
Research Article | DOI: https://doi.org/10.31579/2692-9562/150
1Department of Otolaryngology, the Second Hospital of Sanming,Sanming, Fujian,China.
2Department of Endocrinology, the Second Hospital of Sanming, Sanming, Fujian, China.
3Department of Otolaryngology-Head and Neck Surgery, National Regional Medical center, Binhai Campus of the First Affiliated Hospital, Fujian Medical University, Fu Zhou, Fujian, China.
4Department of Otolaryngology-Head and Neck Surgery, the First Affiliated Hospital, Fujian Medical University, Fuzhou, Fujian, China.
5Allergy Center, the First Affiliated Hospital, Fujian Medical University, Fuzhou, Fujian, China.
*Corresponding Author: Wei Lin., Allergy Center, the First Affiliated Hospital, Fujian Medical University, Fuzhou, Fujian, China.
Citation: Keliang Zheng, Yingchun Zheng, Yonghong Lei, Jing Lin, Wei Lin, (2025), Modifiable Factors for Tinnitus: A Mendelian Randomization Study Analysis, Journal of Clinical Otorhinolaryngology, 7(4); DOI:10.31579/2692-9562/150
Copyright: © 2025, Wei Lin. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 11 September 2025 | Accepted: 12 September 2025 | Published: 19 September 2025
Keywords: joint disorders; disease; blood pressure
Objective:
The topic of tinnitus has received considerable scholarly interest. Contributing factors to the development of tinnitus encompass aging, exposure to loud noises, smoking, and hearing impairment. Nevertheless, the precise risk factors, particularly those that can be modified, remain uncertain. This study aims to explore the potential genetic factors that may be associated with an increased susceptibility to tinnitus.
Methods:
Mendelian randomization analyses were performed using data from the United Kingdom Biobank and FinnGen Biobank data infrastructure. The present study examined the correlation between thirteen prevalent life factors, which were identified as potential risk factors for tinnitus through a comprehensive review of tinnitus risk factors. This investigation employed an inverse-variance weighted (IVW) model to analyze the association. To mitigate database source bias and strengthen the reliability of our findings, the UKB data was utilized for the discovery cohort, while the Finnish database served as the validation cohort. Following this, a meta-analysis was conducted to amalgamate the findings, thereby bolstering the robustness of the results.
Results:
Following a thorough process of MR Quality control and exposure screening, we have identified and chosen 13 risk factors as exposures through careful observation. We discovered significant associations between exposure to the UKB database and the occurrence of tinnitus. Specifically, waist circumference, waist-hip ratio, fasting blood glucose, and fasting insulin were identified as causal factors for tinnitus. Our analysis revealed that waist circumference (IVW, p=0.006, OR=1.37, 95% CI, 1.09-1.71, Cochran Q statistics=13.47, Pheterogeneity=0.2), waist-to-hip ratio (IVW, p=0.005, OR=1.71, 95% CI, 1.17-2.50, Cochran Q statistics=36.5, Pheterogeneity=0.1), fasting blood glucose (IVW, p=0.007, OR=0.7, 95% CI, 0.54-0.9, Cochran Q statistics=34.46, Pheterogeneity=0.59), and fasting insulin(IVW, p=0.03, OR=2.07, 95% CI, 1.07-4.01, Cochran Q statistics=24.95, Pheterogeneity=0.58) all exhibited significant associations with tinnitus.In the validation cohort (Finnish database), our subsequent analysis revealed that smoking exhibited a causal relationship with tinnitus (smoking, IVW, p=0.018, OR=1.20, 95% CI, 1.03-1.40, Cochran Q statistics=52.83, Pheterogeneity=0.86). To analyze these findings, a meta-analysis approach was employed (Waist circumference, p=0.003, OR=1.27, 95% CI, 1.08-1.49,I2=0.00%).
