
Research Article | DOI: https://doi.org/10.31579/2641-0419/506
*Corresponding Author: L. Baciulescu, Cardiologie, Centre Hospitalier Agen-Nérac (site d’Agen), Agen, France.
Citation: L. Baciulescu, (2025), Mitral valve prolapse and long QT interval: the missing link explaining sudden cardiac death in these patients?, J Clinical Cardiology and Cardiovascular Interventions, 8(15); DOI:10.31579/2641-0419/506
Copyright: © 2025, L. Baciulescu. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 07 August 2025 | Accepted: 03 November 2025 | Published: 12 November 2025
Keywords: mitral valve prolapse (MVP); ventricular tachycardia (VT); ventricular fibrillation (VF)
Introduction: Mitral valve prolapse (MVP) is associated with ventricular tachycardia (VT), ventricular fibrillation (VF) and sudden cardiac death (SCD). It is considered that SCD requires a substrate, a trigger, and a modifying risk factor, but not all patients with MP-related SCD/VT/FV have a substrate (fibrosis or severe mitral regurgitation -MR or mitral annular disjunction -MAD).
Objective: This case presentation suggests that the missing link explaining SCD in some patients with MVP is a significant variability of the QTc interval with a pathological prolonged QT interval preceding MP-related SCD/VT/FV. Subclinical inflammation could be the substrate.
Method: I present to you the case of a patient aged 72 with MVP, severe MR and a NSTEMI (sub occlusion of the distal right coronary) who was implanted with a subcutaneous defibrillator (S-ICD) after an aborted sudden cardiac arrest, followed by repeated arrhythmic events (AE) in the next weeks, despite revascularisation. The ECG performed in the intensive care unit showed a prolonged QTI of 531ms. A cardiac MRI was performed, finding a preserved left ventricular ejection fraction (LVEF) with infero-septal hypoperfusion without evidence of necrosis or inflammation. Because of the multiples complications during and after the initial hospitalization, a Mitra Clip procedure was performed at distance. The echocardiography post intervention showed a mild residual MR and normal LVEF. After the intervention, the betablockers were stopped because of a tendency to mild bradycardia but two weeks later, the patient was re hospitalised for traumatic syncope. The first ECG found a long QTI (500ms) but the followings showed an important QTc interval variability, with sometimes normal values and frequent ectopy. The patient’s blood tests were completely normal. The consultation of the S-ICD showed a good functioning and one VF preceded by prolonged QTI. During the hospitalisation, the patient presented another syncope due to a new FV (figure 1) despite the absence of any acute trigger. There is a long QTI (not standardized measurement on S-ICD tracings but QTI longer than half of the RR space) preceding the VF. The diagnosis of an associated congenital long QT syndrome (LQTS) was ruled out. After the resumption of beta-blockers, the patient no longer presented with sustained arrhythmias.
Results: This patient with MVP presented multiple AE (VF), each one preceded by a prolonged QT interval, in the absence of congenital LQTS, probably related to subclinical inflammation.
Conclusion: Is there a significant QTc interval variability, with the appearance of a long QTI preceding malignant arrhythmias in all patients with MVP? Should we treat MVP like LQTS and avoid any drug or situation that could prolong the QTI?
Mitral valve prolapse (MVP) is a common valvular heart disease with 2-3% prevalence. Arrhythmogenic bileaflet MVP (ABiMVPS) syndrome was described with female predominance. The annual rate of sudden cardiac death in MVP is double the general population at 0.2-0.4%/year. The coexistence of ABiMVPS and congenital long QT syndrome (LQTS) is rare but malignant.
Mitral valve prolapse is associated with ventricular tachycardia (VT), ventricular fibrillation (VF) and sudden cardiac death (SCD). The risk of SCD is specific for the MVP substrate and independent of mitral regurgitation (MR) severity (80% of SCD occur in patients with moderate mitral regurgitation).
