
Research Article | DOI: https://doi.org/10.31579/2768-2757/097
Cardiovascular Surgery Service Dr. Juan A. Fernández General hospital.
*Corresponding Author: Alejandro Ezequiel Bugueiro Bertier, General Surgery Department, Ain Fernández General hospital.
Citation: Bugueiro Bertier AE, (2023), Middle Aortic Syndrome in An Advance Age Patient Description of a Surgical Case, Journal of Clinical Surgery and Research, 4(6); DOI:10.31579/2768-2757/097
Copyright: © 2023, Alejandro Ezequiel Bugueiro Bertier. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 04 September 2023 | Accepted: 20 September 2023 | Published: 11 October 2023
Keywords: aortic coarctation; intermittent claudication; aorta; hypertension; aortic stenosis
Middle Aortic Syndrome : is a rare form of presentation of aortic´s coarctation that represents 0.5-2% of this same entity. It usually occurs in the pediatric or young adult population, which is why the age of this patient is interesting for this case. It mostly affects women with an estimated ratio of 4:1. Renal involvement is the most prevalent and idiopathic etiology is the most frequent.
This pathology presents clinically as difficult-to-control hypertension together with intermittent claudication. This article includes the case of an 81-year-old female patient with a history of hypertension, sedentary lifestyle, smoking, osteoporosis, cholecystectomy in 2010 and appendectomy in childhood. On this occasion, the patient presented a stenosis of the infrarenal abdominal aorta and a superficial femoral artery lesion simultaneously, for which she was approached in a hybrid manner with a straight balloon-expandable stent and a suprapatellar femoral-popliteal bypass.
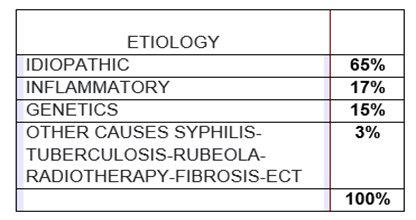
The term Middle Aortic Syndrome was described for the first time in 1947 by Quain and collaborators who observed this pathology in a pediatric age group with an average age of 9 years. Middle Aortic Syndrome is the name we use to denote infradiaphragmatic aortic stenosis. This entity represents 0.5 to 2% of all coarctations of the aorta and mainly affects the pediatric or young adult population with a higher prevalence in women (ratio of 4 to 1 compared to men according to the Coarctation of the Aorta in the study Unusual Sites by Bengt Hulting & Aado Vendsalu). These stenoses occur in different locations and they have a relevant influence on the subject's clinical condition depending on the affected arterial territory. Most commonly, renal artery involvement is observed, which can reach up to 70percentage (within this percentage, two-thirds of the time, both renal arteries are involved bilaterally). The most affected renal areas that are described most frequently (approximately 69percentage) are the suprarenal, leaving the intrarenal location in second place (approximately 23percentage) and last but not least is the infrarenal location (8percentage). as is the case that we will describe below. If it is the renal artery involved, it generally manifests as hypertension that is difficult to control pharmacologically meaning that cannot be controlled by the use of up to 3 antihypertensive drugs at maximum doses. In these cases, the objective would be to reduce the tension below the 95percentage percentile in the pediatric population or, in the event of left ventricular hypertrophy or target organ damage, the 90percentage percentile should be reached. In adults this consists of maintaining systolic pressures below 120 mmHg and diastolic pressures below 80 mmHg. If this hypertension is not treated, it could lead to left ventricular hypertrophy that eventually leads to heart failure, a common cause of mortality in subjects with this pathology. If the involved artery is the superior mesenteric or celiac trunk, this may be reflected as symptoms of intestinal ischemia with its suggestive post-ingestion periumbilical pain and weight loss due to rejection of food. Let us remember that apart from these signs and symptoms, the patient may also experience intermittent claudication which will be expressed by abdominal murmurs and the possible absence of femoral pulses. According to the study Disease Beyond the Arch: A Systematic Review of Middle Aortic Syndrome in Childhood by Rawan et al. its etiologies are multiple but within all the varieties we find that the idiopathic etiology is the most frequent with almost two thirds of all cases. This is followed by the inflammatory cause that shows takayasu as the most relevant and within the genetic origins we can highlight neurofibromatosis type 1 among others. With a lower percentage of the total, we have other causes such as tuberculosis, syphilis, rubella, radiotherapy or fibrosis to name a few. Diffuse congenital hypoplasias, such as those seen in Noonan syndrome, Sam William syndrome, Alagille syndrome, and tuberous sclerosis, to name a few, could have their embryological origin due to the overfusion of the two dorsal aortas in the 4th week of development, generating the hypoplasia of the aorta.
