
Case Report | DOI: https://doi.org/10.31579/2690-4861/159
Division of Cardiovascular Medicine, Department of Internal Medicine, University of California (Davis) Medical Center, Sacramento, CA, USA.
*Corresponding Author: Sandhya Venugopal, Division of Cardiovascular Medicine, Department of Internal Medicine, University of California (Davis) Medical Center, Sacramento, CA, USA.
Citation: P Prasad, M Majid, P Applegate, Ali A Mahdi, S Venugopal. (2021). Mitral Stenosis: Making the diagnosis. International Journal of Clinical Case Reports and Reviews. 8(5); DOI:10.31579/2690-4861/159
Copyright: © 2021 Sandhya Venugopal, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 03 August 2021 | Accepted: 27 September 2021 | Published: 05 October 2021
Keywords: rheumatic heart disease; echocardiographic surveillance; mitral stenosis
The case of a 60-year-old man illustrates a number of important features of rheumatic heart disease (RHD). The patient’s age of presentation was late (>50 yo) and he had no history of predisposing condition for RHD but served in the South Pacific when he was in the US Navy. RHD was limited to mitral stenosis in this patient and his presentation of heart failure was late. His ECG revealed ample evidence of right ventricular enlargement, and echocardiography demonstrated severe mitral stenosis, enlarged right ventricle and right atrium and marked pulmonary hypertension. Because percutaneous balloon mitral valve commissurotomy was precluded by the degree of mitral valve calcification, he underwent successful surgical valve replacement with relief of symptoms. Although RHD is rarely encountered in North America and Europe, it remains a major cause of mortality in the developing nations.
A serious heart condition went unnoticed for decades – and then advanced to the point of requiring prompt surgical intervention. The patient, a 60-year-old man with no past medical history, presented with a month of progressive dyspnea on exertion. For the past two weeks, he noted increasing orthopnea and intermittent wheezing and palpitations. He was not taking any medications and had not accessed medical care recently. He served in the Navy in Southeast Asia during his teens and twenties, was a current smoker, and was working as a welder and carpenter with carbon and asbestos exposure. His brother died of a myocardial infarction at age 46 years as did his father at age 51 years.
The patient was tachycardic (106 bpm), but with otherwise unremarkable vital signs (O2 saturation: 96% on room air, respiratory rate: 18/min, blood pressure: 111/75 mmHg, temperature: 99.4° F.) and he was interacting appropriately. He appeared cachectic and on cardiac examination had a regular rhythm, normal S1 and S2, and a 2/6 apical systolic murmur with a faint diastolic rumble. P2 was not accented, there was no parasternal lift, and an opening snap was not detected. No gallops or rubs were audible, and his jugular veins were difficult to visualize. The patient’s lung sounds were diminished at the bases and there were coarse crackles from bases to mid-back. There were no focal neurologic findings.
Laboratory data: cardiac troponin: <0>
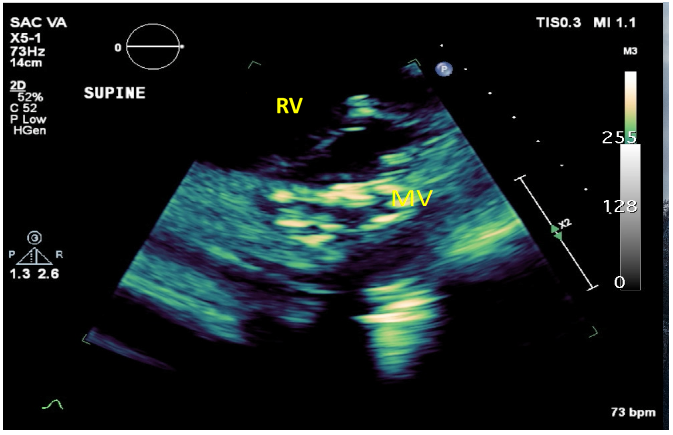
A chest radiograph showed moderate bilateral pleural effusions and prominent interstitial markings. Calcifications were present along the aortic arch. Computed tomography (CT) of the chest revealed cardiomegaly, mild pulmonary edema, and large bilateral pleural effusions. Transthoracic echocardiogram (TTE) (Figures 1 and 2) disclosed markedly thickened, severely calcified mitral valve leaflets with commissural fusion and severely decreased excursion indicative of critical mitral valve stenosis (MS) with a mean gradient of 26 mmHg ref <2>
CT of the head showed chronic microvascular changes and a left basal ganglia hypodensity, which may reflect prior lacunar infarct. Carotid ultrasound revealed large bilateral calcified plaques resulting in narrowing with doppler findings suggesting 50-79% bilateral stenosis.

