
Research Article | DOI: https://doi.org/10.31579/2690-8808/170
Department of nursing, college of medicine and health science, Wolkite University, Wolkite, Ethiopia.
*Corresponding Author: : Shegaw Tesfa, Department of nursing, college of medicine and health science, Wolkite University, Wolkite, Ethiopia.
Citation: Shegaw Tesfa, Tadesse Tsehay, Tebibu Solomon, (2023), Modern health seeking behavior and its determinant factors among household heads in the rural community South West Ethiopia, 2022. Community based cross-sectional study, J, Clinical Case Reports and Studies, 4(4); DOI:10.31579/2690-8808/170.
Copyright: © 2023, Shegaw Tesfa. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 05 May 2023 | Accepted: 15 May 2023 | Published: 20 May 2023
Keywords: modern health seeking behaviors; house hold heads; wolkite; ethiopia
Background: Healthcare seeking behavior refers to any activity or inaction made by people who believe they have a health issue or are ill with the intention of finding a suitable treatment. The timing and types of healthcare services used today can affect population health outcomes.
Objective: To assess modern health seeking behavior and its determinant factors among household heads in the rural community South West Ethiopia, 2022.
Method: A community based cross sectional study was employed. A systematic random sample technique was used to collect information from 410 participants through an interviewer-administered questionnaire. Data were entered into Epi-data version 3.1 and exported to SPSS version 26 after being checked for completeness. The significant variables were determined using bivariate and multivariate logistic regression analysis.
Result: The overall level of modern health seeking behavior was low (74.9%). Variables being elder age (AOR=4.287, 95% CI (1.133, 16.223)), illiterate (AOR =4.075, 95%CI (1.094, 15.180)), and family size (AOR=5.826, 95% CI (3.097, 10.960)) were significantly associated with low level of modern health seeking behavior.
Conclusion: The community has low level of modern health-seeking behavior among household heads, and relatively being elder age, illiteracy, and family size were prominent predictors of low level of modern health seeking behavior.
The concept "healthcare seeking behavior" (HSB) refers to any activity or inaction made by someone who believes they have a health issue or are ill with the intention of finding an appropriate remedy[1]. Health seeking behavior belongs under the broader definition of health behavior, which includes actions taken to maintain good health, prevent illness, and respond to any deviation from a good state of health [2]. Delaying medical attention is linked to a higher chance of adverse outcomes, and healthcare-seeking behavior includes the timing and types of healthcare service utilization [3].
Health-seeking behavior is an activity that promotes, protects or maintains one's health, regardless of actual or perceived health. In most areas, western science and medicine account for only a small portion of medical care and medical workers are frequently in low supply because most medical services are delivered outside of the jurisdiction. To understand how people use medical services, we must first understand how they interpret their symptoms [4].
According to the Ethiopian Demographic and Health Survey (EDHS), 44% of households used some type of health care service, 31% treatment for sick people` and 24% immunization, and majority of households 50% government health station or clinic, and 15% private health facilities [5]. Poor healthcare seeking behavior has been linked to ineffective morbidity and mortality prevention, and control in the context of health problems [6].
Evidences described that socioeconomic status, geographic contexts, cultural concerns, service quality, and health system policies and procedures are all factors that influence community health seeking behavior and individuals with higher modern health seeking behavior may have better ability on the disease prevention and maintenance of health condition [7], and individuals who get previous health information are more likely to seek medical health care [8].
Health care usage is influenced by geographic, economic, and social constraints, as well as a lack of health care coverage. As a result, knowing how individuals seek health care may have a huge influence on how health services are created so that people get most out of them and it is critical to improve medical care. There is presently a scarcity of data from a community based research to back up the initial steps in providing improved health care to the community. Because it highlights the sociocultural processes that promote or discourage individuals from seeking medical treatment, such data is valuable for planning, coordinating, and implementing health-care delivery systems [9].
