
Research Article | DOI: https://doi.org/10.31579/2578-8868/278
1MAOS Aguilar Eloy M HIMFG Nurses Office 2019
2EEI. Ma. Del Rocío Casas Service Specialties HIMFG 2019
3Head of the Department of Nursing Saldívar F. Araceli- HIMFG-2019
4Deputy Head of the Department. Of nursing. Aguilar G. Olivia- HIMFG 2019
*Corresponding Author: Eloy Margarita Aguilar, Neurophysiology Department, Ysbyty Gwynedd Hospital, Bangor, North Wales, UK. LL57 2PW.
Citation: Aguilar E. Margarita, Ma. Del Rocío Casas Ramírez, Araceli Saldívar Flores, Olivia Aguilar-Guzmán and Cols, (2023), Missed nursing care in hospitalized pediatric patients, perceived by mothers and nursing staff in a tertiary care institution, J. Neuroscience and Neurological Surgery, 14(2); DOI:10.31579/2578-8868/278
Copyright: ©, 2023, Aguilar Eloy Margarita. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 21 November 2023 | Accepted: 08 December 2023 | Published: 22 December 2023
Keywords: Neuromodulators ; Serotonergic modulation ; neural functions
Introduction: Missed nursing care refers to the care that the patient requires and that is totally or partially omitted or significantly delayed, in the pediatric population implies its identification due to its vulnerability; They do not yet have the capacity to identify their needs to demand their fulfillment. Objective: Identify missed nursing care and its relationship with the reasons, in the pediatric population, based on the perception of mothers and nursing staff.
Methodology: Cross-sectional descriptive study, 209 mothers of pediatric patients and 69 nurses from a tertiary care institution participated. The data was collected using the MISSCARE instrument, the analysis was based on descriptive and inferential statistics.
Results: The care that is lost according to the primary caregiver are: Basic care: Support in hand washing 25.66%, oral care 45.9%, support for walking 36.4%. Care is lost due to lack of human resources 72.13% and materials 68.26%, highlighting the unexpected increase in patients 84.2% and lack of communication with other departments 67.5%. The nursing professional mentions loss of basic care; support for walking 23.2, checking indicated diet 21.7; The reason for the lost care is due to lack of material resources in 98.5%, lack of human resources in 87.68, unexpected increase in patients 100% and insufficient support staff 98.6%, communication 91.59; In the work environment, 50.14 identify a lack of leadership.
Conclusions: The care lost in the hospitalized pediatric patient is due to a deficit in human resources, materials, lack of support from other departments and communication
The health of the Mexican population is a fundamental area established in article 4. of the country's Political Constitution (1) and described in the General Health Law (2), for which there is a care coverage of 300,000 nurses (3), The OECD considers there should be 9 nurses per 1000 inhabitants, however, we have 3.3 (4)
The child population from 0 to 14 years old is 31,752,284 and adolescents from 15 to 19 years old are 10,806,690 in the country, (5); It is necessary to have a care program for their growth and development, prevention and timely care in case of illness or later rehabilitation to reintegrate them into their social context.
Over the past decade, researchers have examined missed nursing care in hospitalized patients as an indicator of the quality of nursing care. Two systematic reviews have documented the predictors and consequences of lack of nursing care in inpatient settings (6). It is worth mentioning that patient care professionals provide services in both the public and private sectors. Their inherent condition is to guarantee quality care, in such a way that the presence of adverse events is avoided during the patient's hospital stay. the patients; In the particular case of this work it is about children; reason that allows us to consider within the adverse events, the omission of nursing care, which in turn generates alteration in the circle of care, Kalisch defines missed care, “as any aspect of the required patient care that is omitted from partially or totally or that is significantly delayed” (7)
From the point of view of quality, it is expected to meet patient expectations and user satisfaction; Studies carried out by Kalisch, are based on Dr. Avedis Donabedian 's model that involves obtaining information to describe and evaluate existing systems, because poorly designed systems lead to inefficiencies, errors and delays, therefore, making changes in The system includes measuring them in its structure (8-9) . (personnel-characteristics of the care unit), process (patient care procedures, were they followed?, reduced...?) and results (condition of patient discharge, iatrogenic: pressure ulcers, accidents such as puncture with a needle of unknown origin, extension of stay days...).
