
Research Article | DOI: https://doi.org/10.31579/2641-0419/103
1Division of Rheumatology, Tygerberg Academic Hospital, National Health Laboratory Services. Faculty of Health Sciences, Stellenbosch University and Tygerberg Academic Hospital, Cape Town, South Africa
2Department of Medicine, Stellenbosch University and Tygerberg hospital
3Division of Nephrology, Department of Medicine, Stellenbosch University and Tygerberg Hospital
*Corresponding Author: Amani Kaawan, Division of Rheumatology, Tygerberg Academic Hospital, National Health Laboratory Services. Faculty of Health Sciences, Stellenbosch University and Tygerberg Academic Hospital, Cape Town, South Africa.
Citation: Amani Kaawan., Mou Manie., Adel M Aboshakwa., Razeen Davids.,(2020) MMED PROJECT The Clinical Profile of Takayasu Disease at Tygerberg Academic Hospital – a retrospective study. J. Clinical Cardiology and Cardiovascular Interventions, 3(11); Doi:10.31579/2641-0419/103
Copyright: © 2020 Amani Kaawan, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 02 November 2020 | Accepted: 12 November 2020 | Published: 19 November 2020
Keywords: Takayasu’s arteritis
Takayasu’s arteritis (TA) is a disease of unknown etiology that causes chronic inflammation of the large blood vessels and usually involves the aorta and its branches. The inflammatory process initially leads to thickening of the arterial wall and may result in stenosis, occlusion, dilatation or aneurysm formation. Although TA occurs more commonly in certain regions such as Asia, it is a global disease. Currently, there is a dearth of information on this condition in African countries, including South Africa.
Results: We have identified 50 patients meeting the ACR criteria for the diagnosis of TA. Data was drawn from the records of the Division of Rheumatology as well as the angiographic records of TA. This included patient demographics, mode of presentation, classification, co-morbidities, complications, clinical and laboratory features, radiological findings, drug therapy as well as outcomes. The cohort comprised 34 of mixed race, 12 black and 4 white patients. The mean age at diagnosis was 16-56 (28.2) years. The most common presention was hypertension, followed by CVA, heart failure, and syncope. Angiography revealed Type V (most of aorta) and Type I (aortic arch branches) lesions to be the most common and that stenosis was much more common than aneurysm formation. Two patients had concomitant antiphospholipid syndrome. Another two had concomitant internal jugular vein thrombosis. Six patients had significant mediastinal lymphadenopathy, only one of whom had TB.
Corticosteroids and additional immunosuppressive therapy were used to control disease activity in most patients. Biological treatment was used in two patients. Surgical intervention consisted mainly of renal auto transplantation. Twelve percent of patients had repeated admissions, which included planned surgical intervention. We had two mortalities, both as a result of massive strokes. The mortality rate was 6%. Only 3 patients had active TB.
Conclusion: The study revealed gender and age characteristics similar to previous studies, confirming that TA affects mainly young females. The mortality rate of 6% in this cohort is significantly lower than that of previous series. The unusual findings in this study were:
Significant chest lymphadenopathy in 12% of the cases,the significantly lower percentage of active TB of only 6%, two cases of a rare finding of venous thrombosis as well as 2 cases of an uncommon finding in TA of antiphospholipid syndrome.