High risk features include complex ventricular ectopy (couplets, triplets, pleiomorphic VC), T wave inversion in the inferior leads, mitral annular disjunction – MAD (detachment of the ‘roots’ of the annulus from the ventricular myocardium causing myocardial stretch), myocardial fibrosis seen at cardiac MRI (papillary muscle/ infero basal LV), high lateral annular velocities with spiked configuration due to mechanical traction -the Pickelhaube sign ( peak systolic lateral velocity of the lateral mitral annulus >1.6 m/s), low ejection fraction, impaired global longitudinal strain, greater mechanical dispersion, double peak strain, which can all be identified with common imaging modalities.
Bi-leaflet prolapse, ≥ moderate mitral regurgitation and female gender are also associated with greater risk of SCD.
Furthermore, there is evidence of increased sympathetic activity, coupled with decreased vagal activity and elevated catecholamine levels in MVP patients with a high ventricular arrhythmic load. This autonomic dysfunction not only increases the frequency of ectopic activity but also predisposes the ventricular myocardium to ectopic activity.
Severe mitral regurgitation may be responsible for the high mechanical traction and stretch that can induce complex ventricular ectopy due to triggered activity even in the absence of intramyocardial fibrosis.
MAD is not always present in patients who have MVP and it can be found in patients without MVP. In a Norwegian study which enrolled 116 patients with MAD, 34% of them presented with severe VT. This study supported that papillary muscle fibrosis may be linked to severe arrhythmic events and showed an association among PVCs, arrhythmic events and MAD independently of the presence of MVP, indicating that MAD itself may be an arrhythmogenic entity. However, more studies are needed to prove and better define this.