For Kalisch, there are four dimensions of care to understand: Individual needs, discharge planning, and education; basic care interventions and care interventions with continuous evaluations that allow decision making. (10)
It is important to consider that the majority of studies aimed at omitting missed care have been carried out in hospitalized adults, but not in pediatric patients; there is very little information; The study intervention in the child is directed at the mother or primary caregiver of the pediatric patient, because age does not allow her to fully distinguish if there is any omission, unless the patient is a chronic patient who has been trained in the various procedures such as: dialysis, care of the catheter or probes, administration of specific medications such as antiretrovirals, being offered a diet that does not correspond...generally, the information is accessible in children eight years of age and older.
It is important to mention that there is a shortage of nursing personnel to provide care to hospitalized children; despite continuing education; The number of nurses is limited to meet this demand. According to Ms. Moreno Monsiváis in his article lost nursing care perceived by mothers of pediatric patients , found that the care that is mainly lost is discharge planning and patient education, followed by basic care in 82.1% (helping or performing oral hygiene and hand washing), verify that the food is at the appropriate temperature 62.1%, bring the food closer and verify the diet before they eat it 61.1%; In addition to lack of materials and equipment or medications, the care that is lost is due to human resources reasons; The unexpected increase in patients and workload was 47%, due to emergency situations, greater attention is required and the time to care for other patients is reduced by 34.5%. 10)
These factors are considered fundamental in the omission, rationing or delay of direct care to the patient. Several researchers have highlighted this problem that had not been analyzed precisely, although it was known vaguely, it was not demonstrated; We now know that workloads generate emotional and physical exhaustion accompanied by a state of frustration when failing to provide comprehensive patient care; On the other hand, the effectiveness of teamwork has been demonstrated, by substantially reducing the omission of care. The impact generated by the work environment and staff training is also known.
The loss or delay of care could represent a legal problem due to omission, which implies having sufficient nursing resources to guarantee the quality of care.
The objective of this research is to identify the lost care reported by the mother or caregiver of the pediatric patient.
By issuing the results of investigations into lost care, it will allow managers to justify the needs of human, budgetary, material and structural resources to the corresponding authorities.
Observational, cross-sectional study through interviews with mothers of pediatric patients hospitalized at the Federico Gómez Children's Hospital of Mexico and in parallel, independently of the nursing staff who were caring for them, without there being any information in this regard on both sides.
The research protocol was approved by the Ethics Research and Biosafety Committees of the Hospital Infantil de México Federico Gómez (HIMFG).
The instrument applied was previously piloted in coordination with the National School of Nursing and Midwifery (ENEO)
The participants agreed voluntarily, after explanation and signing of informed consent.
207 mothers or fathers who assume the role of primary caregiver were interviewed, their children were under 18 years of age, at least 72 hours of hospitalization, parents who had children in short-stay services, intensive care units, were excluded. emergency room, operating room, outpatient surgery. They were selected through probabilistic random sampling for finite populations with a confidence level of 95% and a margin of error of 5%.
69 nurses in charge of patients were interviewed independently. The same items were evaluated as the primary caregiver; They were also asked about the work environment in which they work.
Missed nursing care and the reasons that lead to it were evaluated through the MISSCARE survey, with validity and reliability previously documented and adapted for its application in the Mexican population. The survey is made up of 64 items classified into three sections:
1.-Demographic data of the caregiver, mother or father: age (<25>
2.-Missed Nursing Care: includes four dimensions of care that mothers or fathers perceive while caring for their child.