The diagnosis of TA may be difficult because of the non-specific nature of the illness in the early stages. Furthermore, TA exhibits different patterns of arterial involvement, disease expression and prognosis in different regions of the world. [1] The clinical presentation results from the arterial lesions and the systemic inflammatory response. At disease presentation or during relapses, TA patients may present with non-specific complaints such as fever, malaise, anorexia, weight loss, myalgia or arthralgia. [2] As arterial lesions progress, more characteristic features of TA may be found such as limb claudication, decreased or absent peripheral pulses, vascular bruits, hypertension and discrepancies in blood pressure between arms due to stenotic or occlusive lesions. [1] In severe cases, this may result in serious complications such as myocardial infarction, stroke and blindness. [3]
Imaging modalities are central to establishing the diagnosis of TA, determining the distribution of lesions and monitoring disease activity. [3] Conventional radiographic angiography [digital subtraction angiography (DSA)] is considered as the gold standard for the diagnosis of TA. However, it is invasive, poses some radiation risk and currently, has largely been replaced by computerized tomography angiography (CTA). Other non-invasive imaging methods including magnetic resonance angiography (MRA), color Doppler ultrasound (CDU), PET with 18F-fluorodeoxyglucose (18F-FDG) and 18F-FDG PET/CT have recently gained ground. In a study conducted in 2004, it was shown that non-invasive imaging methods, deoxyglucose positron emission tomography (PET) and magnetic resonance imaging (MRI)) provided important additional information about disease activity and progression of vessel wall thickening when compared with X ray angiography. [4]A meta-analysis done to assess the diagnostic value of 18-FDG-PET in estimating disease activity in TA concluded that 18-FDG-PET had moderate diagnosis value in assessing TA activity and may add additional value to the current diagnosis methods. [5]
The goal of treatment are to stop the acute inflammatory process and prevent further damage to the vessel wall. The mainstay of therapy is glucocorticoids (usually prednisone); however, other medications include cytotoxic drugs, such as methotrexate, which are often used to help control the disease and reduce the need for prednisone. Newer agents include mycophenolate leflunomide and biologics such as TNF alpha blockers (infliximab, etanercept), tocilizumab, abatacept and rituximab are also increasingly being used for treatment of resistant cases. [3] Treatment of symptomatic fibrotic lesions (stenosis or occlusions) requires either vascular interventional or surgical therapy. This can be achieved by angioplasty with or without stenting or in severe cases, by vascular resection and surgical interventions.
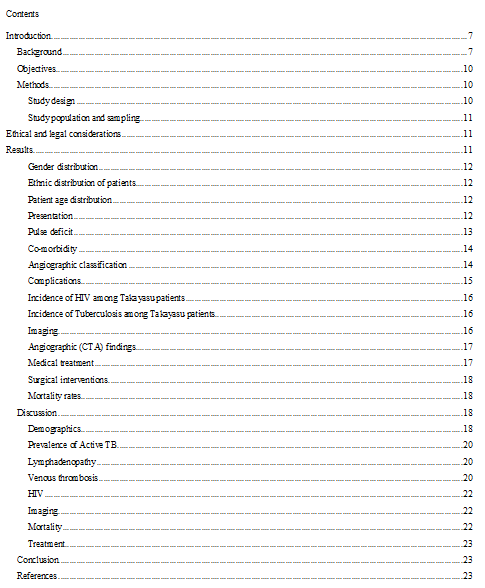
As shown in (table 1), currently there is a paucity of data on TA from the African continent including South Africa. A literature search has revealed only 3 publications on TA from South Africa. One important study was conducted at the Groote Schuur Hospital (GSH) in Cape Town (South Africa). [21] The study reported on 272 patients over a fifty-year period (1952-2002). Patients had a mean age of twenty-five years, of which 75% were female and comprised predominantly mixed race (68%).Some limitations of the study included a lack of information on non-vascular symptoms, the use of outdated imaging techniques, older treatment regimens as well as lack of information on co-morbidities such as HIV, diabetes and atherosclerosis. Additionally, the study reported the use of anti-TB therapy without definite confirmation of the TB diagnosis in some of the cases. Another study reporting on paediatric cases in Gauteng (South Africa) was conducted over a period of fifteen years and included thirty-one patients with a higher prevalence of TA among black patients. [3] This particular study was conducted at the Baragwanath Hospital (Johannesburg, South Africa). [3] The third study was conducted at the King Edward VIII Hospital in Durban (South Africa) and was a small series (11 patients) reporting mainly on the morphological and radiographic features of TA. [3]
A publication from Tunisia in 2010 reported on 27 patients with a mean age of diagnosis was 33 years and 88.9% were females. [3] A second Tunisian study included a limited number of 11 females and was conducted over a 12 year period, wherein the mean age at the time of diagnosis was 29.1 years. .[3] Furthermore, other published studies from the African continent was from Morocco with 47 patients.. [3]
