
Case Report | DOI: https://doi.org/10.31579/2690-4861/064
1Director Professor, Department of Obstetrics and Gynaecology, Lady Hardinge Medical College,New Delhi, India.
2Assistant professor, Department of Obstetrics and Gynaecology, Lady Hardinge Medical College,New Delhi, India.
*Corresponding Author: Kanika Chopra,Department of Obstetrics and Gynaecology, Lady Hardinge Medical College,New Delhi, India.
Citation: R Yadav, K chopra. (2020) Microperforate Hymen with Pyocolpos in a 16-Year-Old Girl: A Rare Case Report. International Journal of Clinical Case Reports and Reviews. 4(4); DOI: 10.31579/2690-4861/064
Copyright: © This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 29 September 2020 | Accepted: 20 November 2020 | Published: 23 November 2020
Keywords: microperforate hymen; pyocolpos; ascending infection; adolescent
Microperforate hymen is incomplete canalization of hymen before birth. It is a rare entity with about 20 cases reported as of now. A, 16-year-old girl, presented to Gynaecology OPD of our hospital with complaints of heavy menstrual bleeding, foul smelling discharge per vaginum and acute pain abdomen for 3 days. She attained menarche at 12 years of age. On examination, abdomen was soft and tenderness was present in suprapubic area. On local examination, hymen was intact and apparently looked imperforate. On per rectal examination, a cystic mass was felt above the anal verge bulging through the anterior rectal wall. Abdominal, trans perineal ultrasound and MRI pelvis was done and possibility of imperforate hymen was made. Under anaesthesia, a syringe- needle was put through the apparent imperforate hymen and 50 ml of pus was drained. Hymenectomy was done. Diagnosis of microperforate hymen with pyocolpos was made. At the time of follow up after 15 days, patient was fine with healthy suture line.
Our case is unique in many ways, first its delayed presentation, second the presentation of microperforate hymen with pyocolpos that was managed successfully surgically.
Microperforate hymen is incomplete canalization of hymen before birth. It is a rare entity with about 20 cases reported as of now.[1] The presentation of this anomaly, in majority patients is delayed as the small hole allows drainage of cervical or menstrual secretions, although not completely. Patients are usually susceptible to urinary tract infection, vaginal and ascending infection leading to pyocolpos. We, present this case owing to its delayed presentation as pyocoplos, inspite of normal menstrual cycles since menarche.
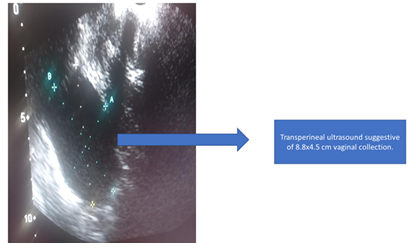
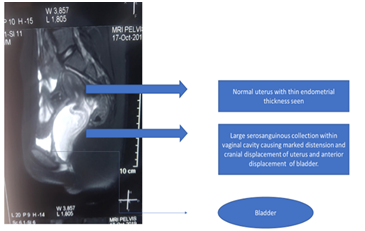
CASE: A, 16-year-old girl, presented to Gynaecological OPD of Lady Hardinge Medical College with complaint of heavy menstrual bleeding during periods followed by foul smelling discharge per vaginum. She complaint of acute pain abdomen three days back, when she went to hospital nearby. She was given I/V analgesics. Ultrasound pelvis and later MRI pelvis was done and diagnosis of hematocolpos was made. Figure 1, 2. She was then, referred to our hospital for further management.
She attained menarche at 12 years of age. She used to bleed for 4-5 days followed by spotting for 5 days, not associated with dysmenorrhea and cycles were every 40-45 days. There was no significant past or family history.
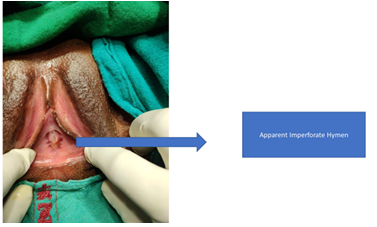
On examination, patient was average built and there was no pallor, icterus, cyanosis, pedal edema or generalised lymphadenopathy. Her vitals were normal (pulse rate, blood pressure and temperature of 96 beats per minute, 112/76mmHg and 98.8-degree Fahrenheit). Chest and cardiovascular system w normal. Her secondary sex characters were well developed (Breast examination was done and was tanner stage 4. Pubic and axillary hair were present). On per abdominal examination, abdomen was soft with a tender mass palpable corresponding to 12-14 weeks gravid uterus. No other organomegaly was palpable. On local examination, external genitalia were normal looking. On separating the labia, urethral meatus was normal looking and hymen was intact and apparently looked imperforate as seen in figure 3. No bulge was seen at hymen. On asking the patient to cough, foul smelling discharge was seen coming out through a very small pin point hole at 1 ‘o clock position. On per rectal examination, a cystic mass was felt above the anal verge through the anterior rectal wall.
