
Case report | DOI: https://doi.org/10.31579/2578-8868/324
Department of Neurosurgery, University of Arizona/Banner University Medical Center Phoenix.
*Corresponding Author: Julie Mayeku, Department of Neurosurgery, University of Arizona/Banner University Medical Center Phoenix, 1111 E McDowell Rd, Phoenix, AZ 85006.
Citation: Julie Mayeku, Chao Li, Robert Bina and Ali Baaj, (2024), Minimally Invasive Transpedicular Approach with Stereotactic Navigation for Evacuation and Fusion of Thoracic Ventral Epidural Abscess of Thoracic Spine: an illustrative case, J. Neuroscience and Neurological Surgery, 16(1); DOI:10.31579/2578-8868/324
Copyright: © 2024, Julie Mayeku. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 10 June 2024 | Accepted: 15 July 2024 | Published: 01 August 2024
Keywords: minimally invasive; transpedicular approach; stereotactic navigation; thoracic spine; ventral epidural abscess
Background: Surgical treatment of ventral thoracic pathologies can be challenging due to anatomical restrictions limiting corridor access, need for extensive spinal cord manipulation and limited experience for most spine surgeons’ due rarity of ventral thoracic pathologies. There is growing evidence that creation of a ventrolateral operative corridor through minimal invasive (MIS) transpedicular approach is safe and effective for accessing and treating of ventral thoracic spinal lesions [ 1-6] However, poor visualization with difficulty of spinal cord manipulation due to tubular retractor restriction remains changeling for MIS transpedicular approach.
Objective: The authors illustrate a case of concurrent utilization of MIS tubular approach and stereotactic navigation to ensures safe and effective removal of epidural abscess and subsequent fusion.
Conclusion: Addressing any lesion located anteriorly to the dentate ligament can be challenging and often necessitates either an antero-lateral or an anterior approach. This choice may depend on various factors, including the availability of an access surgeon. Utilization of stereotactic navigation with MIS transpedicular approach for ventral thoracic lesions, allows for real time intraoperation localization and visualization increasing lesion targeting accuracy and less cord manipulation. It also provides immediate post instrumentation checks and less radiation exposure for operating personals.
Due to limited midline access, surgical intervention of ventral thoracic spine pathologies requires transthoracic, posterolateral, transfacet or transpedicular approaches. Anatomical limiting corridor access and need for spinal cord manipulation in a narrow spinal canal the makes it challenging to access the anterior of spinal cord, with increasing risk of cord injury. Rarity of thoracic ventral pathologies limit experience for most spine surgeons with increasing the surgical comorbidities associated with surgical treatment of these lesions [1-6]. There are growing evidence that creation of a ventrolateral operative corridor through a transpedicular is safe and effective for accessing the ventral thoracic spinal cord. With evolving from open to minimally invasive surgery, MIS transpedicular approaches via tubular retractor systems have shown better clinical results than open transpedicular with regards to ventrolateral operative corridor access [2,5,6]. However, poor visualization with difficulty of spinal cord manipulation due to tubular retractor restriction remains changeling for MIS transpedicular approach [2]. Utilization of stereotactic navigation with MIS transpedicular approach for ventral thoracic lesions allows for real time intraoperation localization and visualization increasing lesion targeting accuracy and less cord manipulation. Immediate post instrumentation check improving accuracy and safe of MIS transpedicular technique [5]. Additional advantages of stereotactic navigation include, immediate post instrumentation checks and less radiation exposure for operating personals. We report a case of successfully decompression and fusion of patient with osteomyelitis, cord compression and ventral epidural abscess of thoracic spine using Minimal Invasive Transpedicular technique with stereotactic navigation. Patient received immediate symptomatic relief and neurological deficit restoration.
Surgical Technique:
Patient was placed in prone position, Brainlab spine navigation system was used to register and utilized throughout surgery. Percutaneous pedicle screws were placed with aid of the navigation system. Then midline incision was made with tube dilator was placed at level between T7-T8 on the right side. After right hemi-laminectomy and T8 transpedicular exposure was perform with high-speed drill, epidural space was exposed. A significant amount of acute purulent material was collected and sent to pathology. A drain was placed then T6 to T9 arthrodesis and fusion were performed with minimal invasive method.
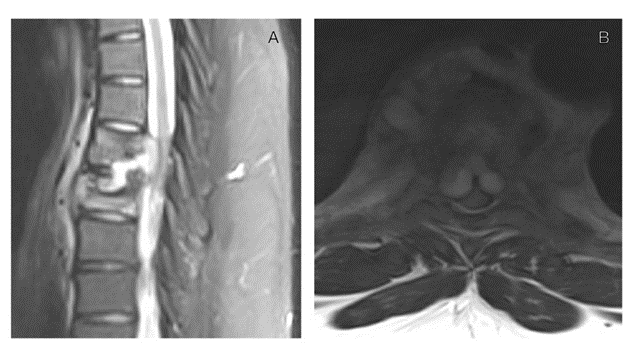
Figure 1. A) Post contrast sagittal Thoracic spine MRI showing T7-T8 osteomyelitis and epidural abscess, B) Axial view of T7-T8 showing epidural abscess with severe cord compression
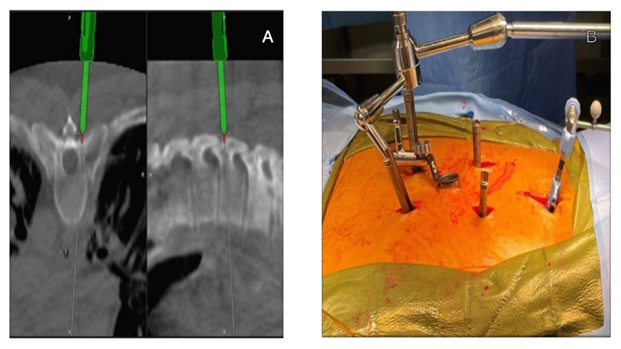
Figure 2: A) CT guided navigation for location of incisions, B) CT guided navigation Localized incisions for percutaneous pedicle screw placement.