Studies from other regions in the world revealed comparable data. A Turkish study included 248 patients from fifteen different rheumatology centres. Results indicated that the mean age was 40 years and the majority (228 out of 248) were females. [3] These findings are supported by a Brazilian study (Sao Paulo) wherein data was collected from three different public universities (UNIFESP, USP, UNICAMP). Seventy-three patients were recruited and showed a mean age of 27 years, with a predominantly female gender. [4]
In terms of its association with TB, tuberculosis has remained an important differential and possible etiological factor. However, tuberculous aortitis tends to cause erosion of the vessel wall with the formation of true or false aneurysms, particularly affecting the descending thoracic and abdominal aorta. Dissection and rupture are important complications rather than the stenosis typical of Takayasu arteritis. The incidence of rupture and bleeding complications of aneurysmal Takayasu arteritis is low. previous studies reported that the association ranged from 5.0 % to 48.0% . However, there was also a lack of information on whether the TB was active or not and, in some cases, the diagnosis of TB appeared questionable. The question of an association of TA with HIV has also not been addressed in previous studies from this region, even though HIV is known to cause thrombosis of large vessels. Information and previous reports on other features of the disease also appear scarce, with special reference to the systemic features such as fever, malaise, lymphadenopathy, weight loss, skin rash, synovitis and anemia.
Studies relating to the main affected arteries of TA in this country is limited. In terms of the most common subtype of TA in South Africa, reports appear varied due to the different demographic profile and regional differences. There is also very limited information on the use of the latest imaging techniques employed for the diagnosis of TA, the treatment regimes, responses and adverse effects to treatment.
Lastly, complications such as arterial aneurysm rupture, angioplasty and surgical bypass of vascular occlusive lesions which require surgical intervention have not been reported on in any significant detail in previous studies. It should be noted that indications for surgery such as revascularization have also been changed over the last few years.
This study attempts to shed light on some of the unresolved areas referred to above.
Objectives
The aims of the study were to determine and describe:
-demographics such as age, gender and race;
-prevalence of TA in the South African region;
-the type of association with active or previous TB or HIV;
- the presenting features and the prevalence and of other co-morbidities in TA patients;
-the affected arteries in TA patients;
-the imaging techniques employed for TA diagnosis;
-the treatment regimes, responses and outcomes treatment;
Methods
Study design
The current study was done at Tygerberg Academic Hospital, a tertiary referral center situated in the city of Cape Town (Western Cape Province, South Africa). Tygerberg Academic Hospital provides a tertiary service to a population of approximately 1.5 million people (the TBH drainage area). Most of the patients who visit the hospital are indigent and are of mixed-race ethnicity.
This was a retrospective observational study, conducted at the Division of Rheumatology at this hospital. Case records of patients with TA meeting the 1997 American College of Rheumatology (ACR) classification criteria were reviewed. Data collected were TA patient demographics, presentations, classification, co-morbidities, complications, clinical and laboratory features, radiological findings, drug therapy and outcomes. Data was accessed from the administrative databases of the Division of Rheumatology at Tygerberg Academic Hospital, allowing the investigator to review the in-patient and out-patient records of the TA patients.
The inclusion criteria were the positive diagnosis of TA according to ACR criteria, which requires that at least three of the six criteria are met (see Table 2 below). [2]

Ethical and legal considerations
The study was approved by the Ethics Committee of the Faculty of Health Sciences of the University of Stellenbosch (project number (S18/09/183) and the Research Committee of the Department of Medicine, Tygerberg Academic Hospital. The study was conducted in accordance to the Helsinki Declaration as well as MRC and ICH guidelines.
The names of the participants were not mentioned in the output of the research. Where the investigator only had access to the collected data in order to ensure the confidentiality and integrity of the data.
A total of 50 patients with Takayasu arteritis (TA) were identified.
Females represented the majority (82.35% n=42) of patients.
Approximately, a third of the population were of mixed ethnicity (68% n=34), almost a quarter (24% n=12) indicated were of black ethnicity and a smaller percentage of patients indicated white ethnicity.