Conclusions:
Our research findings provide evidence supporting a causal association between waist circumference and tinnitus, potentially influenced indirectly by obesity-related indicators. Thereby furnishing substantiation for potential tinnitus prevention measures in subsequent research endeavors.
Tinnitus is defined as the perception of non-speech sound in the absence of an external acoustic stimulus [1]. Tinnitus pathophysiology is not limited to the auditory system alone [2]. Some models of tinnitus pathophysiology suggest that networks associated with attention, memory, distress and multisensory experience are involved in tinnitus perception [3]. Tinnitus is an extremely prevalent condition that impinges on the lives of sufferers to varying degrees. A meta-analysis shows that the prevalence of tinnitus ranges from 11.9 to 30.3% using the same definition of tinnitus[4]. Suffering from tinnitus causes mental distress in most patients [5]. In some people, it is a fairly minor irritation but, for many, the tinnitus intrudes to such a degree that it affects their ability to lead a normal life, and in some very extreme cases has resulted in suicide [6]. It is a very common medical symptom, and some studies show that 5 to 15% of adults had tinnitus in life. It is a condition that could be chronic and for some patients could be very debilitating [7]. A large cross-sectional study involving children and adults who were referred to a regional otolaryngology hospital showed that 97% of those who reported tinnitus had concomitant hearing loss detected by routine audiometry [8]. In addition, tinnitus impact was found to predict increased depression, anxiety sensitivity, and reduced quality of life [9]. At presentation, the possibilities of otological disease, anxiety, and depression should be considered. No effective drug treatments are available, although much research is underway into mechanisms and possible treatments [10]. The causes of tinnitus are varied, but remain unclear in most individual cases [10,11]. However, in some situations, a single hypothesis cannot accurately explain the cause of tinnitus [12]. The objective of our study was to investigate the genetic predisposing factors associated with tinnitus. The numerous etiologies, such as aging (presbycusis), noise exposure, stress, hypertension, diabetes, ototoxic medications, temporomandibular joint disorders, traumatic or ischemic damage, vascular problems, middle-ear problems, and the complex pathophysiology involving peripheral and central auditory and non-auditory structures, have led to the belief that tinnitus is a consequence of some other disease [13].Evidence was also found for a number of non-otological risk factors including temporo-mandibular joint disorder, depression, chronic obstructive pulmonary disease, and hyperlipidemia. Negative associations indicating preventative effects were found for diabetes and high alcohol consumption [14]. Multiple associated factors have been identified, including cardiovascular, psychological, neurological, musculoskeletal and dietary factors [15]. Hypertension and former smoking were associated with an increase in odds of frequent tinnitus [16]. Loud leisure-time, firearm, and occupational noise exposure also were associated with increased odds of frequent tinnitus (16). The tinnitus prevalence increased with age (adjusted odds ratio [AOR], 1.087). Female gender (AOR, 1.401), sleeping less than 9 hours (sleep 7 or 8 h: AOR, 1.437; sleep 6 h or less: AOR, 1.737), noise exposure in other places (AOR, 6.395), and momentary noise exposure (AOR, 5.504) increased the risk of tinnitus [17]. These studies are observational studies, which are susceptible to subjectivity, operational errors, and so on. That makes these studies unreliable. Mendelian randomization uses genetic variants to determine whether an observational association between a risk factor and an outcome is consistent with a causal effect. Mendelian randomization relies on the natural, random assortment of genetic variants during meiosis yielding a random distribution of genetic variants in a population [18]. Mendelian randomization (MR) is one approach to overcome confounding [19]. Mendelian randomization (MR), by using genetic variants randomly allocated at conception as instrumental variables, is less susceptible to confounding than conventional observational studies [20]. The employment of Mendelian randomization (MR) techniques has experienced a noticeable surge in recent years in order to estimate the causal influence of risk factors (exposures) on diseases (outcomes). Consequently, we employed MR methodology to investigate the risk factors associated with tinnitus. This study offers a foundation for both prevention and treatment approaches.