Her baseline investigations were haemoglobin 11.4gm%, total leukocyte counts 18,380/ microlitre, Neutrophil/ lymphocyte- 90.7/9.5, erythrocyte sedimentation rate 73mm, platelet count 2.98 lakh/ microlitre, random blood sugars 110mg/dl. Liver and kidney function tests were normal. Urine routine microscopy and culture sensitivity was normal. Ultrasound pelvis on day 2 of this cycle, was suggestive of normal size uterus with a central endometrial thickness of 5.1mm with vaginal dilation due to collection of echogenic free fluid within measuring 8.4cm x 4.5 cm. Bilateral ovaries were normal looking. MRI pelvis was also done to confirm the diagnosis and possibility of imperforate hymen was made.
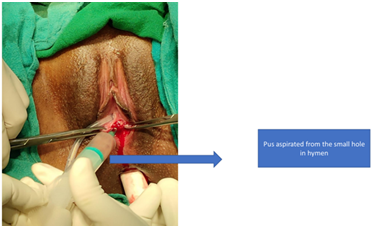
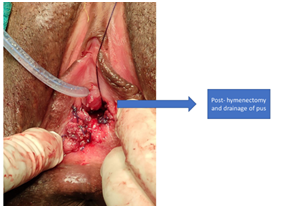
Patient was admitted and started on antibiotics and analgesics. After written and informed consents, patient was planned for examination under anaesthesia and proceed. Under anaesthesia, patient was catheterized and findings confirmed. Through the hymen, a needle was inserted, pus aspirated and sent for culture sensitivity, figure 4. Cruciate incision was then given in the hymen and around 50 ml of pus was drained. Hymenectomy was done and edges of vaginal mucosa was sutured at introitus with interrupted sutures, figure 5. Betadine washing of vagina was done. Hemostasis ensured. Patient stood the procedure well. Catheter was removed on POD 2 and discharged on POD 3 in a stable condition. At the time of follow up after one week, patient was fine with healthy suture line.
Discussion
Hymen is a thin membrane present at the distal part of vaginal canal and is formed by the fusion on sinovaginal bulb and urogenital sinus. It canalizes just before birth. Its canalization allows cervical secretion and menstrual blood to come out. Complete or incomplete canalization leads to pent up of these secretions and thus varied presentation.
Imperforate hymen is seen in 0.1% girls and is associated with cyclic pain abdomen, primary amenorrhea with well-developed secondary sexual characters and on examination a hymenal bulge is seen.[2] Such patients usually presents at puberty, but can also present in early years of life as mucocolpos, recurrent urinary tract infections and urinary retention.[3]
Microperforate hymen is characterised by incomplete canalization of hymen before birth. It usually exists as an isolated anomaly. Rarely, it is seen with bifid clitoris, hypoplastic kidneys, duplicate ureter and anorectal malformation.3 Patients with this anomaly are highly susceptible to urinary tract infection, vulvovaginitis and ascending infections.[3] Presentation in these patients are usually delayed, and depends largely on the hole size. Patients may present with prolonged light bleeding post menstrually and in acute cases as abdominal pain, urinary retention or dysuria and pyocolpos leading to malodorous vaginal discharge with fever similar to our case. Pyocolpos or pus-filled vagina results due to ascending infection and invasion of entrapped vaginal secretions. [4] It is a surgical emergency in majority. If delayed, due to any reason, pyoslpinges, pelvic abscess, sepsis, vaginal scarring and vesicovaginal fistula can result. [5, 6] These patients may also prevent in later age with inability to have vaginal intercourse and conceive. But there are cases reported of patient conceiving in cases with microperforate hymen as well. [7, 8]
Patient has to be evaluated completely in order to rule out differentials of imperforate hymen, vaginal atresia or agenesis, labial adhesions and transverse vaginal septum. [4, 5]
Ultrasound abdomen and pelvis is the modality of choice for diagnosis. MRI can also be done to confirm the anomaly and plan surgical procedure accordingly as in our case.
Few numbers of cases are reported till now in literature. Our case is unique in many ways, first its delayed presentation, second the presentation of microperforate hymen with pyocolpos that was managed successfully surgically.
Conclusion:
Early recognition of varied presentations of this rare anomaly may prevent any complications like pyocolpos as in our case. Our patient presented with acute pain abdomen that led us to the diagnosis. But patients presenting with any abnormality in menstrual cycle in their early reproductive years, should be evaluated completely including a thorough external genitalia examination to ensure early diagnosis of this rare hymenal anomalies and thus timely management.
Conflict of interest: None
Acknowledgement: None
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