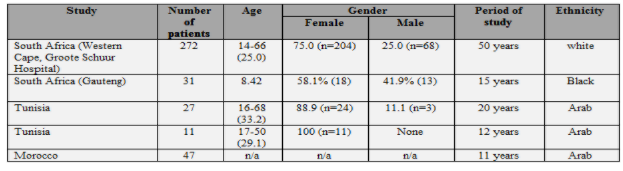
Almost half of the patients (44% n=22) were between the ages of 26-35 years, followed by less than a third (31% n=17) who were between the ages of 16-25 years. Only seven patients (14.0% n=7) belonged to the 36-45 years age group and four patients (8.0% n=4) were in the age group of 46 and over.
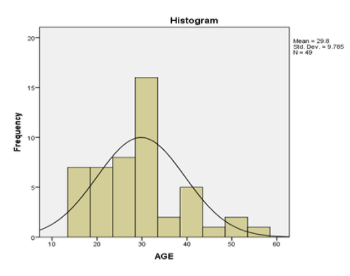
As shown in table (3), half of the patients (50% n=25) had hypertension (HPT) in their presentation, followed by eleven patients (24.0% n=12) who presented with cerebrovascular accident (CVA). One patient had both hypertension and CVA, and five patients (10.0% n=5) presented with heart failure (HF).
The above Table refers to the main methods of presentation, some patients had more than one presenting feature which represent 5 patient (10%) of total cohort. Of the three patients who presented with syncope, one had loss of vision; whereas one patient presented with constitutional symptoms and erythema nodosum. In the group of patients who presented with hypertension, one also had abdominal pain and BP discrepancy and another one had dry gangrene of the lower limb. Another patient also presented with lymphadenopathy. In the CVA group, one patient also had left side paresthesia and one patient also had palpitations.
Of two patients in whom we could not identify the mode of presentation, one of them was diagnosed at age of two years with no clear documentation of his presentation and the other had incomplete documentation.Significant lymphadenopathy was found in six patients (12% n=6) which refers to “pathological” lymph nodes of 2 cm or more, particularly in the hilar or mediastinal region. The regions in the chest where the lymph node was found were: mediastinal in one patient, hilar in another patient, one pretreacheal and two patients were subcarinal with cervical lymph nodes. Supraclavicular and pretreacheal and perivascular (scattered) lymph nodes - on PET scan was detected in one patient. Three patients had RVD tests all of which were negative, and three patients had transbronchial lymph node biopsies all of which were negative for TB. Only one patient showed evidence of TB (on bronchial washing).
As shown in the table below, the majority (72%) of our cohort had pulse deficits, and most of them involved the radial artery: on the right side (36.1%) and on the left side in (61.1%).
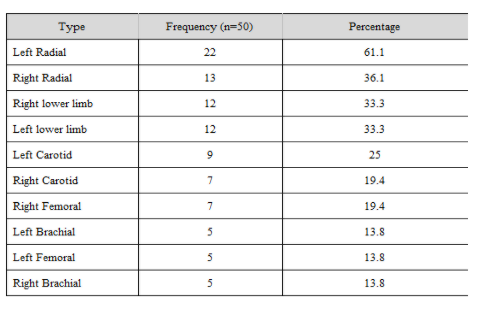
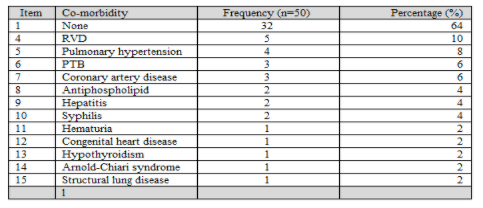
Table 5 shows the presence of co-morbidity in the cohort group. The majority of patients (66% n=32) had no co-morbidity.
There were 3 cases of active proven pulmonary tuberculosis (PTB) (6% n=3), two of whom were diagnosed on sputum testing and a third from bronchial washings. pulmonary hypertension was present in four patients. One patient had documented chronic thromboembolism and two had DCMO. The fourth patient had hypertensive heart disease.