2.1 MR produce
In this particular investigation, a mendelian randomization three assumptions was employed, as depicted in Figure 1. The single nucleotide polymorphisms (SNPs) were found to have a direct association with the exposure to modifiable risk factors. Furthermore, it was determined that these SNPs were not influenced by any confounding factors. Lastly, the SNPs were observed to solely impact the occurrence of tinnitus through their effect on the exposure to modifiable risk factors.

Figure 1: Mendelian randomization three assumptions.
2.2 The summary statistic of modefiable risk factors:
We obtained measurements of Body mass index (BMI), waist circumference, hip circumference, and waist-to-hip ratio from the GIANT (Genetic Investigation of A Nthropometric Traits) consortium. The covariates considered in our analysis included sex, age, age squared, and principal components. In the body mass index (BMI) genome-wide association study (GWAS), a total of 681,275 European individuals and 2,336,260 single nucleotide polymorphisms (SNPs) were included. In the waist circumference GWAS, 60,586 European individuals and 2,744,366 SNPs were included. For the hip circumference GWAS, 225,487 individuals of mixed ancestry and 2,542,663 SNPs were included. Lastly, in the waist-to-hip ratio GWAS, 99,076 individuals of mixed ancestry and 2,146,958 SNPs were included. We obtained measurements of total cholesterol, high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), and triglycerides from the Global Lipids Genetics Consortium (GLGC). The variables included in the analysis as covariates were sex, age, age squared, and principal components. The GWAS for total cholesterol involved a sample size of 187,365 individuals of mixed ancestry and analyzed 2,446,982 single nucleotide polymorphisms (SNPs). Similarly, the GWAS for HDL-C included 187,167 mixed individuals and examined 2,447,442 SNPs. The GWAS for LDL-C encompassed 173,082 mixed individuals and investigated 2,437,752 SNPs. Lastly, the GWAS for triglycerides involved 177,861 individuals of mixed ancestry and analyzed 2,439,433 SNPs. Fasting glucose and fasting insulin were obtained from the MAGIC (Meta-Analyses of Glucose and Insulin-related traits Consortium), while the covariates considered in the analysis included sex, age, age squared, and principal components. In the GWAS analysis of fasting glucose, a total of 133,010 European individuals and 64,432 single nucleotide polymorphisms (SNPs) were included. Similarly, for the GWAS analysis of fasting insulin, a cohort of 108,557 European individuals and 64,421 SNPs were incorporated. We obtained data on smoking and drinking habits from the GWAS and Sequencing Consortium of Alcohol and Nicotine use, while controlling for covariates such as sex, age, age squared, and principal components. The GWAS analysis for smoking encompassed a sample size of 337,334 European individuals and 11,913,712 single nucleotide polymorphisms (SNPs). Similarly, the GWAS analysis for drinking involved 335,394 European individuals and 11,887,865 SNPs. The Type 2 diabetes mellitus (T2DM) data was obtained from the DIAGRAM database, with the covariates consisting of sex, age, age squared, and principal components. The T2DM genome-wide association study (GWAS) included a total of 110,452 individuals of mixed ancestry and analyzed 2,915,012 single nucleotide polymorphisms (SNPs).
2.3 The summary statistic of tinnitus:
The genome-wide association studies (GWAS) conducted on tinnitus involved the utilization of the UK Biobank (UKB) biobank(https://www.ukbiobank.ac.uk), which encompassed a sample size of 3,625 individuals of African American or Afro-Caribbean descent and 15,538,145 single nucleotide polymorphisms (SNPs). Additionally, the FinnGen consortium (https://www.finngen.fi/en) was also involved in the GWAS, employing a sample size of 3,502 European individuals with tinnitus, 196,592 control individuals, and 16,380,426 SNPs. Figure 2 provides an overview of the study design employed in this research. A manual search was conducted in the PubMed database to identify modifiable risk factors related to disease, diet and lifestyle, metabolism, and infection. The outcome datasets consisted of summary statistics for SNPs associated with these risk factors, with a significance threshold of p < 5 KB=10000, r2=0.001.>
Figure 2: Analysis framework of the article
The Cochran's Q-test was employed to evaluate the heterogeneity of causal estimates across single nucleotide polymorphisms (SNPs) using the IVW method. The results of this study did not indicate any significant heterogeneity for the exposures examined (P > 0.05). Furthermore, the MR-PRESSO test was utilized to identify potential outliers with horizontal pleiotropy, and no outliers were detected (P > 0.05).