Modernhealthseekingbehavior is a complex phenomenon that requires thorough examination in order to give information that will aid in the development of healthcare policy and programs. Most studies on health-seeking behavior in Ethiopia have been disease specific particularly on malaria, TB, and maternal health [10]. Since no similar study in the study area on health care seeking behavior in the household level, this study help to assess the health seeking behavior among household heads and identified factor affecting health care seeking behavior.
Understanding the modern health seeking process may have a huge influence on how health services are structured so that individuals can get the most out of them. It is critical to improve medical care and make it more accessible to people who require it. This improving a country's health condition requires increasing access to health care services. Understanding people's health related behaviors, on the other hand, is a critical component in enhancing community health at both the individual and community levels.
Information obtained from a community based research can aid in the development, organization, and implementation of health care delivery systems. Understanding people's health related behavior is also a necessary step for policymakers to develop effective treatments. Therefore, this study is expected to give insight to government body and different Non-Governmental Organization (NGO) about modern health seeking behaviour of the community and help to guide the health care providers and other concerned stakeholders to work more towards alleviating the problem. The finding of this study will also might be used as a base line data for other researchers interested on this area.
General Objective
To assess level of modern health seeking behavior and its determinant factors among household heads in the rural community Southh West Ethiopia, 2022.
Specific Objective
To assess the level of modern health care seeking behavior behaviors among house hold heads in the rural community South West, Ethiopia, 2022.
To identify determinant factors associated with modern health seeking behavior among house hold heads in the rural community South West, Ethiopia, 2022
Study area and period
The study was conducted in Wolkite Town, which is the capital city of Gurage Zone, South West, Ethiopia and 158 km far from Addis Ababa and 429 km away from Hawassa, capital city of the South Nation Nationality people of Ethiopia (SNNPR). Wolkite Town is located between latitude of 8 17 ̸N 37 47 ̸E and longitude of 8.283 N 37.783 E with an elevation of 1,910 and 1,935 meters above the sea level. The total population of the Town is about 92,512. The structural plane of wolkite town is set up from three sub city, which are Bekure, Addis Brihan and Gubreye sub city. The study was conducted from March to June, 2022.
Study design
A cross sectional study design was employed
Source of population
All adult population living in Wolkite Town
Study population
All households in Wolkite Town sub city
Study unit
All selected households in each sub city
Inclusion and Exclusion Criteria
Inclusion Criteria
All household heads lives in Wolkite Town age greater than 18 years old present during data collection period.
Exclusion Criteria
Critically ill, physically impaired unable to communicate and speech
Sample size and sampling procedure
Sample size determination
Sample size was determined by using single population proportion formula considering the following assumptions; using the prevalence of 58.4% from similar study done among community in South, Ethiopia [11]. Confidence interval of 95%, margin of error 5%, and 10% of non-respondent rate.

Where, n=required minimum sample size
z=z-score value corresponding to a given level of confidence
p=estimated population proportion
w=allowable margins of error
We add total non-respondent rate of 10%
373+37=410
Sampling technique
Wolkite Town was stratified in to three sub city, which is Bekure, Addis Birhan and Gubrye sub city and each household was selected from each stratum using simple random sampling methods.
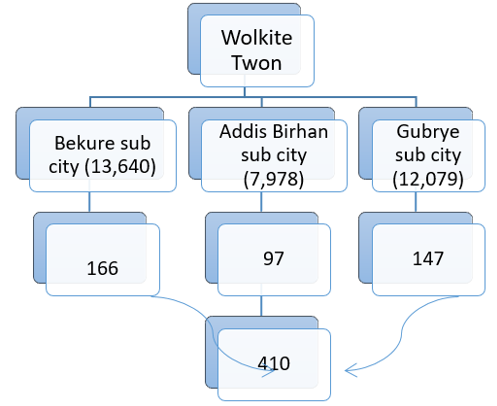
Figure 1: Schematic presentation of sampling procedures
Operational Definition
Modern health seeking behavior: having a score ≥ the mean on each of the target dimensions was equated with having a high level of health seeking behavior and participants having a score below the mean on one of the target dimensions were equated with having a low level of health seeking behavior.