The mechanism of SCD in MVP is not completely elucidated. It is considered that SCD requires a substrate, a trigger, and a modifying risk factor, but not all patients with MVP-related SCD/VT/FV have fibrosis or severe mitral regurgitation. Subclinical inflammation and a prolonged QT interval may be the missing link in these patients.
The objective of this case presentation is to demonstrate that there is a significant variability of the QTc interval and that a pathological prolonged QT interval precedes multiples episodes of VT/VF and SCD in a female patient with idiopathic bi leaflet MVP.
I present to you the case of a patient aged 72 with mitral bi-leaflet prolapse, severe mitral regurgitation and a non-ST elevation myocardial infarction (sub occlusion of the distal right coronary artery) who was hospitalised in the intensive care unit after an aborted sudden cardiac arrest, followed by repeated and frequent arrhythmic events (VT and VF in the next weeks, necessitating multiples external electrical shocks, despite revascularisation).
The patient’s medical history: substituted central hypothyroidism, breast surgery for lobular carcinoma in situ, sudden death of her father at the age of 64 (myocardial infarction).
The ECG done in the intensive care unit shows a prolonged QT interval of 531ms (figure 1). Beta blockers and magnesium were administrated with shortening of the QT interval, which remains pathological during the hospitalisation in the ICU (figure 2).
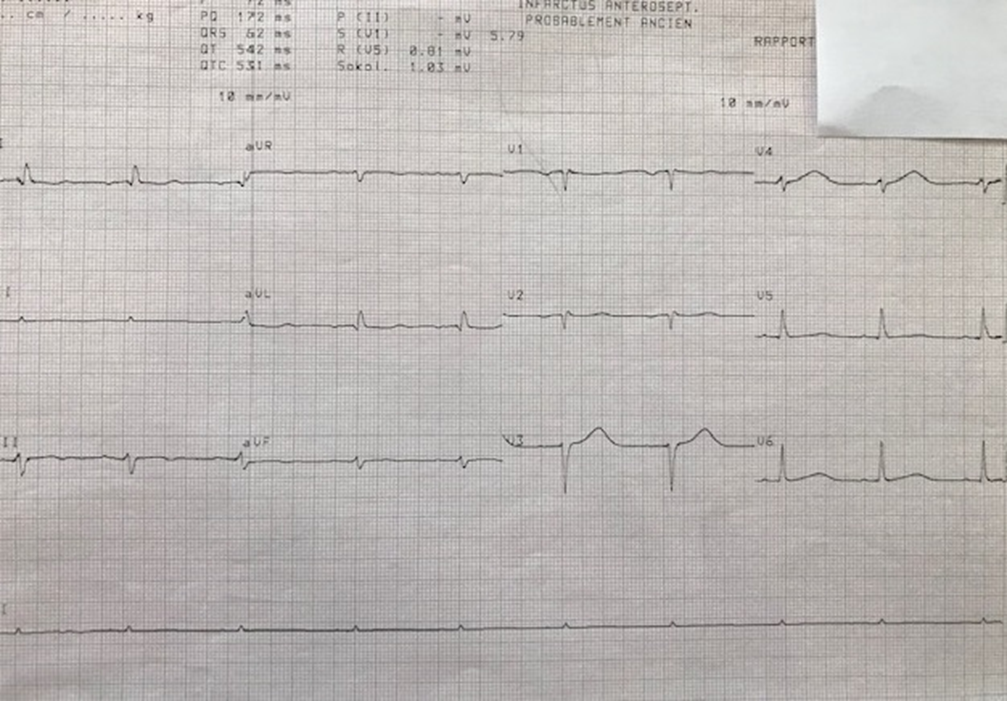
Figure 1
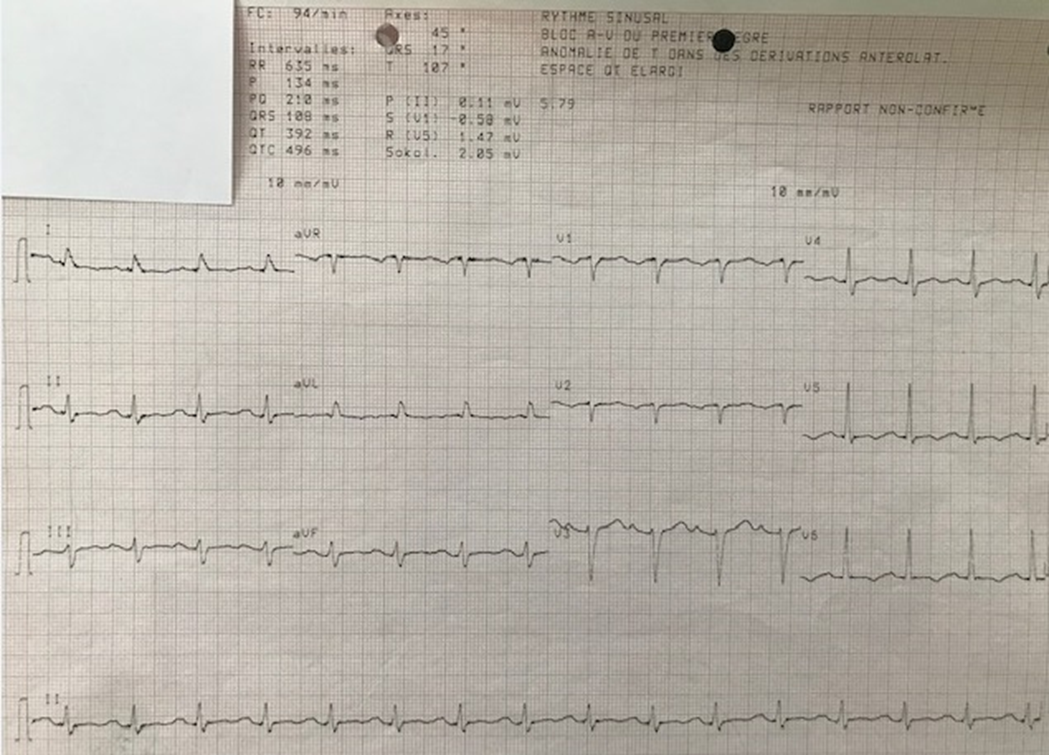
Figure 2
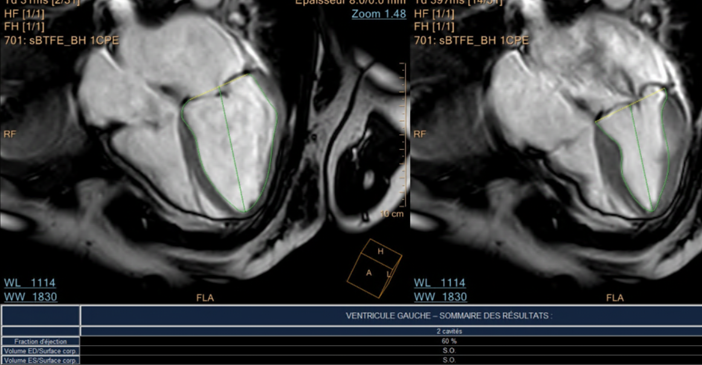
A cardiac MRI was performed, finding a preserved left ventricular ejection fraction with infero-septal hypoperfusion without evidence of necrosis in the viability sequences; high-grade mitral regurgitation is confirmed; no abnormality suggestive of myocarditis were found.