Individual Needs, discharge planning and patient education, basic care and continuous evaluation care, the section is made up of 24 Likert-type items , six response options, namely: always = 5, frequently = 4, occasionally = 3, rarely = 2, never = 1 and not applicable = 0 (which is generated for care that is not carried out during the night shift, such as feeding the patient, ambulation...), the responses were recategorized in a binary way, (1 =always or frequently, 0=otherwise) and added n in an unweighted additive score of global lost care for each dimension, they were expressed on a percentage scale. Higher values in both, suggest greater lost care
3-Reasons that lead to lost care:
Human resources, material resources and communication, section made up of 17 Likert-type items with four response options: Significant reason 4, moderate reason 03, minor reason =2, not a reason =1.
The analysis is carried out using the SPSS V.25 statistical package, initially the main demographic characteristics of the sample are described (mean, percentages) followed by the average percentage with 95% CI) of the global lost care indices (based on its four dimensions) and the reasons that lead to its occurrence (human resources, materials and communication).
Lost Nursing Care, perceived by this professional.
In this results section, the demographic and work characteristics of these professionals are shown, then the Missed Care is described, as well as the dimensions that are missed with the greatest proportion; Subsequently, the significant reasons they perceive for missing nursing care are stated; Finally, the work environment and its dimensions are described based on the perception of the staff themselves.Demographic and employment
characteristics
The sample was made up of 69 nurses who work at the Federico Gómez Children's Hospital of Mexico. An average age was 37 years, with a range of 25 to 54 years. Sex was characterized as 21.7% men and 78.3% women. According to the last degree of training, it was found that 53.6% have nursing degrees and 26.1% have a specialty.
70% hold the category of general nurse A, B, C and 30% specialist A, B or C.; 39.1% of the nurses surveyed work on the night shift, 31.9% on the morning shift and 29% on the afternoon shift. Table 1.
| n = 69 | Fo | % | |
| Sociodemographic | |||
| Age (years), mean | 37 + 8.04 | ||
| 25-35 | 37 | 53.6 | |
| 36-45 | 19 | 27.5 | |
| 46-54 | 13 | 18.8 | |
| Sex | |||
| Women | 54 | 78.3 | |
| Man | fifteen | 21.7 | |
| Last level of training | |||
| Nurse technician | 6 | 8.7 | |
| Post-technician in nursing | 2 | 2.9 | |
| Nursing degree | 37 | 53.6 | |
| Specialty | 18 | 26.1 | |
| master's degree | 6 | 8.7 | |
| Category in institution | |||
| General Nurse A | 5 | 7.2 | |
| General Nurse B | 12 | 17.4 | |
| General Nurse C | 31 | 44.9 | |
| Specialist nurse A | 1 | 1.4 | |
| Specialist nurse B | 1 | 1.4 | |
| Specialist nurse C | 19 | 27.5 | |
| Work shift | |||
| Morning | 22 | 31.9 | |
| Evening | twenty | 29 | |
| Night | 27 | 39.1 |
Table 1. Demographic characteristics of nursing professionals,
Professional satisfaction was measured with 4 items on a scale from 1 to 5, where: 1=Very dissatisfied and 5=Very satisfied. Each item was recoded into a binary variable (0 and 1) where 0= dissatisfaction and 1= Satisfaction. Then the items were added, where: <3>4= Satisfied. An average of 3.75 ± 0.46 was found, in addition, 23.2% of the staff are dissatisfied and 76.8% satisfied. Table 2.
| n = 69 | Fo | % | |
| Satisfaction | |||
| Dissatisfied | 16 | 23.2 | |
| Satisfied | 53 | 76.8 |
Table 2. Total professional satisfaction.
