
Research Article | DOI: https://doi.org/10.31579/2641-0419/213
*Corresponding Author: Ranjit Sharma, Nepal Medi citi hospital, 44700 Bhaisepati, Lalitpur, Nepal.
Citation: Ranjit Sharma, Anish Hirachan, Milan Gautam. (2021) Morphology of Coronary Artery Disease in a Patient with, Psoriasis Presenting with an Acute Coronary Syndrome. J. Clinical Cardiology and Cardiovascular Interventions, 4(15); Doi:10.31579/2641-0419/213
Copyright: © 2021 Ranjit Sharma, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 03 August 2021 | Accepted: 01 September 2021 | Published: 10 September 2021
Keywords: coronary artery disease; acute coronary syndrome
Background: This study was designed to evaluate the patterns of coronary artery disease in patients with Psoriasis presenting with acute coronary syndrome (ACS).
Methods: This was a prospective, observational study, conducted on 28 patients with Psoriasis, presenting with acute coronary syndrome undergoing coronary angiogram from September 2017 to March 2021. All patients had undergone coronary angiogram; severity and morphology of coronary lesion were analyzed. Echocardiography was used to analyze LV wall motion and LV function.
Results: The study showed that of 28 patients with Psoriasis who presented with ACS, 45.8% of patients were presented with NSTEMI, 39.2% % STEMI, and Unstable angina 15%. The average time of presentation after the onset of the symptom was 14.8 hours. 66 % of patients were a smoker. Coronary involvement 50% had TVD, 40% DVD, and 10% had SVD. In 77.6% culprit vessel was LAD, 10.4% LCX, and 12% RCA. In 75% of patient's coronary lesion was located in the proximal LAD. Chronic total occlusion was found in almost 26% of patients. Extensive LV wall motion abnormality with severe LV systolic dysfunction was noted in Psoriasis patients at the time of presentation (mean LVEF=28%).
Conclusions: Psoriasis patients presenting with ACS, associated with increased severity of coronary lesions, multivessel involvement, and depressed LV systolic function.
An acute coronary syndrome (ACS) is the leading cause of death and disability worldwide [1]. World Health Organization data show that around 17.7 million cardiovascular disease deaths worldwide in 2015 (31% of all-cause mortality), of whom 7.4 million were due to coronary artery disease [2].
Psoriasis is a chronic autoimmune, relapsing inflammatory disease of the skin affecting 2% to 3%, the global adult population [3]. Psoriasis can occur at any age, but the onset is usually between the ages of 18 and 35 years. A bimodal onset has been suggested with an initial peak at ages 16 to 22 years and a second peak at age 57 to 60 years [4]. The prevalence of psoriasis varies according to geographical location, with higher rates among Caucasians when compared with other ethnicities [5]. It is also argued that countries located away from the equator have shown a higher prevalence of the disease when compared to warmer climates where the reported cases are relatively lower [6]. The most common type of psoriasis, accounting for 90% of cases, is psoriasis Vulgaris, which is characterized by the presence of papulosquamous plaques of various sizes and numbers [7]. The plaque severity and degree of affected body surface area vary throughout an individual’s life [8].
The life expectancy of people with psoriasis was reported to be nearly 5 years lower compared to control groups, with cardiovascular problems being the main cause of death [9]. Understanding why psoriasis is a risk factor for atherosclerosis requires a basic understanding of their shared pathogenic features. [10] A meta-analysis conducted by Choudhary et al. demonstrated that 30.3% of patients with psoriasis had metabolic syndrome [11]. A strong link between high BMI and the development of both diseases has been explained in a robust systematic review which demonstrated that the incidence and prevalence of obesity are higher in patients with psoriasis and it is independently associated with CVD [12]. Smoking is a strongly recognized risk factor for CVD [13]. It has been demonstrated that patients who smoke more than 20 cigarettes per day are associated with a twofold risk of severe psoriasis [14]. Recent studies have found a higher prevalence of metabolic syndrome (17.8%, p=0.021), CVD (4.6%, p=0.044), hypertension (32.5%, p=0.000), and hyperlipidemia (22.3%, p=0.025) in patients with psoriasis, as compared with that of the controls [15]. Seventy-three (37%) patients with psoriasis had LDL levels higher than the target LDL level proposed by the ATP III guideline [15].