The patient had multiple complications during and after the hospitalization in the intensive care unit (ICU): sepsis due to lung infection, pulmonary embolism and atrial fibrillation, so the heart team decided that a MITRA CLIP procedure was the best option (because of the high operative risk of the mitral valvuloplasty). The patient was implanted with a subcutaneous defibrillator (S-ICD) and the Mitra Clip intervention was performed 7 months later.
The echocardiography post intervention showed a good result: mild residual mitral regurgitation after the positioning of two mitral clips, normal ejection fraction.
After this intervention, the betablockers were stopped because of a tendency to mild bradycardia. Two to three weeks after the MITRA CLIP intervention, the patient was hospitalised for syncope with cranial trauma.
The initial ECG found a sinus rhythm, first-degree AV block with left atrial hypertrophy (PR 230ms), an anterior left hemiblock, a long QT (500ms), premature ventricular complexes (PVC) as shown in figure 3:
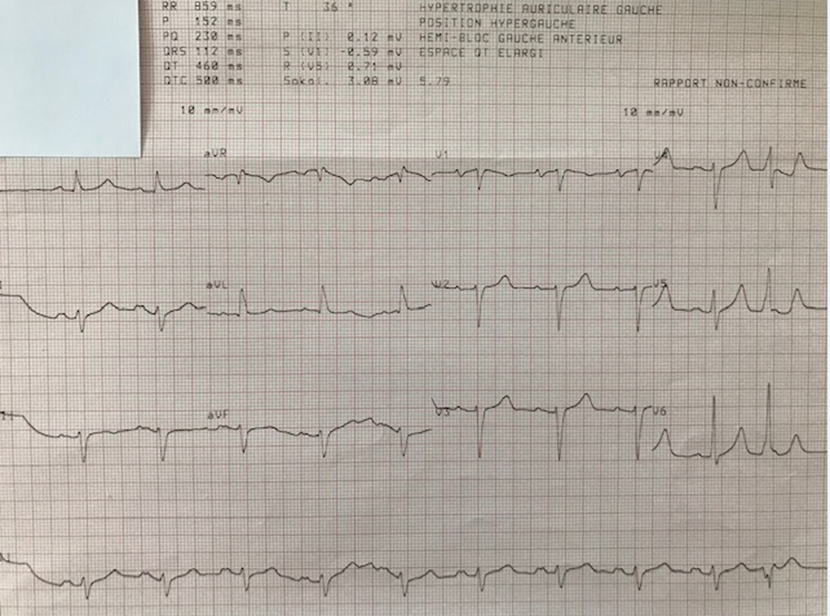
Figure: 3
The interrogation of the S-ICD found one arrhythmic event (appropriate electrical shock for VF) preceded by prolonged QT interval (figure 4)
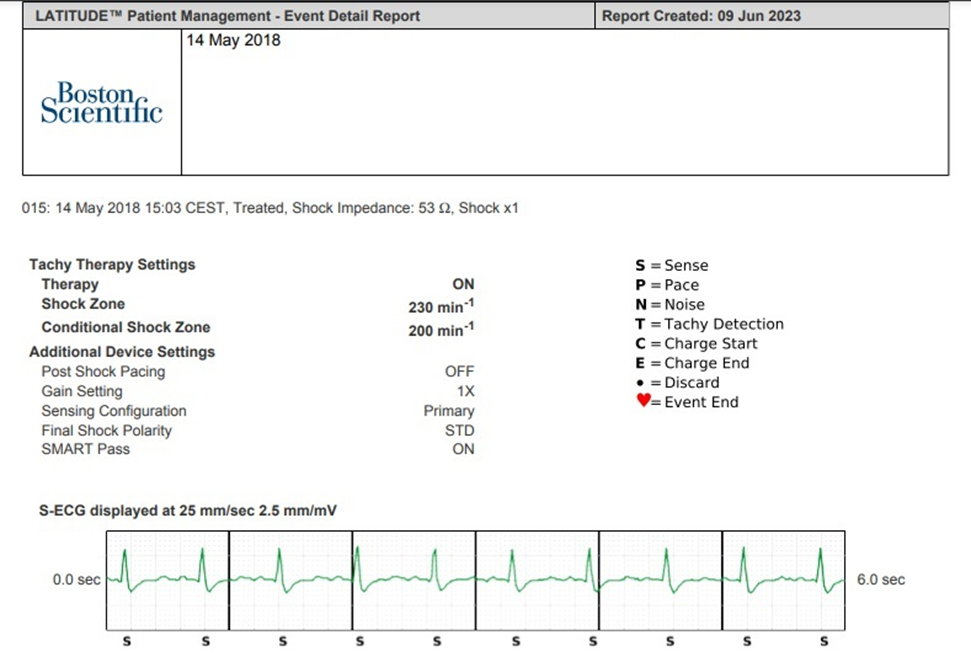
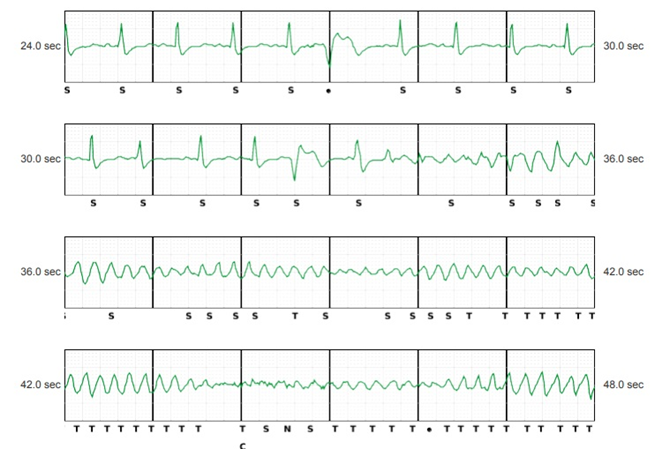
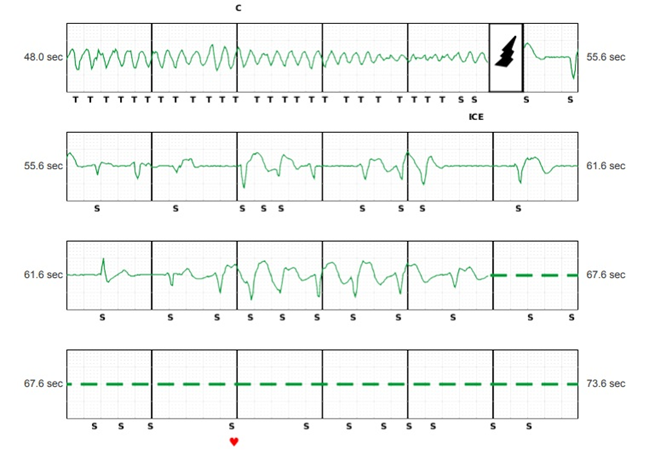
Figure: 5
The patient’s blood tests were completely normal, especially troponins, brain natriuretic peptide, potassium, calcium, and magnesium, TSH.
The ECGs showed an important QTc interval variability, with sometimes values considered normal for women (453ms) and frequent premature polymorphic ventricular complexes (figure 5).
