
Case Report | DOI: https://doi.org/10.31579/2690-4861/251
┬╣I st Surgery Clinic, ŌĆ£ Prof Dr Ion Chiricuta ŌĆØ Institute of Oncology
┬▓ŌĆ£Iuliu HatieganuŌĆØ University of Medicine and Pharmacy Cluj-Napoca, Romania
┬│II nd Surgery Clinic, Timisoara Emergency County Hospital, Romania
Ōü┤ŌĆØVictor BabesŌĆØ University of Medicine and Pharmacy Timisoara Romania
ŌüĄII nd Obstetric and Gynecology Clinic ŌĆ£Dominic StancaŌĆØ Cluj-Napoca, Romania
*Corresponding Author: Flaviu Ionut Faur, I st Surgery Clinic, ŌĆ£Prof Dr Ion ChiricutaŌĆØ Institute of Oncology Romania.
Citation: Flaviu I. Faur, Suciu P., Catalin F. P. Barbulescu, Clim A., Nati I., et. al (2022). Modified Martius Flap for repair of a postradiation Rectovaginal Fistula (RVF). A case report. International Journal of Clinical Case Reports and Reviews. 12(1); DOI:10.31579/2690-4861/251
Copyright: ┬® 2022 Flaviu Ionut Faur, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 29 August 2022 | Accepted: 05 September 2022 | Published: 17 October 2022
Keywords: rectovaginal fistula; mmartius flap; sars-cov2; ICG; sexual function; postradiation fistula
Introduction: A rectovaginal fistula (RVF) is an abnormal connection between the rectumŌĆÖs lower part and vaginaŌĆÖs posterior wall. It takes up approximately 6% of the overall anorectal fistulas, which are responsible for patientsŌĆÖ psychosocial collapse due to the incapacitating symptoms observed amongst the patients.
Case presentation: The study case presented was of a 33-year-old woman previously diagnosed with squamous carcinoma of the cervix FIGO IIIA (2017) treated through means of curative radiochemotherapy, utero-vaginal intracavitary brachytherapy (GammaMed plus iX 14 Gy/PTV-HR/ 2 weeks). In April 2021, she presented herself at the surgery unit claiming exclusion of fecal through the vagina and constant perineal pain. As a result of the clinical examination of the Milligan perineal area (vaginal touch, rectal touch), and presenting a positive Carey test (the methylene blue test ŌĆō positive, bubble air test ŌĆō positive), it was confirmed a recto-vaginal connection, positioned at around 3-4 cm from the EAS. This was followed by a loco-regional exploration through pelvic MRI scan which confirmed a lower recto-vaginal connection (fistula), situated at approximative 3 cm from the EAS, with a diameter of 8 mm (Rothenberger I).
Conclusions: There are a lot of metrics in the specialized literature that emphasize the versatility and feasibility of the Martius/mMartius procedure regarding the resolution of the RVF located in the lower, respectively median sphere. This metrics are also sustained by the anatomic flexibility of the perineal area regarding the loco-regional vasculature. An important aspect of this procedure is also related to the RVFŌĆÖs etiology, and that is because the local surgical intervention needs to be performed in minimum inflammatory circumstances, when the tissues do not present any tumoral impregnation.
A rectovaginal fistula (RVF) is an abnormal connection between the rectumŌĆÖs lower part and vaginaŌĆÖs posterior wall. It takes up approximately 6% of the overall anorectal fistulas, which are responsible for patientsŌĆÖ psychosocial collapse due to the incapacitating symptoms observed amongst the patients [1-2]. Moreover, RVF can also lead to recurring infections at the vagina or the lower urinary tract level.┬Ā
Approximately 88% of the RVFs are caused by obstetrical traumas caused, on their end, by a damage at the rectovaginal septum level. Besides the obstetrical traumas, RVFs can also appear as a result of: an intervention performed at the colorectal level, or even during a surgical procedure at the pelvic level (up to 10% of the proctectomy cases are particularly associated with the use of surgical staples, with neoadjuvant and adjuvant chemotherapy), the irradiation process which can cause a phenomenon of obliterating endarteritis along with the devascularization of the perineal region, neoplasia (for instance rectal, vaginal and bladder carcinoma which can cause a direct invasion) and local inflammatory processes: diverticulitis, chronic intestinal inflammatory disease┬Ā[3-5]. The traumas on the perineal region can also result in RVF.