Perception of Lost Nursing Care
Lost nursing care was measured with the MISSCARE Instrument ( Kalisch ), which is made up of 24 items on a Likert-type scale, where: 1= Care is never lost and 5= Care is always lost. Each item was recoded into a binary variable (0 and 1), where 0 is care provided and 1 is care missed. Finally, the items were added by dimension and global score of lost care, calculating an index on a scale of 0-100.
global lost care index perceived by HIMFG nursing professionals was 19.38%. By dimension, a greater loss or delay was observed in Individual Needs (18.84%), followed by Basic Care (16.81%), Patient Education and Discharge Plan (14.49%) and finally Continuous Evaluations care (4.35%). Table 3.
| n = 69 | Half, % | Confidence Interval 95% | |
| lower | Superior | ||
| Half, % | |||
| Global | 19.38 | 13.09 | 25.68 |
| Individual needs | 18.84 | 11.38 | 26.30 |
| Education and Discharge Plan | 14.49 | 7.95 | 21.04 |
| Basic care | 16.81 | 10.61 | 23.01 |
| Continuous care evaluation | 4.35 | -0.59 | 9.28 |
Table 3. Lost nursing care globally and by dimensions.
In the dimension of Individual Needs , the care that is most often lost or omitted are: Evaluation with multidisciplinary visits (26.1%), help going to the bathroom (7.2%) and administration of medications (4.3%). Figure 1.
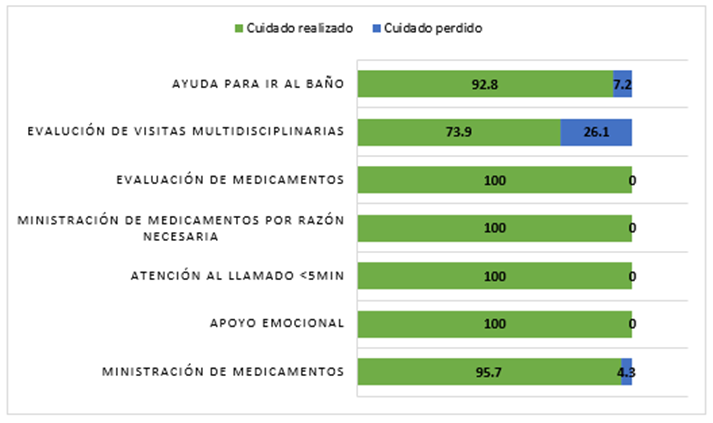
Figure 1. Lost nursing care, Individual Needs dimension
The dimension of discharge planning and patient education documents is lost 14.49%. The care that is most missed or delayed is related to hospital discharge planning (23.2%), followed by patient education (5.8%). Figure 2.
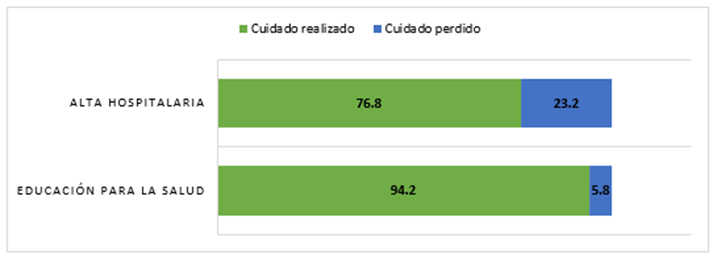
Figure 2. Missed nursing care, discharge planning and patient education dimension
In the Basic Care dimension, support for walking (23.2%), verification of indicated diet (21.7%) and support for bathing (10.1%) are identified as being lost in a higher percentage. Figure 3.
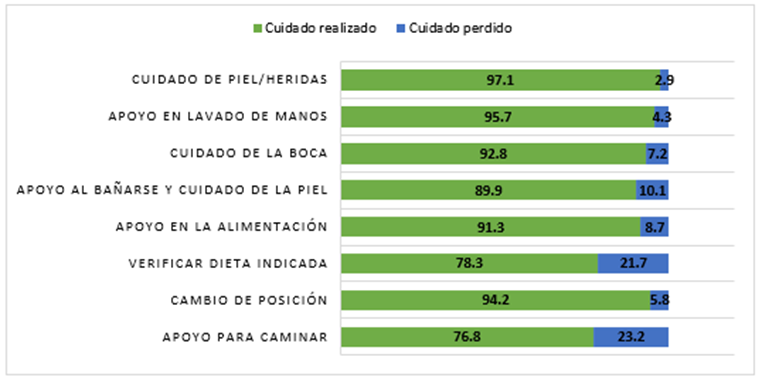
Figure 3. Missing Nursing Care, Basic Care dimension
Finally, in the Continuous Evaluations dimension, the aspects that are most lost are the registration of income and expenses, condition assessment and reevaluation of current condition, all with 1.4% respectively. Figure 4.
