – hospitalization, hospitalization in ICU and need for ventilatory support; “C” - comparison between women of reproductive age with different skin colors; “O” - outcomes: cure or death associated with COVID-19 in black and indigenous women of reproductive age; and "T" - type of study: epidemiological, observational, cross-sectional studies, prospective and/or retrospective cohort, series and/or case reports. Thus asking: What is the production of scientific knowledge available in the national and international literature of epidemiological studies on the mortality of black and indigenous women of reproductive age with COVID-19 when compared to women of other skin colors?
Inclusion and exclusion criteria
The following inclusion criteria were established: primary studies epidemiological, observational, cross-sectional, prospective and retrospective cohort studies,series and/or case reports published from December 2019 onwards, which addressed articles that answered the study question; available in full electronically; in English or Portuguese. The time frame was established to ensure an adequate number of primary studies, since the inclusion of a high volume of research could make conducting the RIL unfeasible or introduce biases in the following stages of the study, in addition to considering the emergence of the coronavirus in China in December 2019 and to increase the credibility of the results, updated references were used. The exclusion criteria were: letters, editorials, experience reports, reviews, studies that did not fit the theme, study population and objectives that were not relevantto the proposal of this research.
Search strategy
The literature searches took place in May 2024 in the following information sources: Elsevier Scientific Publications (EMBASE), Latin American and Caribbean Literature in Health Sciences (LILACS), on the Medical Literature Analysis and Retrievel System Online (MEDLINE) portal via National Library of Medicine (PUBMED), SciVerse Scopus (SCOPUS), ScienceDirect and Web of Science. The search in the selected databases/portal was carried out with the descriptors selected individually using the Boolean operator AND and OR, using terms indexed in the structured vocabulary of the Health Sciences Descriptors (DeCS) of the Virtual Health Library (VHL) and Medical Subject Headings (MeSH terms).
Study selection
After searching each database, the studies were managed in the Rayyan®[18] web application and studies that met the inclusion criteria were selected. The selection of studies was carried out in three stages: screening of titles and abstracts, by two independent reviewers. Articles that did not meet the inclusion criteria were excluded at this stage; full reading: the articles selected in the previous stage were read in full by two independent reviewers and discrepancies in the inclusion of articles were resolved by a third reviewer.
Data extraction and analysis
The assessment of the methodological quality of the studies was carried out using the level of evidence, taking into account Melnyk & Fineout-Overholt (2005). 1A: Systematic Review (with homogeneity) of Randomized Controlled Clinical Trials (RCT); 1B: RCT with Narrow Confidence Interval; 1C: “all or nothing” Therapeutic Results, 2A: Systematic Review (with homogeneity) of Cohort Studies; 2B: Cohort Study (including lower quality RCT); 2C: Observation of Therapeutic Results (outcomes research) and/or Ecological Study, 3A: Systematic Review (with homogeneity) of Case-Control Studies; 3B: Case-Control Studies, 4: Case Report (including lower quality Cohort or Case-Control) and 5: Expert Opinion without critical evaluation or based on basic materials (physiological study or study with animals)[19].
For data processing and analysis, the software IRAMUTEQ® (Interface de R pour les Analyzes Multidimensionnelles de Textes et de Questionnaires) [20] was used, which is anchored in the R software and allows various statistical analyzes on the textual corpus. The software identifies and formats initial context units that become elementary context units. In the software, vocabulary research is carried out, and words are reduced, based on their roots (lemmatization), with the dictionary created from the reduced forms, and active and supplementary forms identified, enabling different types of analysis, such as Descending Hierarchical Classification, similarity analysis and word cloud [20-22]. The results were presented and discussed with dialogue between the study authors (figure 2-8).
Presentation of the summary of results
The extracted data were presented descriptively and summarized in tables. Data from the studies were collected, containing the following information: study, year of publication, language, country, objectives, methodological characteristics (study design) and main results. Data analysis was carried out qualitatively, seeking to identify recurring patterns and themes in the included studies.