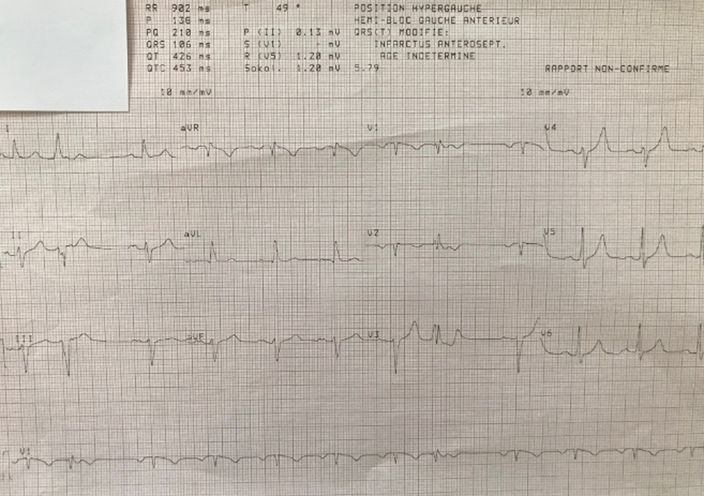
Figure: 5
During the hospitalisation, the patient presented another syncope due to a new arrhythmic event despite the absence of any acute trigger (no infection, no ischemia, no electrolyte abnormalities or hormonal imbalance, no QT-prolonging drugs etc) except probably the subclinical inflammation due to the recent Mitra clip intervention (figure 6).
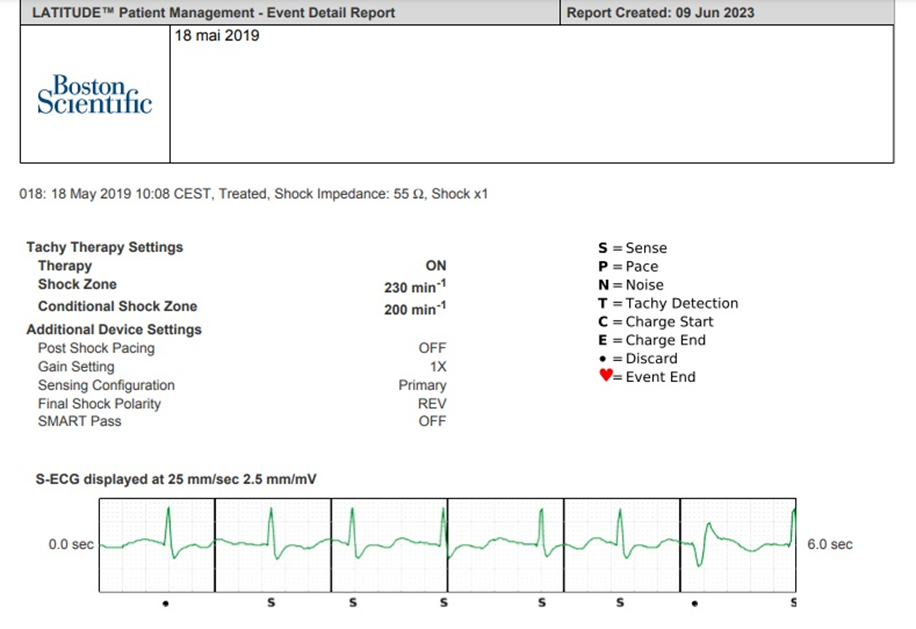
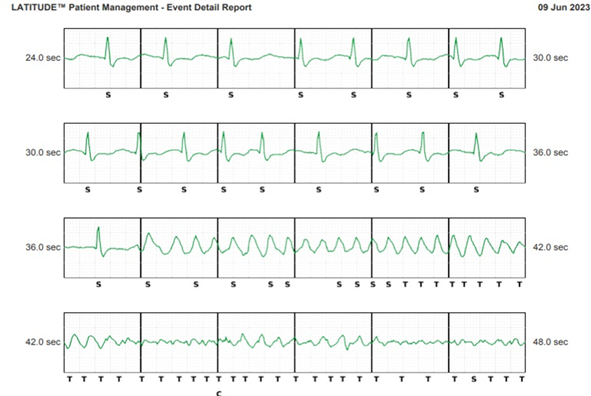
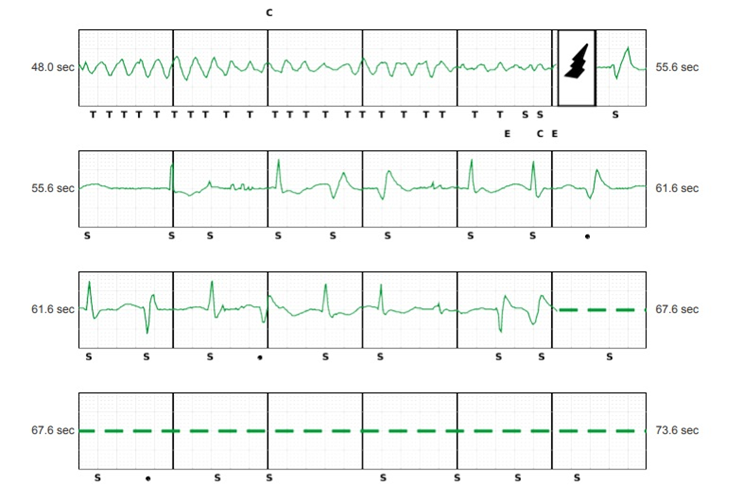
There is an elongated QT interval (not standardized measurement on S-ICD tracings but QT interval longer than half of the RR space) and we can see a PVC that falls on a T wave resulting in ventricular fibrillation. An appropriate choc was delivered by the S-ICD.
The betablockers were reintroduced slowly followed by complete stabilisation of the patient.
The diagnosis of an associated congenital long QT syndrome was ruled out by the heart team after preceding to specific tests, but genetic testing was not done.
After the resumption of beta-blockers, the patient no longer presented with sustained arrhythmias (a 7-year period of follow-up), despite the recurrence of severe mitral regurgitation requiring surgical revision a few years after Mitra Clip intervention.
A double chamber transvenous defibrillator was implanted because of sinus node dysfunction.
This patient presented multiple arrhythmic events (VF), each one preceded by a prolonged QT interval. The initial aborted SCD was due to the acute coronary syndrome and MVP with severe mitral regurgitation, the fallowing two arrhythmic events occurred shortly after a Mitra Clip intervention, in the context of betablocker interruption and no other potential trigger found, except the variability of the QTI, with prolonged QT interval before VF.
Risk stratification of MVP is not clear despite the plethora of risk factors associated with it because there is still no strong predictor of malignant arrhythmias. Additionally, it is not clear which combination of risk factors incurs the highest risk.