Data collection tool and quality assurance
Data was collected via standardized questionnaires prepared in English language and then translated into the national language, Amharic and translated back to English to ensure its consistency and accuracy. The tool consists of three parts socio demographic part, participants’ personal characteristics, and health seeking behavior parts, which adapted from WHO STEPS instrument and global physical activity questionnaire (GPAQ) modification with reliability of coefficient of 0.88 (12) . The questionnaire was pretested on 5% of the calculated sample size out of the study area. Data were collected by six trained 4th years nursing graduating class students and two senior nurse supervisors after one day training. Finally, filled questionnaires were checked for its completeness and consistency of the data by the principal investigator on daily basis.
Statistical Analysis
Data entry was done by using Epi-Data version 3.2 and exported to SPSS version 26 for analysis. Descriptive statistics was used to determine frequency, percentage and graphs, and binary logistic regression analysis variables with P-value <0>
Socio demographic Factors
A total of 410 households heads were involved in this study with the response rate of 100%. Among the study participants male comprises 228 (55.6%) and 182 (44.4%) were females. Majority of individual 159 (38.8%) lies at the age group of 26-35 years. Two hundred eleven (51.5%) of study participant had monthly income between 1000-4000 birr. Two hundred thirty seven (57.8%) of the households have a family size of greater or equal to 5 (Table1).
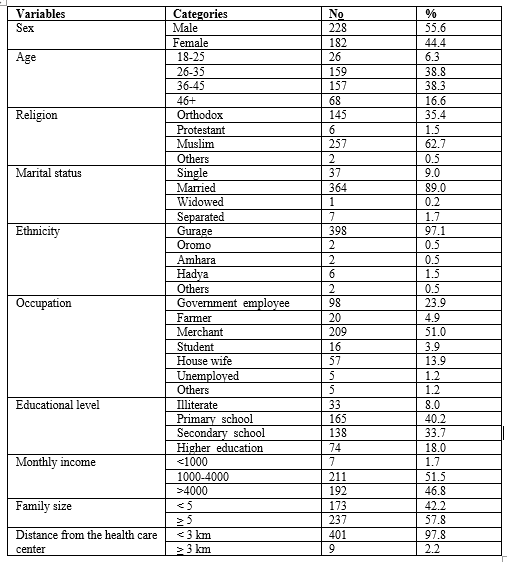
Table 1: Socio-economic and demographic characteristics of participants (n=410) in Wolkite town, Gurage Zone, SNNPR, Ethiopia, June 2022
Accordingly, 392 (95.6%) took action when got ill. 271 (66.1%) of participants undertook screening for general health status and 139 (33.9%) of study participants did not took screening. Similarly, more than forty percent (47.8%) participants did not undertake health oriented leisure activities (Table 2).
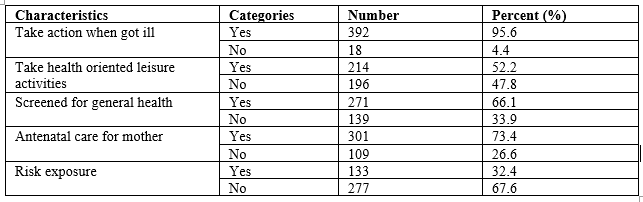
Table 2: Health-seeking behavior of study participants in Wolkite town, Gurage Zone, SNNPR, Ethiopia, 2022
Health care seeking behavior in the household level
From the study participants only 25.1% the households had high health care seeking behavior; while 74.9% had low health care seeking behaviors.
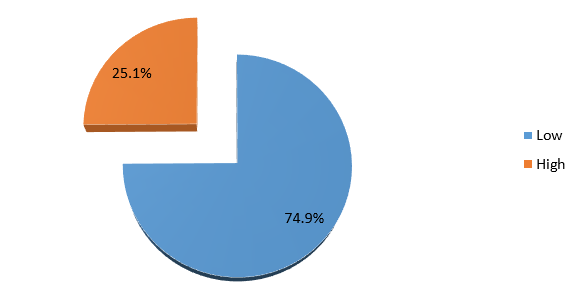
Figure 2: Level of modern health seeking behavior, Wolkite Town, 2022Factors associated with modern health seeking behaviors
In multivariate logistic regression analysis variables like age, family size, and level of education were independently associated with modern health seeking behavior.