One patient had interstitial lung disease but did not have pulmonary hypertension. Two patients had antiphospholipid antibody syndrome (APS), one of which had left carotid thrombosis and other one had cerebrovascular disease (2 strokes).
Five patients had retroviral disease (RVD). Two patients had chronic Hepatitis B, one patient had Arnold Chiari type1 with no syrinx; one patient had congenital heart disease; one patient had hypothyroidism, one had ureteric fistula, one patient had persistent haematuria (of unknown cause) and two patients had secondary syphilis.
In the current study, the new classification for TA was used as shown in Figure 2 below.
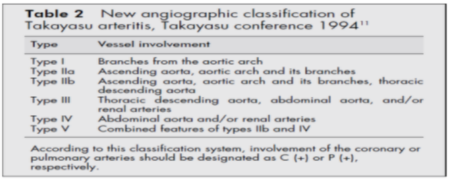
In our cohort, the majority of patients met Type V (38% n=19) of the ACR criteria. Type I was found in nine patients (18% n=9), Type III was found in seven patients (14% n=7), Type IIa and IIb were found in two patients, respectively.
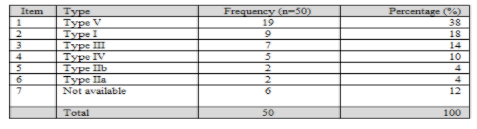
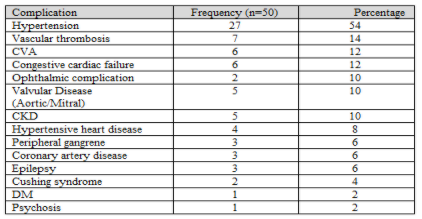
Table 9 shows complications related to disease and treatment. The majority of patients had HPT (54% n=27) which includes the earlier manifestation and subsequent complication with six patients reporting CVA (12% n=6).
Left Heart Failure was present in 6 patients. In four of these patients, this was assessed as being the result of severe hypertension and the other two was labeled “idiopathic”.
Three of the patients of our total cohort suffered a stroke subsequently .Chronic kidney disease was present in 5 patients (10%) and was thought to be mainly due to bilateral renal artery stenosis and severe hypertension.
Complication which occurred in 2 patients included optic nerve atrophy and glaucoma in another case. Valvular heart complications were present in 5 cases (10%) in the form of mitral regurgitation in two patients and aortic regurgitation in another 3 patients.
The vascular complications (arterial or venous thrombosis) occurred in seven patients (14% n=7). Pulmonary embolism was found in two patients with no obvious underlying venous thrombosis. Two of the patients had jugular vein thrombosis and the remaining were arterial in nature. Two patients had thromboembolic to the coronary vessels one had an intramural thrombus in the left ventricle (patient with DCMO).
Chronic kidney disease was found in (10%) of our patients where latest creatinine ranged from 140-180 umol/L.
Three patients (6% n=3) had coronary artery disease (CAD), the aetiology of which may be multifactorial. As mentioned, two patients had thromboemboli from the left ventricle and a third had diffuse atherosclerotic disease. A similar percentage of (6% n=3) was preset in patients who had peripheral vascular ischemia with evidence of gangrene in lower limbs and in the mesenteric vasculature. Steroid induced Cushing syndrome was present in two patients (4% n=2).
A total of 34 patients were tested for HIV (68%) in our cohort. Almost 15% (14.7%) of the patients who were tested were positive, thus the majority (85%) of the patients who were tested were negative.
Among our cohort, 20 patients (40%) were tested for TB. The majority (85%) of the tested population were negative, while 3 patients (15%) tested positive. It is important to note TB testing was based on clinical suspicion.
The majority (88% n=44) of the patients in this cohort had CTA and PET SCAN (88% n=44) each. PET SCAN is sometimes repeated as a follow up in detecting evidence of disease flare - 39 patients had both CTA and PET and 4 had only CTA). Half of patients (50% n=25) had Doppler, which is usually used as the initial diagnostic tool to confirm vasculature abnormality. In this cohort study, Doppler was frequently used in (50%) of patient to assess the renal and carotids. Only ten patients (20% n=10) had an MRI.