The diagnosis of long QT syndrome (LQTS) is primarily based on the measurement of the QTc interval (corrected QT), which is usually elongated, although 20% to 25% of patients with mutation confirmed LQTS may have normal QTc; the overlap in resting QTc intervals between healthy people and patients with LQTS makes diagnosis difficult.
The association between LQTS and mitral prolapse is classical but understudied and not fully understood; these patients frequently have negative and asymmetrical T waves in the inferior leads and a QT interval slightly longer than normal, but they are not genotyped because it is considered that these modifications are caused by the mechanical traction/stretch of the pillars.
These also means that any further enlargement of the QT interval in patients with mitral valve prolapse (caused by ischemia, inflammation, fibrosis, QT-prolonging drugs, hypokalaemia, hypocalcaemia, hypomagnesemia etc) can increase the risk of arrhythmic event and sudden cardiac death much more then in patients without mitral valve prolapse.
An unknown proportion of patients have a congenital LQTS associated to mitral valve prolapse and their risk of SCD is even greater.
The congenital LQTS type 3 is more difficult to diagnose, and it differs from LQTS1 and 2 in various aspects. LQTS3 patients present more often with marked resting bradycardia and QT prolongation is more pronounced during slow heart rate (rest, sleep) with in fact normalisation at faster heart rates. The first cardiac event is more likely to be fatal. Of the known genetic variants of the long QT syndrome, the long QT3 variant results from mutations in the SCN5A gene and accounts for 5% to 10% of clinical cases.
Sudden cardiac death was described due to a novel disease causing mutation in the SCN5A gene encoding the cardiac sodium channel in a patient with myxomatous mitral valve disease and flail posterior leaflet treated with the macrolide antibiotic azithromycin.