Atherosclerosis is a lipid-related chronic inflammatory disease in which immune mechanisms play a pivotal role [16]. The lesions are filled with large numbers of immune cells. Similarly, Psoriasis is characterized by chronic autoimmune, relapsing inflammatory disease of the skin [17]. At the cellular level, atherosclerosis is associated with inflammatory cytokines, such as TNF-α and IL-1, which overlap with the same markers implicated in psoriasis [18].
T-helper 1 cells of the adaptive cellular immune system are integral in plaque development and inflammation propagation for both psoriasis and atherosclerosis [19]. The activated T-helper 1 cells release proinflammatory cytokines, including interferon-g, tumor necrosis factor-a, and interleukin-2 (20). This leads to the activation of macrophages, keratinocytes, and vascular cells, all of which release additional cytokines [21]. In addition to the role of T-helper 1 cells, proinflammatory effects of T-helper 17 cells and anti-inflammatory effects of T regulatory cells contribute to both pathologies. T-regulatory cells modulate the inflammatory process by secreting anti-inflammatory cytokines, such as interleukin-10 and transforming growth factor-b. Both psoriasis and atherosclerosis have reduced numbers and activity of T-regulatory cells and resultant hyperactivity of T-helper 1/T-helper 17 cells. Therefore, psoriasis and atherosclerosis result in plaques in the skin and arteries, respectively that are a focus of both local and systemic immune activity [22, 23].
Chronic exposure to systemic inflammation in patients with severe psoriasis can result in coronary microvascular dysfunction (CMD). This may lead to the impairment of the coronary arteries’ ability to augment coronary blood flow (vasodilator abnormality) and/or in a reduction in coronary blood flow (coronary microvascular spasm) [24]. High levels of angiotensin-converting enzyme levels, renin, and ET-1 in psoriasis are associated with an increased risk of hypertension [25]. It is believed that the adipose tissue in psoriatic patients acts as a source of angiotensinogen that is converted to angiotensin II [26].
Some of the systemic medications have side effects that increase cardiovascular risk. Cyclosporine can worsen arterial hypertension, although it infrequently causes new-onset hypertension during short-course, intermittent therapy [27]. Cyclosporine also can alter lipid metabolism, resulting in hyperlipidemia [28]. Systemic retinoids have been shown to increase serum triglycerides and decrease serum high-density lipoprotein cholesterol and insulin sensitivity [29]. Methotrexate is capable of increased homocysteine levels that could tip the hemostasis balance to a prothrombotic state [30]. Cardiovascular medications may affect psoriasis. Statins, traditionally used for the treatment of hyperlipidemia and atherosclerotic disease, also have anti-inflammatory effects that could provide potential benefits in psoriasis [31]. Beta-blockers have been suggested to both induce and exacerbate psoriasis [32]. Selective beta-blockers, including metoprolol and atenolol, also have been reported in association with psoriasiform eruptions [33, 34]. Angiotensin-converting enzyme inhibitors have been reported to have a possible association with psoriasis. Psoriasis and psoriasiform eruptions also have been reported with angiotensin II antagonists, calcium channel blockers, and clonidine [35, 36, and 37]. Steroids have an effective role in the treatment of psoriasis but they are implicated in heart diseases. They can potentially cause hypertension by various mechanisms which include increased systemic vascular resistance, extracellular volume, and cardiac contractility. They also cause sodium retention, hypokalemia, and hypertension by altering the blood pressure regulatory system [38]

It is a retrospective, single-center study, performed at Nepal Mediciti Hospital, Nepal. A total of 28 Psoriasis patients who presented with acute coronary syndrome from September 2017 to March 2021 were enrolled in this study. In all 28 patients with Psoriasis, presenting an acute coronary syndrome left ventricular systolic function, and left ventricle wall motion analysis was done before coronary catheterization. All patients were taken to the catheterization lab for a coronary angiogram. Severity and morphology of coronary lesion were analyzed
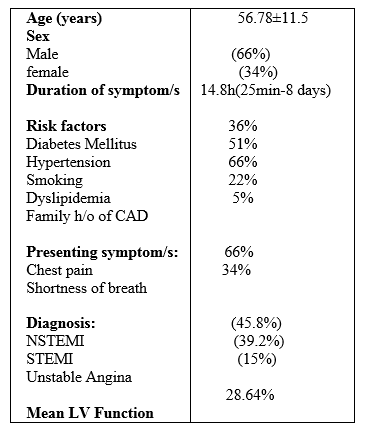
A total of 28 Psoriasis patients presenting with the acute coronary syndrome were included in the study. The average age was 56.78 ± 11.5 with the youngest being 26 years and the oldest being 72 years old. Most of the patients were male 66%. The average time of presentation after the onset of the symptom was 14.8 hours.