┬ĀPostradic rectovaginal fistulaŌĆÖ frequency is approximately between 6%-10% with the most frequent appearance in the case of endometrial, cervical, and vaginal cancer, and a very important criteria to emphasizes in regards with its etiology is the fact that RVF is dependent on the level of irradiation [7]. The diagnosis of the postradic RVF usually happens during the first 2 years since the beginning of therapy however, during the same period, tardive fistula can also be diagnosed. When dealing with RVF one important thing to take into consideration is the exclusion of the local recurrences through the marginal biopsy process at the fistulaŌĆÖs hole [8]. Fecal diversion is a primordial therapeutic stage which has a high and important impact on minimizing the symptoms [9-10].
Rectovaginal fistula types were classified by Rothenberger into simple and complex as it follows:
Whereas the diagnosis can be easily confirmed by distal examination of the rectum, the treatment, especially of the recurring fistula, could be a very complex one. A small dimension fistula could even be asymptomatic, but on the other hand, the RVF evolution is manifested through severe clinical phases such as: defecation and eliminating gases through the vagina, tenesmus, rectorrhagia, diarrhea, pollakiuria, abdominal pain, lower back pain or an anorectal burning feeling.
The fistulaŌĆÖs anatomical situs needs to be identified in a brief way by emphasizing its direction, length, diameter, and path, and this is because some elements such as fistula diameter represents an important aspect in choosing the surgical procedure. Rectoscopy, sigmoidoscopy or the anorectal examination along with the identification of the fistula holes are simple and frequently chosen methods for the diagnosis process. The radiological examination regarding the rectovaginal fistula includes procedures such as: vaginogram, fistulogram and the barium meal. The inherited technics for the diagnosis of the rectovaginal fistulas as described by Carey and respectively Lockhart-Mummery are still highly used. Also, Shieh and Gennaro have reported a percentage of 9% for the diagnosis of the rectovaginal fistulas using the Carey technique [15].
PatientŌĆÖs medical history, together with a clinical examination which included proctoscopy and vaginal examination, are influencing in approximately 90% of the cases to setting a RVF diagnosis.
In case the diagnosis is still unclear, the next step is to conduct more imagistic examinations such as: nuclear magnetic resonance (NMR), computed tomography (CT) with contrast material, endoscopic ultrasound (EUS). NMR and EUS have the highest rate of diagnosis, both offering the possibility to examinate, at the same time, other potential injuries at the sphincter level [16-17]. The CT with contrast material is the second most used procedure, this examination being very precise in diagnosing abscessŌĆÖ formations or any malign tumors which represent RVF comorbidities. The biggest advantage of EUS procedure is its high availability and the fact that it also offers the possibility to evaluate potential injuries at the sphincter level, which are very important in the process of choosing the correct surgical procedure [18]. The manometry study at the sphincter level can be regarded as an important criterion in the way the rectovaginal fistulas are treated [19]. The intestinal clearance and the minimalization of the gut microbiota are primordial therapeutic phases which increase the surgical success.┬Ā
Regardless the fact that there are various treatment methods for RVF, they all depend on where the fistula is located and also on other potential comorbidities that the patient might have. Small dimensions RVFs are usually addressed using an approach at the anus, vagina, or perineal level (20). Transabdominal approaches are usually used to address superior fistulas. Treating fistula via anatomic processes is associated with a lower success rate compared to approaching it via a combination of the processes along with the adjuvant interposition of the healthy and vascularized tissue.
Rectovaginal fistulas represent a challenge for both the patients and the surgeons. Conventional therapy frequently fails which makes the surgical intervention to be the most sustainable approach for reconstructing the fistula.