Figure 1- Flowchart for search, selection and inclusion of studies adapted from PRISMA
| Title | Year of publication, language and country | Type of study and level of evidence | Objective | Results |
| Maternal mortality and COVID-19: A nationwide ecological analysis from Ecuador23 | 2024 English Ecuador | Cross-sectional study | Systematically evaluate the epidemiological characteristics of COVID-19 in pregnant women, evaluate related maternal mortalities, verify the case fatality rate, and outline associated risk factors | 3,274 cases of COVID-19 have been identified, with 22 deaths. The majority of cases were of mixed ethnicity, however, the highest fatality rate was observed among indigenous people, those aged between 40 and 44 years old and those with a history of comorbidities |
| Tracking excess of maternal deaths associated with COVID-19 in Brazil: a nationwide analysis24 | 2023 English Brazil | Cross-sectional study | Estimate maternal deaths in Brazil caused directly and indirectly by COVID-19 in 2020 | The chances of being a black woman, living in a rural area and being hospitalized outside the municipality of residence among maternal deaths were higher |
| Anti-black racism and maternal death from COVID-19: what did we see in the Pandemic?25 | 2023 Portuguese Brazil | Cross-sectional study | Present racism and its manifestations in maternal death from COVID-19 | The results show how racism affects black and brown pregnant and postpartum women, who have a higher mortality rate due to COVID-19 compared to white women, particularly in the postpartum period. The chance of maternal death in the postpartum period for black women was 62% higher compared to white women |
| Racial and Ethnic Disparities in Postpartum Care in the Greater Boston Area During the COVID-19 Pandemic26 | 2022 English United States of America | Retrospective cohort study | Examine whether the COVID-19 pandemic is associated with an increase in existing racial and ethnic disparities in access to postpartum care | Participants were racially and ethnically diverse, Asian, Black, White Hispanic, and other race or ethnicity women; access to postpartum care recovered more slowly among Black and Hispanic women than among White women |
| Clinical characteristics and risk factors for maternal deaths due to COVID-19 in Brazil: a nationwide population-based cohort study27 | 2022 English United States of America | Cohort study | Monitor the characteristics and factors associated with death among pregnant and postpartum women with coronavirus disease | Black people had a higher risk of death than women who self-identified as white. Women in the North, Northeast, Central-West and Southeast regions had a higher risk of death than women in the South region |
| Progression of COVID-19 Among Black Pregnant Women: Population-Based Study28 | 2022 English Brazil | Cross-sectional study | To evaluate the evolution of COVID-19 related to skin color among Brazilian pregnant women registered in the Influenza Surveillance Information System (SIVEP Gripe) | The study identified that there was a drop of approximately two thirds in the proportion of pregnant women who required ICU care or died, when comparing the first and second periods. In the second period, black pregnant women had approximately five times greater risk of death compared to white and mixed-race women. |
| Effect of the COVID-19 pandemic on Social Determinants of Health in Non-Hispanic Black pregnant women29 | 2022 English United States of America | Retrospective cohort study | Examining the difference in social determinants of health for non-Hispanic Black pregnant women during the COVID-19 pandemic compared to pre-pandemic | Non-Hispanic Black women during the pandemic had more job opportunities and more prenatal care than before the pandemic, but they experienced more racial discrimination and felt less safe in their neighborhoods |
| Higher severe acute respiratory syndrome coronavirus 2 infection rate in pregnant patients30 | 2021 English United States of America | Cross-sectional study | Estimate the rate of coronavirus infection in pregnancy and examine disparities by race, ethnicity, and English language proficiency in Washington State | The proportion of pregnant patients in nonwhite racial and ethnic groups with severe acute respiratory syndrome coronavirus disease 2 infection was 2 to 4 times greater than the racial and ethnic distribution of women in Washington state who gave birth live in 2019 |
| Structural racism and risk of SARS-CoV-2 in pregnancy31 | 2021 English United States of America | Retrospective cohort study | Compare Black and Non-Black Pregnant Women Infected with SARS-CoV-2 to Understand How the Distribution of Risk Factors May Differ by Race | Black women were younger and more likely to identify an occupational contact as exposing them to SARS-CoV-2. Most women were more likely to have a premature birth |