Angiographic (CTA) findings
The majority (58%) had stenosis, followed by stenosis and aneurysm in (32%) as shown in the table below.


Different types of options for treatment are available to TA patients depending on the course of the disease. The majority of patients (60% n=30) were treated with a combination of treatments including methotrexate or azathioprine with steroids.
Ten patients (20%) reported not being on treatment, due to “burnt-out” disease or patients did not have active disease at the time. Two patients received biologics; one received (Infliximab) and the other received tocilizumab.
Four patients (8% n=4) were treated with steroids only (Prednisone).
The efficacy of each treatment was not included in our study

Surgical interventions
Some patients had surgical intervention to treat complications arising from the disease. Twelve patients (24% n=12) had renal surgical intervention which included four of them undergoing autotransplantation. Five patients had renal artery graft, two patients had nephrectomy and one had kidney transplant. Furthermore, five patients (10% n=5) had aortic complications requiring surgical intervention, which included repair of AAA and arch of the aorta. Lastly, one patient case required repair of root of the aorta, which included aortic valve replacement. Two of patients required amputation, one had one toe amputated and the other two left fingers amputated.

Two patients (4%) died which both as a result of massive strokes.
Demographics
In terms of age distribution, our findings report a mean age of 28.2 years (16-56) years which is consistent with the Brazilian study (27 years) [19], the one Tunisian study (29.1) [15] and Groote Schuur series (25 years). [4] Higher mean ages were noted in the other Tunisian study (33.2 years) [16] and Turkish series (40 years). [18] In terms of ethnic distribution, our findings show that TA was predominantly found among the mixed-race group, which is similar to that of the GSH study. [21] The reason is that the Western Cape has a predominantly mixed-race population which explains the difference to the Gauteng series, where the majority of the population are of African ethnicity (black). [12] Gender distribution in this study among TA patients is supported by similar studies confirming the predominant female involvement (82%) and is consistent with other series by GSH (75%) [21], Turkish study (91.9%) [18], Tunisian study (88.9%) [15] and the Brazilian study [19]
Hypertension
Hypertension was the most common presentation in TA patients. Over half of patients in this series (54%) presented with hypertension and is consistent with the with GSH series (77%) [21], Turkish series (43%) [18] and Greek series (78.0%). [4] The pathogenesis of the hypertension is postulated as being due to renal artery stenosis in most cases or “coarctation of the aorta” in other cases. It should be noted that the majority of the patients had category Type V (38%) which affects the ascending aorta, aortic arch and its branches, and thoracic descending aorta as well as abdominal aorta and/or renal artery.
Theoretically, patients with TA have suppressed immunity. This is thought to be due to the immune mediated nature of the disease as well as the treatment with steroids and other immunosuppressive therapy.
In our cohort, 10% of our patients tested positive for TB. However, although all patients were subjected to an appropriate history-taking and had a chest radiograph, extensive testing for TB was not conducted on those patients assessed as not likely to have TB. Thus, the TB status of the majority (60%) was not known. Definitive exclusion of TB was also not conducted in other studies. However, a low prevalence of TB of only 6% (n=3) is unexpectedly lower in comparison to other studies. This is of particular significance considering the fact that patients in our cohort hail from a predominantly poor and disadvantaged communities where there is a pandemic of TB.
A more direct comparison can be made to the GSH study where the proportion of TA patients diagnosed with TB was as high as 20%. [21] A potential problem with the diagnosis of TB in this series was that a strongly positive Mantoux was also regarded as evidence of “active” TB. Currently routine Mantoux screening as evidence of TB is not the norm. In terms of TB prevalence, the Korean series reported prevalence of 17%, Turkish series (6.4%) [1] and the Brazilian study 41.0%.[19] Generally a high percentage of TB (up to 90%) has been reported in pediatric series including the South African study.
