
Case Report | DOI: https://doi.org/10.31579/2690-1919/275
Pathology and Cytology Laboratory (CITADIAG SL). Plaza de San Leandro, esquina calle Alhóndiga 59. 41003. Sevilla. Spain.
*Corresponding Author: Francisco Javier Torres Gómez. Pathology and Cytology Laboratory (CITADIAG SL). Plaza de San Leandro, esquina calle Alhóndiga 59. 41003. Sevilla. Spain.
Citation: Francisco Javier Torres Gómez, Rosa Sánchez de Medina González, Beatriz Bravo Zambrano, Vanesa Ortega Bravo. (2022). Moluscum contagiosum on infundibular cyst. No more than a curiosity, J. Journal of Clinical Research and Reports, 12(1) DOI:10.31579/2690-1919/275.
Copyright: © 2022 Francisco Javier Torres Gómez. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 17 October 2022 | Accepted: 24 October 2022 | Published: 31 October 2022
Keywords: Infundibular Cyst; Molluscum contagiosum; Skin; Mixed cutaneous lesion; Incidental histologic features
The infundibular cyst is a skin lesion typically located on hairy areas that is extremely common. In fact, it is part of the daily routine of any pathology laboratory. Although both the dermatologist, the surgeon and the pathologist are sufficiently familiar with it and guide each case correctly, sometimes there are histological peculiarities that justify the histological study of the lesion. The coincidence of a molluscum contagiosum, a highly contagious entity in the context of an infundibular cyst, implies taking a series of precautions that would not be implemented based solely on clinical criteria.
The infundibular cyst is a skin lesion typically located on hairy areas that is extremely common. In fact, it is part of the daily routine of any pathology laboratory. Although both the dermatologist, the surgeon and the pathologist are sufficiently familiar with it and guide each case correctly, sometimes there are histological peculiarities that justify the histological study of the lesion. The coincidence of a molluscum contagiosum, a highly contagious entity in the context of an infundibular cyst, implies taking a series of precautions that would not be implemented based solely on clinical criteria.
A 22-year-old female patient who came to the clinic due to the appearance, at the level of the right arm, of a rapidly growing nummular lesion with no associated symptoms. The lesion had a soft consistency and was not umbilicated on the surface. Surgical excision was performed with the clinical diagnosis of epidermoid cyst. The histological study showed the presence, at the dermal level, of a cystic lesion lined by flat stratified epithelium without atypia, with the presence of a stratum granulosum and intense scaling at the luminal level. Multiple luminal keratin scales were combined with eosinophilic nodular formations with a ground glass appearance. Interpreting its presence as that of molluscum bodies, attention was paid to the complete lesion silhouette, identifying the pan-epithelial focal occupation by the same structures, allowing the diagnosis of molluscum contagiosum on infundibular cyst (Fig 1-5). There was only one lesion
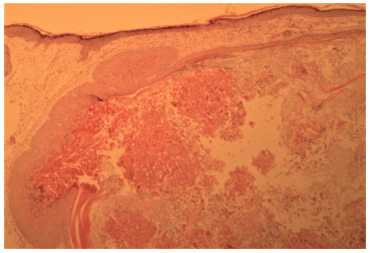
Figure1: Moluscum contagiosum on infundibular cyst. There can be seen multiple molluscum bodies are seen at the epithelial and luminal levels. HE 40X.
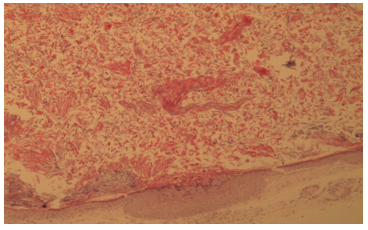
Figure 2: Moluscum contagiosum on infundibular cyst. Multiple molluscum bodies are born from the epithelial line and are mixed with keratin scales at the luminal level. HE 100X.
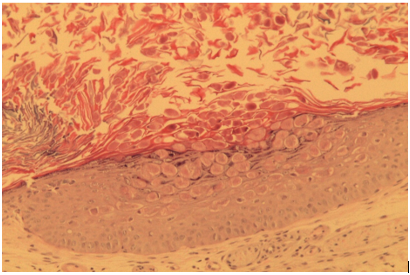
Figure 3: Moluscum contagiosum on infundibular cyst. There can be seen multiple molluscum bodies are seen at the epithelial and luminal levels. Detail. HE 200X.
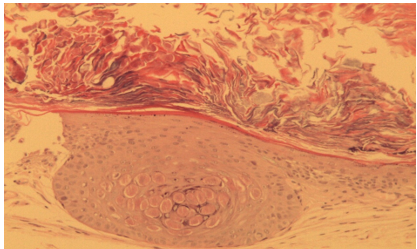
Figure 4: Moluscum contagiosum on infundibular cyst. There can be seen multiple molluscum bodies are seen at the epithelial and luminal levels. Detail. HE 200X.
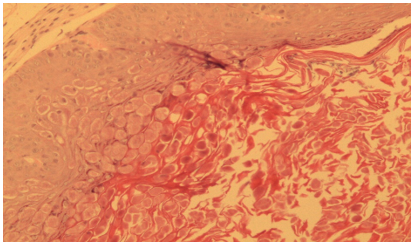
Figure 5: Moluscum contagiosum on infundibular cyst. There can be seen multiple molluscum bodies are seen at the epithelial and luminal levels. Detail. HE 400X.
The peculiar association of these two entities with an unequal incidence has been described in the literature. Most of the articles highlight the curiosity of the picture and provide characteristic images that even integrate publications with the format of “what is your diagnosis?” [1-3].
With this case we not only expand the international series but also reflect on various issues:
Most of the cases that describe this lesional association allude to a location in the head and neck, while our case was located in the arm.
There are studies that even introduce the precaution of not falling into clinical diagnostic confusion [5], although these are usually minor and do not have important prognostic implications, as in our case, which could well have been nothing more than an anecdote with a careless microscopic study. It is, therefore, one more anecdote of which dermatopathology is a rich discipline. We hope that the histological images are to the liking of the scientific community.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