The commonest symptom was chest pain 66% followed by shortness of breath in 34%. The diagnosis was made base on a clinical symptom, electrocardiography findings, and cardiac biomarkers. Most of the patients 45.8% were presented with NSTMI followed by 39.2% STEMI and 15% unstable angina. Among the risk factors, smoking was the commonest and found in 66% of patients followed by hypertension 51% and diabetic 36%. Coronary involvement 50% had TVD, 40% DVD, and 10% had SVD. In 77.6% culprit vessel was LAD, 10.4% LCX, and 12% RCA. In 75% of patient's coronary lesion was located in the proximal LAD. Chronic total occlusion (CTO) was found in almost 26% of patients. Extensive LV wall motion abnormality with severe LV systolic dysfunction was noted in Psoriasis patients (mean LVEF=28.64%).
Recent evidence has suggested that psoriasis is associated with systemic inflammation and an increased risk for developing cardiovascular disease. This has led to the concept that systemic inflammation from psoriasis may predispose to atherosclerotic initiation and progression. Recent studies have found a higher prevalence of metabolic syndrome (17.8%, p=0.021), CVD (4.6%, p=0.044), hypertension (32.5%, p=0.000), and hyperlipidemia (22.3%, p=0.025) in patients with psoriasis, as compared with that of the controls. Seventy-three (37%) patients with psoriasis had LDL levels higher than the target LDL level proposed by the ATP III guideline. Similar findings were found in our study and showed that hypertension was found in 51%, dyslipidemia in 22%, and diabetes mellitus in 36%.
Several studies have shown a strong association between psoriasis and angiographic coronary artery disease. Similar findings were found in our study and showed that 50% had TVD, 40% DVD, and 10% had SVD. In 77.6% culprit's vessel was LAD, 10.4% LCX, and 12% RCA. In 75% of patient's coronary lesion was located in the proximal LAD. Chronic total occlusion was found in almost 26% of patients. Extensive LV wall motion abnormality with severe LV systolic dysfunction was noted in Psoriasis patients at the time of presentation (mean LVEF=28%).
Psoriasis has a bimodal distribution of incidence, with a first peak in patients between 20 to 30 years old and a second peak in patients 50 to 60 years of age. Because this second peak coincides with the age range that patients are also more likely to develop overt CAD. . In our study the average age was 56.78 ± 11.5 with the youngest being 26 years and the oldest being 72 years old.


There are several limitations of this study. First, it is a single-center retrospective study. Second, coronary angiographic scoring was based on visual estimation at the time of cardiac catheterization. Third, IVUS and OCT were not used to interrogate the coronary lesion.
Psoriasis patients presenting with ACS, associated with increased severity of coronary lesions, multivessel involvement, and depressed LV systolic function. Various studies have explored the link between cardiovascular complications and psoriasis. But other avenues need to be explored and more in-depth research on a wider scale is required.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