Although lymphadenopathy is a well-documented finding in patients with TA, the presence of large mediastinal nodes mimicking TB is rare. Current literature reports isolated cases of “massive” lymphadenopathy mimicking TB. In our cohort, six patients (12% n=6) had significant lymphadenopathy. In these cases; however, it is mandatory to exclude TB. Although one patient clearly had TB, evidence of TB for the remainder of the population was not available. It may be suggested that previous cases of severe lymphadenopathy due to TA, may have been regarded as being due to TB and in some cases, were subjected to anti-TB treatment. This is the first study that documents significant lymphadenopathy in 10% of the cases of TA.
Two patients in this study had internal jugular vein thrombosis and two had the CTA proven pulmonary embolism. However, there was no obvious site of venous thrombosis evident in the patients with pulmonary embolism. As TA is a disease affecting large arteries, venous thrombosis did not form part of the clinical features of this condition. Internal jugular vein thrombosis is also very rare, but 2 cases were evidenced in our cohort. Furthermore, isolated case reports relating to venous thrombosis and one reporting on internal jugular vein thrombosis have been noted. [5]
Two female patients of our cohort had antiphospholipid syndrome increasing the risk of venous and arterial thrombosis. The rarity is clear because the literature search revealed the association of TA with antiphospholipid syndrome as 2 case reports, one from Korea in which an elderly female was affected [5], and in the other a young Japanese man (17 years old). [6]
Cardiomyopathy:
Although 6 patients presented with heart failure, two of the cases did not have a clear cause such as severe hypertension or ischaemic heart disease. We feel that it is reasonable to assume that these cases were due to the rare entity of TA associated cardiomyopathy. Furthermore, there was no data exploring this topic, only a case report of TA presented with heart failure. [6]
In this study only 34 of the 50 patients were tested for HIV. HIV testing was not routinely done but reserved for those with underlying clinical suspicion of this condition. Thus, just under 15% of those tested were positive for HIV making it very difficult to draw any meaningful conclusions on the effect of this condition. From the limited numbers who were HIV positive, it does not appear that this condition presented differently in this sub group.
In our patients the commonest vessel affected was the subclavian artery (42%) and is consistent the Gauteng pediatric study (52.2%) and the Tunisian series. In the GSH series, 70% involved the entire aorta. [21] Our study showed that most TA patients had Type V (32%), which mirrors the findings of the Brazilian series (52%). [19]
CT angiogram has been and remains the imaging method of choice for the diagnosis of TA. Most of the patients had Type V disease, which was also the case in the GSH study. PET CT scanning has been shown to be a good adjunctive method of imaging in cases where there may be uncertainty on whether there is active vasculitis in the patient or not. The radiographic findings characteristic on CTA, namely stenosis and aneurysm formation, do not necessarily imply active disease. In this study, 80% of the patients had PET-CT scanning done, some of whom had more than one. This number is much larger than that which have reported previously and it appears that this may become a routine part of the follow up if there is a need to determine “active” TA.
In this study only 2 patients (4%) died. This represents a low mortality compared to previous reports and is a much lower than the mortality than that reported from the GSH of 20%.[21] This may reflect earlier and improved diagnosis of milder cases which may have been missed in the past or, may be due to alternative therapies which were not available previously (see below). [17]
Largely because of limitation of state resources, only two patients received biologic therapy. One patient received infliximab and the other patient received infliximab which caused reactivation of TB. She subsequently received tocilizumab and is currently still on this treatment.
Conclusion
In summary this study revealed gender and age characteristics similar to previous studies, confirming that TA affects mainly young females. The mortality rate of 6% in this cohort is significantly lower than that reported in previous series.
Some of the unexpected findings in this study was the significantly lower percentage of active TB. This study also revealed 6 cases of “massive” chest lymphadenopathy only one of which was due to TB. It may well be that some of the TB cases reported in previous studies may have been over-diagnosed.
This study also revealed two (2) unusual cases of venous thrombosis - supporting isolated previous reports of venous thrombosis.
Another previously documented but rare finding in TA was that there were 2 cases of cardiomyopathy in our cohort.
A prospective study involving larger numbers from different institutions may shed some light on these intriguing findings.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