2.4 statistical analysis.
The statistical analyses were conducted utilizing the Two SampleMR package in R statistical software, version 4.1.2, provided by the R Foundation in Vienna, Austria. A two-tailed p-value of less than 0.05 was deemed to be statistically significant.
3.1 Validation results of tinnitus in the UKB consortium
In an exploratory analysis utilizing data from the UKB outcome source, a significant causal relationship was observed between waist circumference (odds ratio [OR], 1.37; 95% confidence interval [CI], 1.09–1.71; p = 0.006), waist-to-hip ratio (odds ratio [OR], 1.71; 95% confidence interval [CI], 1.17–2.50; p = 0.005), fasting glucose (odds ratio [OR], 0.7; 95% confidence interval [CI], 0.54–0.90; p = 0.007), fasting insulin (odds ratio [OR], 2.07; 95% confidence interval [CI], 1.07–4.01; p = 0.03), and tinnitus using the IVW method (Figure 3).The four aforementioned results did not exhibit any heterogeneity or horizontal pleiotropy, as indicated by the statistical tests(Pheterogeneity>0.05 and Ppleiotropy>0.05).
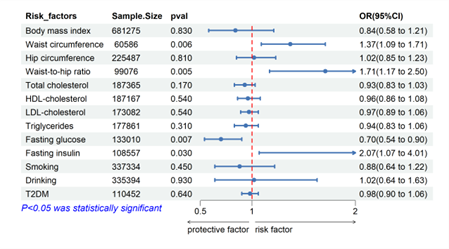
Figure 3: Forest plot of Mendelian randomization results from UKB.
3.2 Validation results of tinnitus in the FinnGen consortium
In a preliminary investigation utilizing the FinnGen Biobank as the source of outcome data, a statistically significant association was identified between smoking and tinnitus using the inverse variance weighted (IVW) method (odds ratio [OR], 1.20; 95% confidence interval [CI], 1.03–1.40; p = 0.018) (Figure 4). Furthermore, no evidence of heterogeneity or horizontal pleiotropy was found (Pheterogeneity > 0.05 and Ppleiotropy > 0.05).

Figure 4: Forest plot of Mendelian randomization results from FinnGen consortium.
3.3 Combined result of cholelithiasis from
In order to enhance the robustness and reliability of the findings, a post-MR meta-merge was conducted, incorporating tinnitus data from both Finland and UKB. Meta-analysisIn shouw that were combined for Meta-analysis, revealing that only waist circumference (odds ratio [OR], 1.27; 95% confidence interval [CI], 1.08–1.49; p = 0.003) remained significantly associated with the outcome. The selection of the model type was based on heterogeneity (I²) and a random effects model was chosen. (Figure5)

Figure 5: Forest plot of Mendelian randomization results from meta-analysis.