It is important to know the origin of middle aortic syndrome because the abdominal aorta may not be the only vessel affected. For example, in neurofibromatosis type 1 it can be associated with cerebral arteriovenous aneurysms and fistulas. In rubella it could occur simultaneously with stenotic pathology of the aortic valve. Takayasu vasculitis primarily involves the aortic arch and descending aorta among many other associations. The diagnosis of middle aortic syndrome can be through renal Doppler, tomography or resonance. Renal Doppler is the first line with a sensitivity of 90% and a specificity of 68%. This modality, despite its low specificity, is indicated to reduce exposure to rays and the use of contrast. As an advantage, MRI allows us to estimate pre- and post-stenosis flows, but if what we want is to evaluate the lesion and its characteristics, then angiography is the indicated method. If we suspect brain injuries, we should consider a tomography or brain MRI. It is recommended as initial therapy to start with a single antihypertensive agent and reach the maximum dose or adverse effect before adding another drug. In principle, enalapril or losartan should be started and diuretics should preferably be used as combined therapy. If elevated pressures persist that cannot be controlled by the use of various hypertensive drugs, surgical treatment is evaluated. If the lesion presents as an isolated stenosis, it can be treated with an isolated patch or also a bypass that bypasses the stenosis if the coarctation is very narrow. The same applies to thoracoabdominal stenosis that can be treated with a bypass that connects the thoracic cavity with the abdominal cavity. Polytetrafluoroethylene (PTFE) is preferred as a material for patches over woven or knitted Dacron. Renal or splanchnic reconstruction will be performed in which case it corresponds. For renal reconstruction, new implantation away from the diseased aorta is recommended. It is generally preferred to use homologous arterial grafts; venous grafts are not recommended due to the risk of aneurysm formation. If the stenotic lesions affecting the renal artery are multiple or this same kidney is hypotrophic, that is, 2 to 3 cm smaller than its size and non-functioning, this may be an indication for nephrectomy. Let us remember that nephrectomy is only performed if the other kidney can supply the function. An alternative to consider is kidney autotransplantation that improves hypertension and kidney function. Repair of the splenic artery can be performed with a prosthesis or implant of venous material. The objective of this article is to describe a surgical case that occurred in June 2022 at the Juan A. Fernandez general hospital in Buenos Aires City (Argentina). What makes this case very interesting is the advanced age of presentation, given that there is not much literature describing the problem presented. In general, cases of pediatric patients or patients under 25 years of age who present major symptoms are reviewed.
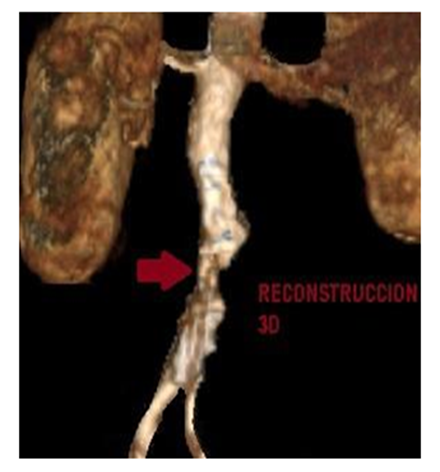
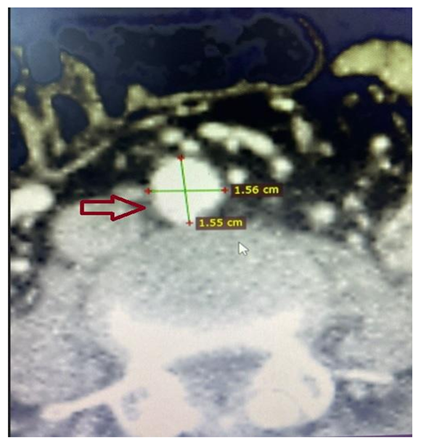
We report the case of an 81-year-old female patient with multiple clinical comorbidities including hypertension, sedentary lifestyle, smoking and osteoporosis. His surgical history highlights an appendectomy in childhood and laparoscopic cholecystectomy in 2010. Imaging showed infrarenal abdominal aortic stenosis with a concomitant stenotic lesion in the right femoral artery, both lesions diagnosed by arterial angiography. In the physical examination of both lower limbs, both femoral pulses were present with detection of a left popliteal pulse and the rest of the examination was completed with positive flow Doppler signals for the other reference points. The hospital has an operating room equipped with portable C-arm rays to perform the endovascular approach and all the necessary elements to complete the laparotomic surgical treatment. It also has a recovery room next to the operating rooms where, by protocol, the immediate post-operative period is carried out.

For this case, it was decided to hold a meeting in June 2022 where it was concluded that a hybrid approach would be the best option given the patient's age and comorbidities. For resolution, a 43 mm andrastent XL straight balloon-expandable stent was used, placed through an 8F right femoral introducer. Taking advantage of the femoral approach and exposure, the proximal anastomosis is performed, constructing a suprapatellar femoro-popliteal By Pass with an 8mm PTFE prosthesis. In the immediate post-operative examination, the presence of all pulses was evident with favorable changes in color and temperature in both limbs. As part of the institution's own hospital protocol, the patient completed the 1st postoperative day in a closed unit and after 72 hours, given the favorable evolution, hospital discharge was determined to continue outpatient follow-up in external clinics. If we look at open surgery statistics, it gives us positive results regarding the treatment of hypertension in approximately 9 out of 10 cases. This type of surgery has low morbidity and mortality in patients with good general condition. Despite presenting good results, the reoperation rate due to new stenosis is almost 10% 5-12 years after the first procedure. The endovascular approach generates a greater number of morbidities over time such as dissections, leaks, aneurysms or thrombosis of the placed stent. Therefore, it requires reinterventions and may cause restenosis. Different studies mention that 55% of patients are free of interventions after one year and 33
In conclusion, based on all the data presented and the favorable result demonstrated by the patient, we must suggest that a hybrid approach is the best way to resolve this type of pathology with the same lesions. On this occasion, the patient's characteristics, age, comorbidities and availability of resources were evaluated. The hybrid approach would be the best option because it not only improves surgical times but also the postoperative period is less aggressive for the patient. As for the follow-up by outpatient clinics, it is carried out with imaging follow-up using contrast-enhanced CT scans every month and then every six months or a year depending on kidney function.
We want to raise the following question: Is an endovascular approach or an open approach better? If both resources are available, doesn't the combination of them give the best result? And finally, when we present a patient, we see a single possibility of resolution or we recognize that we have ways of using different techniques or approaches.
All authors declare that there is no conflict of interest.
We thank all the staff from surgical instrumentation, nursing and all those who help us day by day. Without them these cases could not be carried out.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