| Disproportionate Impact of Coronavirus Disease 2019 (COVID-19) Among Pregnant and Postpartum Black Women in Brazil Through Structural Racism Lens32 | 2020 English Brazil | Cross-sectional study | Monitor SARS-CoV-2 related maternal deaths in the country | Maternal mortality in black women due to COVID-19 was almost 2 times higher than that observed in white women |
| Risk factors for adverse outcomes among pregnant and postpartum women with acute respiratory distress syndrome due to COVID-19 in Brazil33 | 2020 English Brazil | Cross-sectional study | To evaluate whether clinical and social risk factors are associated with negative outcomes for COVID-19 disease among Brazilian pregnant and postpartum women | The analysis showed that the postpartum period, age over 35 years, obesity, diabetes, black ethnicity, living in a peri-urban area, not having access to the Family Health Strategy or living more than 100 km from the reporting hospital were associated with an increased risk of adverse outcomes |
| The tragedy of COVID-19 in Brazil: 124 maternal deaths and counting34 | 2020 English Brazil | Cross-sectional study | To describe outcomes for pregnant and postpartum women with COVID-19 disease from the first documented case in Brazil on February 26, 2020 until June 18, 2020 | It was diagnosed in 978 pregnant and postpartum women in Brazil during the study period, the study found 124 deaths of pregnant or postpartum women. Of the 978 positive cases, 207 (21.2%) were admitted to the ICU (134 recovered cases and 73 fatal cases). It is worth mentioning that 22.6% of women who died were not admitted to the ICU, and only 64.0% had invasive ventilation. |
| Racial and ethnic disparities in severity of COVID-19 disease in pregnancy in the United States35 | 2020 English United States of America | Epidemiological study | Review cases of women in an obstetric clinic diagnosed with COVID-19 | Black women had chronic lung disease, diabetes, hypertension, or obesity, which may have contributed to their increased vulnerability to COVID-19 |
| Coronavirus disease 2019 pregnancy outcomes in a racially and ethnically diverse population36 | 2020 English | Case series study | Describe the clinical course of coronavirus disease 2019, the effect of comorbidities on disease severity, laboratory trends, and pregnancy outcomes of symptomatic and asymptomatic pregnant women | Hispanic women were overrepresented in the coronavirus-positive group. Additionally, Hispanic ethnicity was associated with a higher rate of moderate and severe illness than non-Hispanic ethnicity. |
| Characteristics and outcomes of pregnant women admitted to hospital with confirmed SARS-CoV-2 infection in UK: national population based cohort study37 | 2020 English United Kingdom | Prospective cohort study | To describe pregnant women admitted to hospital with coronavirus infection in the United Kingdom | Pregnant women admitted to the hospital were black, overweight, aged 35 or over and had pre-existing comorbidities |
Source: Prepared by the authors. 2024
Table 1: Synthesis of knowledge of the studies included in the review
The graph below is a representation of Zipf's Law, used in word frequency analyzes in texts. In the Zipf chart, the frequency of a word (Y-axis) is plotted as a function of its ranking (X-axis) on a logarithmic scale. The most frequent word is in first place, the second most frequent in second place, and so on; the Y axis represents the frequency of occurrence of each word in the analyzed corpus; the logarithmic scale is typical in Zipf graphs, as it makes
it easier to visualize the distribution of word frequencies; and each red dot on the graph represents a word from the analyzed corpus, with its frequency plotted against its ranking. The graph shows a sharp drop in frequency as the ranking increases, which is expected in a Zipf graph. The linearity of the graph on a logarithmic scale suggests that the distribution of word frequencies follows Zipf's Law (figure 2).

Source: Prepared by the IRAMUTEQ® software (R Interface for Multidimensional Analysis of Texts and Questionnaires. 2024.
Figure 2: Word frequency by representation of Zipf's Law
Using the software, a word cloud was generated where the frequency of words in the text corpus is visualized, where the size of each word is proportional to its frequency in the analyzed text. Highlighted words: "woman" is the most highlighted word and, therefore, the most frequent in the analyzed corpus. Words related to maternal mortality and COVID-19: "covid," "pandemic," "respiratory," "syndrome," "infection," "intensive,"
"ventilation," and "diagnose" indicate the presence of discussions about respiratory complications and the severity of COVID-19 infection. Social and demographic aspects: "black," "Hispanic," "white," "ethnic," "race," "racial," and "minority" suggest that the study addresses racial and ethnic disparities in maternal mortality associated with COVID-19. "Age," "group," and "factor" can indicate analysis of different demographic groups. (figure 3).