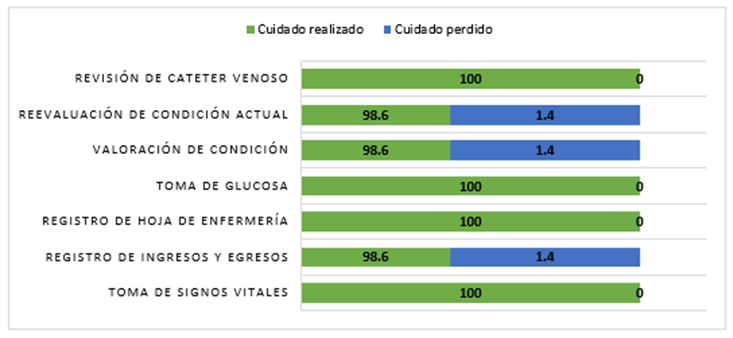
Figure 4. Lost nursing care, Dimension Continuous evaluations
Reasons for Missed Nursing Care
Section B of the MiSSCARE instrument consists of 17 items that describe the reasons why nurses who provide care to pediatric patients perceive that care is lost or delayed. With a Likert-type scale where: 1= is not a reason and 4= is a significant reason. Each item was recoded into a binary scale (0 and 1), where 0 = It is not a reason and 1 = It is a significant reason. Finally, the items were added by dimension and total score, calculating an index on a scale of 0-100.
The global index of significant reasons for missed care was 89.69 (95% CI 85.25-94.14); Those with the highest percentage for losing care are Material Resources (98.55%), followed by Communication (91.59%) and Human Resources (87.68%). Table 4.
| n = 69 | Half, % | Confidence Interval 95% | |
| lower | Superior | ||
| Half, % | |||
| Global | 89.69 | 85.25 | 94.14 |
| Human Resources | 87.68 | 82.57 | 92.79 |
| Material resources | 98.55 | 95.66 | 101.44 |
| Communication | 91.59 | 86.99 | 96.70 |
Table 4. Significant reasons for Missed Nursing Care.
In relation to the Human Resources dimension, the lost nursing care is mainly due to the unexpected increase in patients (100%), insufficient support staff (98.6%), emergency situations and insufficient staff (97.1%). Figure 5.
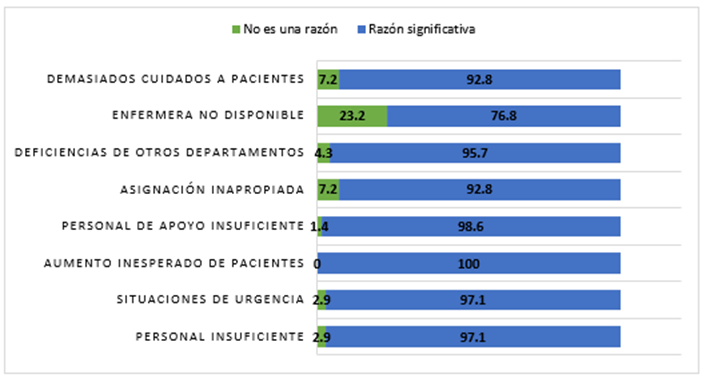
Figure 5. Significant reasons for lost care, Human Resources dimension.
Regarding material resources, 100% of nursing professionals report that care is lost or delayed because there are no medications available or the medical equipment is not functional , and 98.6
The present study reports the perception of the primary caregiver in relation to the lost care identified during the care of their hospitalized patient and the perception of the nursing staff in the same areas, in addition, the work environment. The study institution, considered a third level of care, is made up of 100% professional staff. highly qualified.