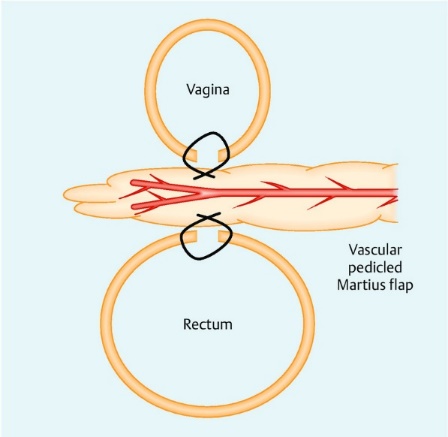
┬ĀOne surgical procedure that offers the proper reconstruction of the lower and median rectovaginal fistulas consists of the interposition of a bulbocavernosus tissue flap and is called the Martius modified labial fat pad flap or shortly Martius flap. Being firstly approached by professor doctor Heinrich Martius in 1928 at Gottingen, the Martius technique was afterwards modified and adjusted. Nowadays, it is used in the reconstruction process of various anomalies of the pelvic floor. The global success rate of the interposition of the Martius flap as additional procedure in the surgical process of the RVF s reported in the specialized literature and publications was of 65-100% [21].
After a horizontal perineal incision, the rectovaginal area (Tyrell fascia and Proust-Barbilian septum) is stabled, the fistula is dissected, while the posterior vaginal wall and the rectal mucosa are closed with unique stitches. When putting in practice the Martius procedure, there is only one area used for the reconstruction of the RVFs. Following precise measurements (6 cm ŌĆō perineum, 45 degrees ŌĆō antero-cranial direction and 8 cm ŌĆō cranial), a second major incision is performed, that of the vertical labia, with the aim of dissecting the posterior adipose tissue flap. The modified Martius flap procedure is later transferred on the back side, under the ischiocavernosus muscle and then stitched with no tension in the rectovaginal area, so that it would overlap with the vagina stiches and the rectal ones [22].┬Ā
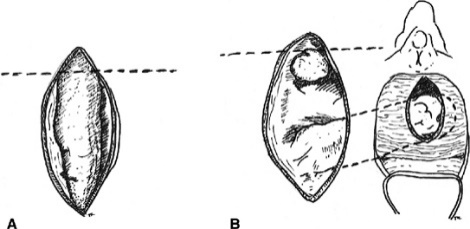
A. The fibrofatty tissue is mobilized with preservation of either the superior or the inferior blood supply.
B. The graft is tunneled to the site of the repair (23).
Case presentation┬Ā
The study case presented was of a 33-year-old woman previously diagnosed with squamous carcinoma of the cervix FIGO IIIA (2017) treated through means of curative radiochemotherapy, utero-vaginal intracavitary brachytherapy (GammaMed plus iX 14 Gy/PTV-HR/ 2 weeks). In April 2021, she presented herself at the surgery unit claiming exclusion of fecal through the vagina and constant perineal pain. As a result of the clinical examination of the Milligan perineal area (vaginal touch, rectal touch), and presenting a positive Carey test (the methylene blue test ŌĆō positive, bubble air test ŌĆō positive), it was confirmed a recto-vaginal connection, positioned at around 3-4 cm from the EAS. It was then decided an endoscopic exploration (sigmoidoscopy) whose results confirmed a recto-vaginal connection at about 4 cm from the EAS, with a diameter of approximately 1 cm. This was followed by a loco-regional exploration through pelvic MRI scan which confirmed a lower recto-vaginal connection (fistula), situated at approximative 3 cm from the EAS, with a diameter of 8 mm (Rothenberger I). It was afterwards decided to collect a circumferential biopsy at the fistula situs level (EHP: lymphoplasmacytic inflammatory sample, without any indication of local tumor relapse). As a first therapeutic step, we procured a diversion of the fecal matter (for 8-12 weeks) using as the main procedure the Volkmann colostomy. This was done through laparoscopic procedure, with a favorable postoperative evolution. The dynamic observation of the case took place every 4 weeks. However, during the process, the patient got infected with SARS COV2, presenting mild symptoms (the patient didnŌĆÖt have any vaccine administrated at that time), for which she was put under conventional therapy which delayed the initial symptoms, followed by an imagistic reevaluation (thoracic CT scan ŌĆō no significant changes, CO-RADS 1), all this situation imposing a delay of the surgical intervention.┬Ā
┬Ā After 4 weeks from the infection with the SARS COV2, respectively 16 weeks from the fecal diversion, it was decided it was safe to reconsider the surgical intervention. It was performed, nonetheless, a preoperative local evaluation (rectal touch, vaginal touch, Lockhart-Mummery sample) which revealed an oversized fistula sphincter (approximately 2.5 ŌĆō 3 cm) compared to the initial clinic-imagistic examination, which resulted in reclassifying the disease stage to RVF Rothenberger II.