This Mendelian randomization study has successfully established a causal relationship between genetically determined increases in waist circumference and the risk of tinnitus. Moreover, within the tinnitus sample exclusively selected from the UK Biobank, four risk factors have been identified as causally associated with tinnitus. Furthermore, the tinnitus sample obtained from the Finnish database has revealed the presence of only one risk factor, namely smoking, that exhibits a causal association with tinnitus. Discrepancies in findings can be attributed to the failure to account for significant confounding variables in certain studies, as well as variations in the definition of tinnitus, the duration of analysis, and the selection of the study population. Factors such as socioeconomic status and lifestyle, which are frequently encountered in conventional observational studies, have the potential to influence the interpretation of results. With hearing loss, older age, male gender, high BMI, higher deprivation, higher blood pressure, smoking history, as well as numerous comorbidities being associated with higher odds of current tinnitus(20). In a systematic review of studies, For models of tinnitus presence, the most common predictors were age, gender and smoking(21). The utilization of a solitary outcome may introduce a potential bias stemming from the data source. The present body of research has begun to disclose a genetic architecture for tinnitus but there is still much work ahead for the identification of specific variants influencing critical gene expression and gene products in tinnitus pathophysiology(22).An important complicating factor is the heterogeneity in tinnitus causes and types(23–26).In contrast, our analysis encompasses a broader scope, encompassing tinnitus data from both the UK Biobank and Finland. By merging the meta-analysis of these two datasets, our findings exhibit enhanced reliability and robustness. In clinical practice, the primary etiologies of tinnitus are frequently examined. On one hand, it can be attributed to localized lesions within the auditory system, while on the other hand, it can be linked to lifestyle factors, encompassing sleep patterns, tobacco consumption, alcohol intake, and similar habits. Established cardiovascular disease and individual and combined cardiovascular disease risk factors were found to be associated with hearing loss(27). According to relvant reports, cardiovascular disease risk factors were found to be associated with hearing loss. Cardiovascular risk factors were assessed via objective measurements including blood pressure, body mass index, waist circumference, lipid profile and glycated haemoglobin (27).Three factors related to cardiovascular disease and its risk factors were associated with having tinnitus(alcohol consumption, Arthritis, use of NSAID medications)(28). we believe that atherosclerotic carotid artery stenosis should be considered a possible cause of pulsatile tinnitus, particularly in patients with cardiovascular risk factors(24).The results were consistent with the previous research- certain measures of cardiometabolic risk inculding waist circumference are weakly related to both reported tinnitus and level of tinnitus handicap(29).In subsequent research, it is advisable to conduct a more comprehensive examination of the underlying determinants of tinnitus, encompassing anatomical characteristics (e.g., hip bone dimensions, hip joint functionality) and lifestyle factors (e.g., prolonged sitting or standing, preference for supine positioning). In the present study, we have successfully established a causal association between waist circumference and tinnitus, thereby highlighting its potential significance in the prevention of tinnitus. This finding is primarily attributed to the comprehensive nature of our Genome-Wide Association Study (GWAS), encompassing diverse sources of data and exposure variables, and further reinforced by a meticulous meta-analysis. Despite the absence of potential pleiotropy or heterogeneity in the sensitivity analysis conducted in this study, it is important to acknowledge that there may still be unresolved bias due to the utilization of different data sets for exposures and outcomes. While the current Mendelian randomization (MR) Study successfully established a causal association between waist circumference and tinnitus, further investigation is required to determine the precise threshold of waist circumference control necessary for managing tinnitus.
Not applicable.
Authors’ contributions
keliang ZHENG: Formal Analysis, Writing–original draft. Wei LIN: Formal Analysis, Writing–original draft,Supervision, Writing–review and editing.yingchun ZHENG: Writing–original draft.yonghong LEI: Writing–original draft. ,jing LIN: Visualization, Writing–original draft. 5: Visualization, Writing–original draft. 6:
Funding
There was no financial support for the research.
Availability of data and materials
Summary statistics for all neoplasms and HPV are available on the IEU GWAS database (https://gwas.mrcieu.ac.uk/).
Ethics approval and consent to participate
Our study used summary statistics from publicly available GWAS (https://gwas.mrcieu.ac.uk/),which followed the protocol approved by the respective institutional review boards, obtained informed consent from all participating studies, and did not require separate ethical approval.
Consent for publication
Not applicable.
Competing interests
All authors declared that they have no potential conflicts of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