The odds of having low level of modern health-seeking behavior among participants age between 36-45 years was 2.8 times higher than those participants age between 18-25 [AOR=2.8,95% CI: (1.023,7.819)].
Similarly, households whose family size greater or equal to five were 5.6 times more likely to have low level of modern health seeking behavior than those households heads whose family size less than five [AOR=5.6,95% CI:( 3.043,10.120)].
Those households heads being illiterate were (AOR = 4.2, 95% CI :( 1.166, 15.010)) 4.2 times more likely to have low level of modern health seeking behavior than those households heads with educational status of higher education and above (Table 3).
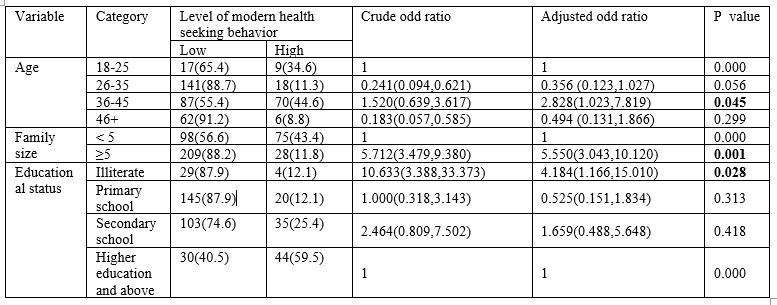
Table 3: Variables significantly associated with modern health-seeking behavior in Wolkite Town, South West Ethiopia, 2022
Prompt and appropriate care seeking practices have importance to reduce death from diseases morbidity and mortality. Many evidences suggest that addressing health seeking behavior pave ways for appropriate utilization of health care services [13]. This study tried to measure level of modern health-seeking behavior in multidimensional approaches among household heads to improve health behavior in the prevention of disease and promotion of health.
In this study, magnitude of modern health seeking behavior among household heads was 25.1%, which line within (95% CI; 21.3-28.8). This extent of modern health-seeking behavior was remarkably low when compared to the study done in Turkey 87.8% [14], India 79% [15], and
Malaysia 35.4% [16]. Also this finding was similar to the studies reported from Bangladesh 42% [17], Northern Ethiopia 43.2% [18], Nigeria 44.2% [19], and Dale Woreda, Sidama Zone, Ethiopia community 72.8% [20]. However, this finding was relatively higher than the report finding of health-seeking behavior of people living in Hosanna Town community, Southern Ethiopia14.6% [21]. The discrepancy could result from different methodologies (difference in geographical differences, sampling techniques and in operational definition of the dependent variable, modern health seeking behavior). In any case, this study suggests that major behavioral interventions are required to enhance health-seeking behavior in order to raise community health service utilization rates.
When they became ill, almost 95.6% of the patients in our study sought medical attention. This outcome was nearly identical to the study carried out in Dale Woreda, Sidama Zone, Southern Ethiopia, at 89.9% [20]. Comparing the current study to studies conducted in Zambia (43.5%) and the Amhara region of Ethiopia (52.3%), there is a decline in the use of health services [22] and Nigeria 48.9% [23]. The improvement may be attributable to ongoing efforts to improve the infrastructure, public awareness, and engagement of community health extension workers.
A decision not to use maternal and child health services was also viewed as an indicator of low health-seeking behavior. In light of this, the outcome indicated that it was 73.4% for maternal and 66.1% for pediatric health issues, however it is higher than the report finding from EDHS 2016 in Ethiopia [23]. This might be as a result of the fact that our sample was fully urban-based, unlike EDHS, which includes both urban and rural areas across the nation, as well as the fact that the survey and the study were conducted at different times.