Prolongation of the QTc interval in patients with MVP has been reported in several studies. The incidence in these studies has been variable, ranging from 91 to 26%. Not all investigations, however, have found a correlation between MVP and prolonged QTc intervals. The Framingham study revealed no evidence of QT prolongation in association with MVP. The incidence of QTc prolongation has clinical significance because several investigators have implied a relation between this repolarization abnormality and sudden death in patients with MVP.
This case suggests that there is a significant variability in the QTc interval in patients with idiopathic mitral valve prolapse (no congenital LQTS) with the appearance of a long QT interval preceding malignant arrhythmias and SCD.
The discovery of a long QT interval in a patient with MVP and bradycardia (but normal QTI when the heart rate is high) could suggest the coexistence of a congenital LQTS3. Studies are necessary to see if beta-blockers could unmask this syndrome.
There is increasing evidence of a genetic association between MVP and LQTS, atrial fibrillation, sinus node dysfunction and cardiomyopathy (dilated cardiomyopathy, noncompaction).
“SCN5A gene encodes the pore-forming ion-conducting α-subunit of the cardiac sodium channel (Nav1.5), which is responsible for the initiation and propagation of action potentials and thereby determines cardiac excitability and conduction of electrical stimuli through the heart. The importance of Nav1.5 for normal cardiac electricity is reflected by various disease entities that can be caused by mutations in SCN5A. Gain-of-function mutations in SCN5A lead to more sodium influx into cardiomyocytes through aberrant channel gating and cause long QT syndrome, a primary electrical disease of the heart. Loss-of-function mutations in SCN5A lead to lower expression levels of SCN5A or production of defective Nav1.5 proteins and cause Brugada syndrome, an electrical disease with minor structural changes in the heart. In addition, both loss- and gain-of-function mutations may cause dilated cardiomyopathy, which is an arrhythmogenic disease with gross structural defects of the left ventricle (and sometimes both ventricles). Other SCN5A-related diseases are multifocal ectopic premature Purkinje-related complexes (gain-of-function mutations), isolated cardiac conduction defect (loss-of-function mutations), sick sinus syndrome (loss-of-function mutations), atrial fibrillation (loss-of-function or gain-of-function mutations), and overlap syndromes (mutations with both loss-of-function and gain-of-function effects). Growing insights into the role of SCN5A in health and disease has enabled clinicians to lay out gene-specific risk stratification schemes and mutation-specific diagnostic and therapeutic strategies in the management of patients with a SCN5A mutation” (A).
Longitudinal studies are necessary to determine if the prolongation of the QT interval just before malignant arrythmia is the underlying mechanism of SCD in MVP.
The possibles implications of confirming this mechanism are significant. Should we treat MVP like a congenital LQTS?
Beta-blockers and lifestyle modifications such as avoiding stimulants such as caffeine, tobacco, alcohol and recreational drugs are already recommended in MVP.
An ICD is indicated for the secondary prevention of out-of-hospital cardiac arrest. Implantation of a loop recorder may be considered dependent on the number of high-risk features present. In the case of suspected arrhythmic syncope and evidence of scarring, it is acceptable to consider an electrophysiology study. Catheter ablation of scar-related malignant arrhythmias has been reported as an effective treatment, but recurrence rate is high.
Prevention and correction of electrolyte abnormalities (hypokalaemia, hypocalcaemia, hypomagnesemia) that can occur during long hospitalisations or in cases of diarrhoea, vomiting, metabolic disorders and unbalanced diets is necessary in all cases.
Aggressive prevention of ischemic heart disease is paramount.
The fallowing questions are to be answered.
Should we genotype all MVP patients? Or only those with high-risk features for SCD ?
As a preventive measure for SCD associated with MVP, should these patients be treated with high dose, non-selective beta-blockers? Should we ban QT-prolonging drugs like amiodarone, sotalol, flecainide, macrolides etc or competitive sport? Should an ICD be implanted if a significant variability of the QT interval is found in MVP patients? Or in case of a sinus node dysfunction necessitating pacing?
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