What is the diagnosis?
Diagnosis: Rheumatic heart disease with severe mitral stenosis
The degree of MV leaflet thickening, calcification, commissural fusion and decreased leaflet mobility on the patient’s echocardiogram indicated that the severe MS and subsequent heart failure were the result of rheumatic heart disease (RHD). Several aspects of his case are noteworthy. A majority of patients with MS do not have an overt history of antecedent streptococcal infection, which was absent in our patient [1]. Women have a higher prevalence of RHD than men, and patients usually become symptomatic between ages 20-50 years [1]. Therefore, our patient’s clinical presentation was late.
RHD is a consequence of repeated valvular damage induced by multiple episodes of acute rheumatic fever (ARF) and/or subclinical rheumatic valve inflammation [1]. In a genetically susceptible host, ARF results from antigenic mimicry in association with an abnormal immune response to group A streptococcal infection involving both humoral and cellular components1. These processes usually involve the pharynx and also joints, skin, brain and heart. Mitral valve incompetence is the most common valvular lesion in early stages, but recurrent valvulitis can cause progression to mitral stenosis with bicommissural fusion, which can critically reduce the mitral valve orifice [1]. To maintain blood flow across a stenotic valve, a pressure gradient develops leading to increased left atrial pressure and left atrial dilation, predisposing patients to pulmonary hypertension and atrial fibrillation. The result of these pathophysiologic derangements includes congestive heart failure and the hazard of systemic embolism [2].
While the global mortality from RHD has declined by approximately 50% since 1990, this disease remains a significant cause of death with the highest rates in India, China and Pakistan [3]. Echocardiography is the gold standard for diagnosis and has revealed a higher RHD prevalence than thought previously when auscultation of the characteristic murmurs was the main diagnostic tool [4]. The World Heart Federation criteria were developed in order to assist with systematic diagnosis of RHD. For MS related to RHD, congenital MV anomalies and nonrheumatic mitral annular calcification must be excluded. The MV morphologic criteria include commissural fusion, anterior MV leaflet thickening (age-specific), chordal thickening, restricted leaflet motion and excessive leaflet tip motion during systole [4].
Treatment of RHD focuses on echocardiographic surveillance and prevention and management of complications, including heart failure, atrial fibrillation, cardio-embolic events, and infective endocarditis [1, 4]. Pregnancy in patients with RHD complicated by right ventricular dysfunction and pulmonary hypertension is associated with high maternal and fetal morbidity and mortality and requires antenatal consultation with cardiology and obstetrics [1]. Interventional treatment is warranted when patients with severe valvular lesions become symptomatic [5]. The choice of mechanical vs. bioprosthetic material for valve replacement depends on the patient’s age, pathologic anatomy of the MV and ability to safely adhere to anticoagulant treatment [6-7]. For mitral stenosis, percutaneous mitral balloon commissurotomy has replaced surgical commissurotomy in patients with suitable MV anatomy and yields excellent mid-term results, with a 50–60% event-free outcome at 10-year follow-up in a recent retrospective study of 1024 patients undergoing this procedure [8]. In patients with MV anatomy unsuitable for percutaneous commissurotomy, valve replacement involves considerations of type of valve (mechanical or bio-prosthetic) patient age, pathology of the MV and capacity to safely adhere to anticoagulant therapy [7].
Echocardiographic criteria and lack of ischemic heart disease on coronary angiography supported the diagnosis of rheumatic mitral stenosis as the etiology of our patient’s cardiac pathology and heart failure. His ECG suggesting severely elevated right ventricular systolic pressure was confirmed by on echocardiography. He received judicious diuresis, given preload dependency in severe mitral stenosis, and received in-patient monitoring for arrhythmias which were as not detected on telemetry [9]. Because of findings of a prior stroke on head CT, and carotid artery stenosis, he was started on secondary prevention for stroke with aspirin and a high-intensity statin. The patient’s markedly calcified mitral valve precluded commissurotomy and as a military veteran, he was transferred to a regional Veterans Administration hospital for mitral valve replacement. After successful cessation of smoking, his mitral valve was replaced, and he experienced early resolution of symptoms.
Financial/nonfinancial disclosures: None declared.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