The results illustrated that variables being older aged, family size, and level of education was significantly associated with low level of modern health seeking behavior.
Age was one of the variables which significantly affect health care seeking behaviors of household heads. The odds of having low level of modern health-seeking behavior among participants age between 36 -45 was 2.82 times higher than those participants age between 18 -25. This finding was the same with the report finding conducted in Uganda [24], Zimbabwe [25], Sidama Zone, Southern Ethiopia [20]. This might be due to elderly aged individuals be retired, jobless, and may have any source of income to attend health facility for maintaining their health, and may have higher sense of responsibility to the family with regards to basic need adequacy, and lack time to seek health facility.
In this study, family size was significantly associated with low level of modern health seeking behavior; household heads whose family size > 5 were 5.55 times more likely to have low health seeking behavior than those households heads less than five, which is mimic with the study revealed in Malaysia [16], North West Ethiopia [22]. This may be due to the fact that those with larger families are likely to carry more responsibility and have faced extreme socioeconomic difficulty, which has stopped them from getting the proper medical attention from modern health facilities for symptoms they have been experiencing.
The level of education of household heads has a substantial impact on their modern health seeking practices. When compared to household heads with better educational status and illiterate, individuals who were illiterate were 4.18 times more likely to face in low levels of modern health seeking activity. This finding was mimic to the study conducted in Turkey [14], India [15], and Southern Nigeria [26] community. Also the finding was similar with the report finding from Malaysia [16], and Bangladesh [17]. This may be because more educated people are more aware of health issues, more aware of the services that are available for healthcare, and more effective in applying this information to maintain or improve their health status.
Standardized and valid questionnaire was used and the study was included new variables did not address in different literature views. The cross-sectional nature of the study design does not confirm definitive cause and effect relationship. The study did not address qualitative section. Furthermore, reports for some of the questions were past history or encounters which are prone to recall bias.
In this finding, the overall level of modern health care seeking behavior among household heads was low, and variables being aged, increasing family size, and illiterate were significant predictors of low level modern health seeking behavior. Therefore, the national health care policy should establish home care service to keep the health status of elder individuals, standard number of family members within a house hold, and increase the educational status of the household heads to enhance modern health seeking behavior of the community.
AOR: Adjusted odd ratio; COR: Crude odd ratio; EDHS: Ethiopian Demographic and Health Survey; GPAQ: Global Physical Activity Questionnaire; HSB: Health Seeking Behavior; NGO: Non-Governmental Organization; WHO: World Health Organization; SNNPR: South Nation Nationality People of Ethiopia; SPSS: Statistical Package of Social Science
The datasets used and analyzed during the current study are available from the corresponding author under the permission of Wolkite University on reasonable request.
Wolkite University's Institutional Review Board (IRB) with ethical approval number RCSUILC/09/2022 has approved this study and the verbal informed consent process. All participants talked about the purpose of the study and the verbal informed consent to confirm their willingness. They notified that to have the right to refuse or terminate at any point of the interview and also the extracted information would not be used other than the study purpose.
The study did not include images or videos relating to an individual, but rather obtaining consent from each participant and information to publish the findings addressed, and participants agreed on that.
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
There is no funding to the study
The authors declare that there is no any conflict of interest in this work and that they have no financial or non-financial competing interests
First, we would like to thank almighty God for being with us in this all journey. Next, our gratitude is to Wolkite University, College of Medicine and Health Science and, Department of Nursing for giving the opportunity to do this research. Finally, our sincere appreciation goes to our advisors Mr. Shegaw T. and Mr. Tadesse T. for their mentorship, guidance, constrictive comment and suggestion and their dedication throughout the developments of this research.
ST: Draft proposal, lead data collection and analysis process wrote final thesis and prepare manuscript; TS: Revised and edit proposal & thesis, support data collection and analysis, revised thesis manuscript; TT: Reviewed different literatures, revised proposal, and manuscript and participated in data collection. All authors revised, consent and approved the final version of the thesis and manuscript.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