Figure 3: Maternal mortality and COVID-19 word cloud
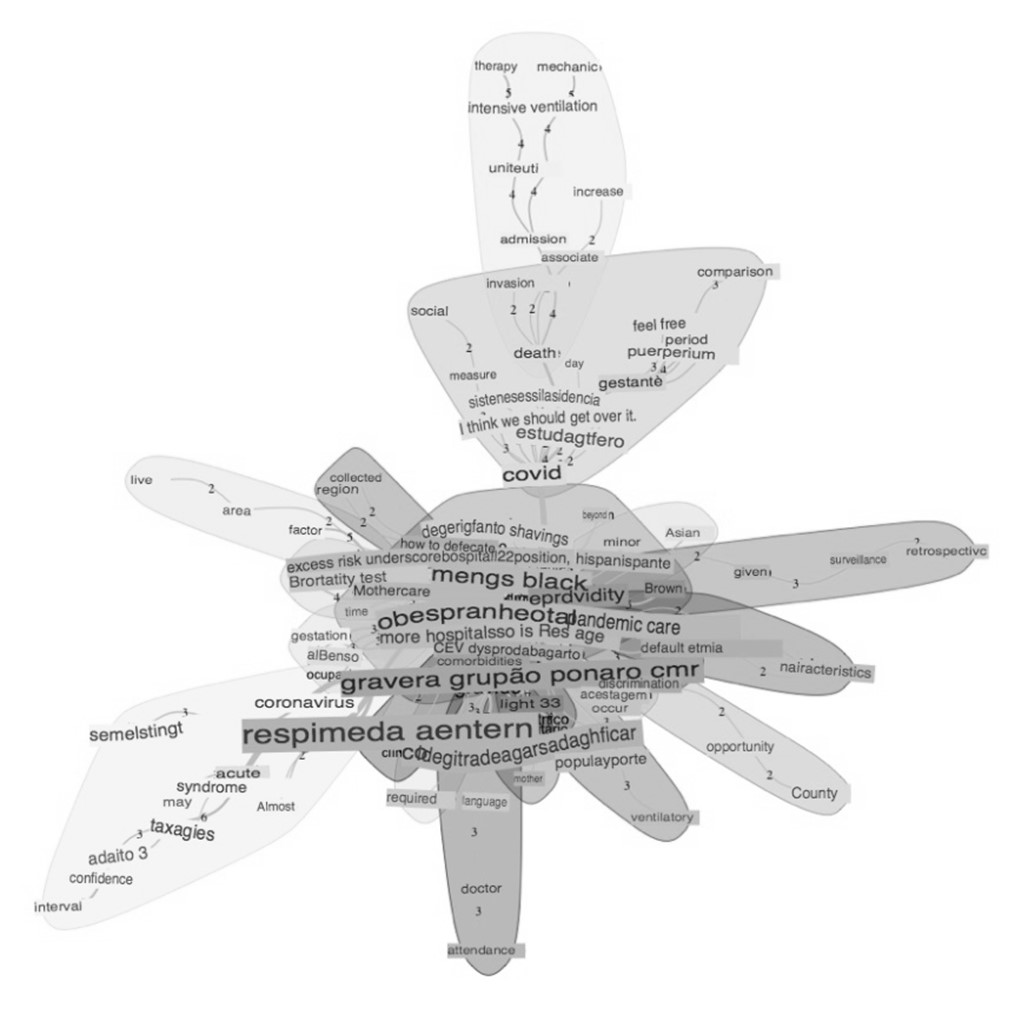
The dendrogram generated by IRAMUTEQ® visualizes the co-occurrence and semantic proximity between different terms in the textual corpus. The words were grouped into clusters, which are highlighted by different colors and shaded areas. Yellow Cluster: includes terms such as "death," "admission," "uti," "therapy," "intensive," and "ventilation," suggesting a focus on severe cases of COVID-19 that require intensive care and are associated with mortality. Orange Cluster: Contains terms such as "pregnant," "period," "symptom," and "postpartum," which appear to be related to conditions and symptoms during and after pregnancy. Green
Cluster: Includes terms such as "coronavirus," "respiratory," "syndrome," and "acute," indicating a focus on respiratory complications associated with COVID-19. Pink Cluster: includes terms such as "pandemic," "ethnic," "discrimination," and "racial," which point to the discussion of racial and ethnic inequalities in health during the pandemic. Blue Cluster: Includes terms such as "ventilatory," "necessary," "given," and "county," suggesting discussions about the need for mechanical ventilation and regional data. Red Cluster: includes many central terms such as "woman," "serious," "childbirth," "black," "covid," and "hospitalization," which appear to be the core of the discussions and are connected to several other clusters (figure 4).