Case Illustration:
37-year male with history of hypertension and positive coccidioidomycosis serology who presented with back pain and numbness of bilateral lower extremities and gait instability. MRI thoracic spine showed T8-T9 osteomyelitis with ventral epidural abscess causing cord compression. On exam, he had decreased sensation to light touch from T10 through bilateral lower extremities and gait imbalance. No weakness or myelopathy.
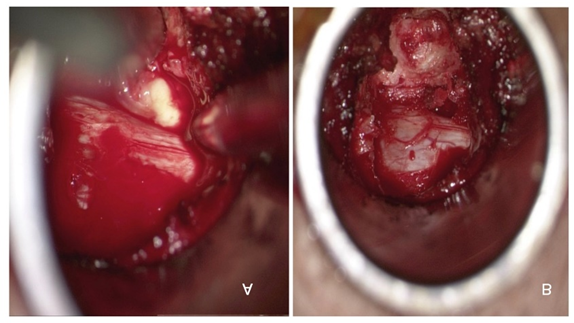
Figure 3. A) Thecal sac and purulent material visualized after T7-T8 MIS Right Transpedicular Hemilaminectomy.
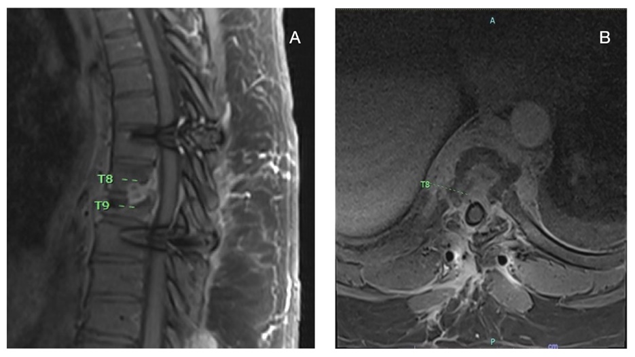
Figure 3 B & Figure 4: A-B Post epidural abscess wash out and decompression) 6 months post operative Thoracic spine MRI.
Surgical treatment of ventrally located thoracic pathologies can be challenging due to the anatomical constraints and need for spinal cord manipulation to reach the anterior portion of spinal canal. Additionally, thoracic ventral lesions are rare in occurrence making for limited operational experience even to experienced spine surgeons, hence higher risk of surgical morbidities. Creation of a ventrolateral operative corridor through MIS transpedicular approach has been shown to be safe and effective for accessing the ventral thoracic spinal cord compared to thoracotomies and other posterior/posterior lateral approaches [2,4,6]. MIS transpedicular approach is however not without limitations. The tubular retractor system limits visualization of surgical field, making it challenging to operate in a narrow spinal canal as well as visualizing ventral spinal cord. We present our case report that use of stereotactic navigation with MIS transpedicular improves accuracy and safety of MIS transpedicular approach by providing intraoperative visualization of the operative anatomy.
For our patient, we used Brainlab spine navigation system intraoperatively to optimize the visualization and targeting of the ventrally located abscess. The navigation probe allowed for trajectory for creation of ventrolateral corridor access to the abscess, guidance to target the ventrally located abscess and instrumentation safely and accurately. We were able to safely decompress, provide needed sample cultures and instrument with minimal tissue injury while mitigating any spinal cord or neuro element injuries. Post decompression and instrumentation images showed good decompression and appropriately placed hardware. Our patient had immediate pain relief and with return of sensation. Patient was discharged home post op day eight following ID and medicine clearance.
In addition to improving surgical accuracy and safe, MIS approach with navigation guidance further allows for less blood loss, shorter surgery times, and decreased length of stay for patients [2,5]. Post-decompression intraoperative image provides verification of decompression and instrumentation allowing for immediate surgical correction if needed. There is also minimized exposure to radiation of operating room personal [5].
MIS transpedicular approach is effective method to evacuate certain ventral thoracic epidural abscess. With aid of frameless stereotactic navigation system, placement of tube dilator is more accurate and efficient. The patient spends less time in hospital, with significantly less blood loss and relatively smaller incision compared to open surgery. In our ventral thoracic spinal epidural abscess case, it shows satisfactory evacuation of ventral thoracic epidural abscess with MIS transpedicular method. The follow up images and clinic visit demonstrate perfect resolution of abscess and good clinical recovery. However patient selection is critical for this type of surgery since the MIS transpedicular approach provides relatively smaller corridor and exposure of ventral part of spinal cord.
None
None
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