We will start with the primary caregiver. In relation to user satisfaction with the care received, they say they are satisfied in a very good percentage.
The global index informs us that lost care occurs in a lower percentage in relation to those described in (11), however it was a little higher than in a private institution, in reference to the dimension of intervention of individual needs it was also The loss is relatively not so high, surely the permanence of the family member encourages them to be aware of their child and request care in a timely manner. It is worth mentioning that pediatric nursing staff develop a great capacity for attention, concentration and anticipation, given the needs of the children. children; It was identified that the care that is missed the most is the evaluation with multidisciplinary visits, which coincides with the data obtained in (11) and help to go to the bathroom, this with a not so significant percentage, surely due to the condition of the patients to whom They have fluid control through a strict balance and it implies their continuous attention and also collaboration of the family member, in relation to the evaluation of medications, there is very good coverage, which contrasts with the private institution, this is not the case in the other public institution.
The Basic Care Dimension is lost in a lower percentage than that found in (10)(11), however: significant in oral care, hand washing and support for walking, the presence of the family member is participatory in this area. It is worth noting that in the verification of the diet, if it is carried out in an important way, it is not the case to confirm that the temperature is adequate, which in other studies does result in high omissions; the participation of the family member is evident, so We infer that the staff gives priority and interventions with a higher degree of difficulty. The continuous evaluation of care is very positive, the loss is minimal according to the present and referred studies.
For discharge planning and patient education, family members report a low percentage of the loss in this area, surely because teaching family members is inherent in the institution, only some relatively recently hired personnel do not do it or perhaps because limited difficulty and time.
The reasons that mothers point out, in a high percentage; for care to be lost are due to the lack of human resources, followed by material resources and communication in this specifically the lack of communication with other departments, lack of clarity in medical indications - which we consider will be reduced because it is being Integrating the electronic record system into the hospital will make medical indications clear - and lack of support among staff is another reason cited.
Based on the responses of the nursing staff, the majority are relatively young staff, all from the bachelor's level, there are no auxiliary nursing staff, the majority are women, who mention being satisfied in their work, but not the entirety. They report having an average of four to five patients assigned.
The care lost in your overall evaluation is good, however, it could improve. In the dimension of individual needs, they mention greater loss in the evaluation of multidisciplinary visits, which coincides with other authors but, in a lower percentage (10.), it is worth noting that emotional support is a characteristic that is very typical of the institution. and the nursing staff fulfills it to the maximum, an area that does not happen in what was mentioned in a private institution (10), in terms of the dimension of basic care, it is lost in the verification of the indicated diet, and support for walking happens in the same way. Likewise with the aforementioned authors (10), although it has been emphasized that the presence of the family member is of great supportive support, we must recognize that during the patient's stay, the responsibility for his or her care will always be the nurse's. Discharge planning is lost in a lower percentage reported by other authors, in the area of health education it is very positive in this institution.
In the dimension of continuous evaluations, the percentage of loss, referred to in the re-evaluation of the current condition, and registration of admissions and discharges, is minimal, because all patients have a medical indication for this control, external factors, changes or others imply discreet loss.
The evaluation of the significant reasons for lost nursing care informs us of high percentages due to the lack of human resources, material resources and communication, this coincides with what is also reported by the Joint Commission. The work environment reports a lack of adequate resources and leadership.
It was considered to relate the presence of adverse events with the loss of care, a fact that was not documented, since none were presented, however; Collaterally, the database related to the institution's adverse events was reviewed and at that time of the investigation there were five cases unrelated to the population studied.
Lost nursing care is widely known, but it needed to be demonstrated through a solid study in this case in the pediatric field, it is a truth that has not been accepted and causes the staff to provide care coverage regardless of the prevailing situation in each institution, therefore it is demonstrated that the lack of human resources, materials and communication affects the care that is lost, omitted or delayed; With this detailed information, the corresponding authorities have bases to justify the demand for resources and cover these needs that allow generating quality in patient care and safety.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