Source: Prepared by the IRAMUTEQ® software (R Interface for Multidimensional Analysis of Texts and Questionnaires. 2024.
Figure 4: Dendrogram of occurrence and semantic proximity between textual corpus terms
The terms within each cluster are semantically related, indicating that they frequently appear together in the analyzed texts. The proximity between the clusters suggests that there are thematic overlaps and that some themes are interrelated. The central theme appears to be "women" and "maternal mortality" associated with "COVID-19," with terms related to disease severity, hospitalization, and intensive care. Other important topics include respiratory complications, racial and ethnic inequalities, and specific care during pregnancy and postpartum. This dendrogram provides a structured overview of the main themes and subthemes covered in your text corpus on maternal mortality associated with COVID-19.
Regarding the classification of a textual corpus into different classes based on similarity analysis and word frequency, each class is represented by a different color and a percentage that indicates the proportion of the corpus that belongs to that class. In this study, class 1 (18.8%) represents the largest proportion of the corpus. Most frequent words: "admission," "state," "death," "union," "hospitalization," "ventilation." serious complications from
COVID-19 leading to hospital admission and the need for ventilation, possibly ending in death; class 6 (17.4%) most frequent words: "ethnic," "black," "pandemic," "disparity," "racial," "population." racial and ethnic disparities during the pandemic, especially focusing on the black population; class 4 (17.4%) most frequent words: “pregnant,” “pregnancy,” “postpartum,” “care,” “complication.” aspects related to pregnancy, postpartum care and associated complications; class 5 (15.9%) most frequent words: "respiratory," "syndrome," "acute," "coronavirus," "ventilation." class 2 (14.5%) most frequent words: "system," "social," "measure," "access," "social and systemic aspects, measures of access to health and social conditions; most frequent words: "hospital," "hospitalization," "doctor," "care," "hospitalization," medical care and treatment. The dendrogram below (figure 5) offers a clear view of how the textual corpus was segmented into distinct themes, which can help in structuring your data analysis and identifying specific areas of focus in the study of mortality associated with COVID-19.

Source: Prepared by the IRAMUTEQ® software (R Interface for Multidimensional Analysis of Texts and Questionnaires. 2024.
Figure 5: Dendrogram in classes segmented into distinct themes
The analysis of the articles included in this review reveals important information about the mortality of black and indigenous women of reproductive age associated with COVID-19 infection. The RIL on maternal mortality due to COVID-19 in black and indigenous women also signals a worrying panorama of inequality and exacerbated vulnerability driven by the pandemic.
Maternal mortality among black and indigenous women when associated with the COVID-19 pandemic demonstrates a consistent pattern of vulnerability. Thus, in Ecuador, it was identified that indigenous women had the highest mortality rate among pregnant women infected with COVID-19, highlighting the intersection between ethnicity and risk of maternal death in this vulnerable population [23].
A study shows that black pregnant women were more likely to develop serious complications, such as the need for mechanical ventilation and intensive care, due to vulnerabilities intensified by factors such as structural racism and economic inequalities [12,30]. The lack of adequate healthcare infrastructure in indigenous areas, along with cultural and language barriers, has contributed to lower quality and accessibility of healthcare, worsening negative outcomes in these populations.
The intersection between skin color, ethnicity and socioeconomic factors is crucial to understanding the disparities in COVID-19 lethality among black and indigenous women [25,26,28,31,32,38]. The disproportionate impact on these populations is the result of a series of social, economic and structural factors that place these women in a position of high risk in relation to maternal mortality. Study reports that black women face a greater likelihood of severe complications, such as respiratory failure, compared to women of other races, which has been attributed to disparities in access to healthcare and pre-existing health conditions, often worsened by factors adverse socioeconomic conditions [12,28,30,32,33].