Operative details
The preoperative procedures for the patients diagnosed with RVF include the clinical examination (Carey test, Lockhart-Mummery test), other paraclinical examination such as panendoscopy/sigmoidoscopy, MRI scan, and in some cases even endoanal ultrasonography (EUS) or bowel cleansing, either by mechanicals means or by using medication. The evaluation of the postoperative sexual life quality and the evaluation of the incontinence scale is done by using the Female Sexual Function Index (FSFI) along with the Wexner or Cleveland Clinic Incontinence Score (CCIS).
Surgical technique┬Ā

Figure 1:┬ĀLockhart-Mummert probe. RVF Rothenberger II

Figure 2:
Operative technique
After a horizontal perineal incision (Fig. 1), the rectovaginal space (Tyrel fascia and Proust-Barbillian septum) is mobilized, the fistula is dissected, and the posterior vaginal wall and rectal mucosa are closed with single sutures. Only one operating field is used for RVF repair in the Martius procedure. After precise measurement (6 cm from the perineum, 45 degrees in an anterior-cranial direction and 8 cm cranially), the second vertical labia majora incision (Fig. 2) is made to dissect the posterior pedicled adipose tissue flap. The modified Martius flap is then pivoted dorsally under the ischiocavernosus muscle and sutured without tension in the Tyrel fascia or rectovaginal space to separate vaginal and rectal sutures [24-25].

Figure 3┬Ā┬Ā
┬Ā ┬Ā ┬Ā Figure 4
Figure 3-4:┬ĀTranslocation of the pediculated cutaneous-adipose flap from the paralabial left side to the posterior vaginal wall, followed by its repair using a┬Ā 3-0 vicryl stitch. The anterior vaginal wall is stitched biplanar using a slow-absorbing 3-0 vicryl stitch.
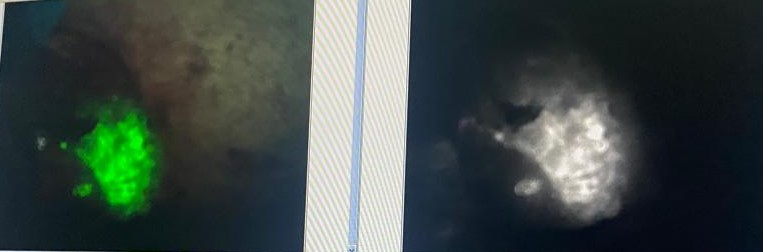
The intravenous injection of approximately 0.1mg/kgc of ICG followed by the examination of the vascularization of the cutaneous-adipose flap.

Figure 5:┬ĀJackson-Pratt drainage type. Left biplanar paralabial stitch done using a 3-0 slow-absorbing vicryl. Pudental nerve block with postoperative analgesic purpose.

Figure 6:┬ĀPostoperative image after 48 hours.
The time duration of the surgery was of about 140 minutes, no intraoperative or postoperative complications were reported according to the Clavien-Dindo classification. The evolution of the surgical wounds (perineal, respectively pudendal ones) was a favorable one as a result of the per primam epithelialization process, without any reporting of local complications. After 72 hours from the surgery, the Jackson-Pratt drain was also removed. The restoration of the continuous bowel transit took place in phase 3 of the therapy process, at about 10 weeks since the repair applying the Martius flap procedure.
The rectal and vaginal permeability was preserved at the normal level, sphincter tonus normal nature, no sign of incontinence according to the Wexner classification, and normal sexual activity according to the FSFI scale (approximately 6 months postoperative the patient went through a progressive vaginal dilation using Frank procedure).
In specialized literature, Pinto et al. outlined a success rate of 87
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal ŌĆ£Brain and Neurological DisordersŌĆØ. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassleŌĆæfree, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