Indigenous women have also experienced elevated rates of maternal mortality during the COVID-19 pandemic, with factors such as geographic location, which limits access to quality health services, and the historical marginalization of these populations, contributing to increased risk [38].
The presence of comorbidities, such as hypertension and diabetes, were also relevant factors found in this review, given their prevalence, they were concentrated among black and indigenous women due to social determinants of health, such as chronic stress associated with racism and poverty [24,27,28,29,31,32]. These conditions increase the vulnerability of these women to COVID-19, exacerbating the risk of maternal Mortality [39,40]
Furthermore, lack of access to quality prenatal and obstetric care is a critical factor contributing to high maternal mortality from COVID-19 [24,32,33,34]. The disruption of healthcare services during the pandemic, combined with a reluctance to seek care for fear of infection, has further aggravated the situation. The literature indicates that women from these populations had less access to adequate prenatal care and often received less guidance about the risks and preventive measures necessary during pregnancy in times of pandemic [24,27,28,29,31,32].
Inequality in the distribution of health resources, such as ventilators and ICU beds, was also highlighted as a reason that contributed to the higher mortality among black and indigenous women. In many regions, these populations live in areas with less hospital infrastructure, which limits access to critical care needed to treat serious complications from COVID-19 [28,32,33].
In Brazil, the situation is similar, where black women face a significantly higher risk of death from COVID-19 compared to white women. Studies highlight that factors such o living in rural areas and being hospitalized outside the municipality of residence increase the chances of maternal Death [24]. In the United States, the racial disparity in maternal mortality from COVID-19 is also evident, with black women presenting a higher risk of serious complications and death during pregnancy and the postpartum period. The pandemic has further accentuated pre-existing inequalities in access to healthcare, with black and Hispanic women facing greater difficulty in receiving adequate postpartum care [29,37].
Furthermore, analysis of maternal mortality in Brazil and the United States indicates that pre-existing comorbidities, such as obesity, diabetes and hypertension, are more prevalent among black women, contributing to the greater severity of COVID-19 and increasing the risk of Death [27]. Studies also indicate that the inadequate response of the health system, combined with racial discrimination, results in higher maternal mortality from COVID-19 among black women. In Brazil, mortality among black women was almost twice as high as that observed among white women, highlighting the urgent need for public policies that address these disparities [25,32].
Black and indigenous women of reproductive age had significantly higher rates of serious complications and mortality associated with COVID-19. These inequalities reflect structural disparities in health, rooted in racism and barriers to access to care. Black and indigenous women have had less access to quality prenatal and obstetric care during the pandemic. This has resulted in less guidance and adequate preventive interventions to deal with infection during pregnancy [25,26,28,31,32,35].
The review suggests equitable allocation of health resources as a key way to ensure that all women, regardless of their race or ethnicity, have access to the care they need during public health emergencies. Finally, it highlights the urgent need for specific interventions and public policies that address structural inequalities that affect black and indigenous women. The COVID-19 pandemic has exposed and exacerbated existing disparities, and the review concludes that it is imperative to develop public health strategies that are culturally sensitive and that address the specific needs of these populations. Only through an equitable and inclusive approach will it be possible to reduce maternal mortality and ensure that all women have the opportunity to have a safe pregnancy and birth, even in times of global crisis.
This study highlights the severity of racial disparities in maternal mortality associated with COVID-19, particularly among Black and Indigenous women. The findings suggest that these inequalities are not merely a consequence of the pandemic, but reflect structural and historical issues of racism and discrimination that permeate access and quality of healthcare. The disproportionate impact of COVID-19 on these populations emphasizes the need for public policies aimed at racial equity in health, including improving access to quality health services, implementing strategies to mitigate structural racism, and promoting interventions focused on the specific needs of black and indigenous women. This study reinforces the urgency of integrated actions that address the roots of social and health inequalities, with the aim of reducing maternal mortality and ensuring safe and equitable care for all women, regardless of their skin color.
Postgraduate Program of the Department of Gynecology of the Escola Paulista de Medicina of the Universidade Federal de São Paulo, Facultad de Enfermería y Fisioterapia of the Universidad de Salamanca and Escuela Universitaria of the Enfermería Cruz Roja of the Universidad Autónoma de Madrid.
The authors have no conflicts of interest to declare
The authorsdeclare that therewas no funding for the study
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
