
case report | DOI: https://doi.org/10.31579/2690-1897/190
1Gastroenterology, Department in Nini University Hospital, clinical instructor of medicine at university of balamand, Lebanon.
2Professor of anatomical pathology, Lebanese university, Lebanon.
3Lebanon, Professor of gastroenterology and hepatology, Lebanese University, Lebanon.
*Corresponding Author: Rose Al Bacha, Gastroenterology, Department in Nini University Hospital, Clinical educator at university of balamand, Lebanon.
Citation: Rose Al Bacha., Claude Ghorra., Joseph Bou Jaoude, (2024), Metastasis of Ewing Sarcoma to the Pancreas: Case report and Literature Review, J, Surgical Case Reports and Images, 7(4); DOI:10.31579/2690-1897/190
Copyright: © 2024, Rose Al Bacha. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 15 April 2024 | Accepted: 29 April 2024 | Published: 06 May 2024
Keywords: ewing sarcoma family of tumors; skeletal ewing’s sarcoma; ewing sarcoma
Introduction: The Ewing sarcoma family of tumors (ESFT) represents a group of classic Ewing’s sarcoma of bone, extra skeletal Ewing’s sarcoma (EES), Askin tumours of the chest wall and primitive neuroectodermal tumours of bone or soft tissues. However, the existence of metastatic disease is the most crucial prognostic marker. While Ewing sarcoma is primarily a bone cancer, it rarely metastasize to the pancreas with 4 reported cases in the literature.
Case presentation: We represent a case of a 38 year old male patient diagnosed with Ewing sarcoma of the bone that developed acute pancreatitis after 6 months. MRI showed a well circumscribed mass measuring 14 mm is present at the junction of the body and tail. FNA and core biopsy was positive for a small blue cell tumor and positive for CD99. These findings were consistent of extension of Ewing sarcoma. Patient was unresponsive to chemotherapy , disease progression and died. . Our case emphasizes the rarity of pancreatic ES metastases, since only four previous cases have been documented in the literature. The necessity of advances in therapy is crucial.
The Ewing sarcoma family of tumors (ESFT) represents a group of classic Ewing’s sarcoma of bone, extra skeletal Ewing’s sarcoma (EES), Askin tumours of the chest wall and primitive neuroectodermal tumours of bone or soft tissues [1]. The translocation t(11; 22) (q24; q12), which produces the EWS/FLI1 fusion gene is the genetic bases of ESFT [2]. The tumor cells are an undifferentiated small round blue cell with a low mitotic index [3].
Ewing sarcoma (ES) of the bone is the second most frequent malignant bone cancer in adolescents and young adults after osteosarcoma4. Whereas EES is an uncommon condition that can appear anywhere in the soft tissues but can alter the cortex of nearby bone. The trunk, extremities, and retroperitoneum are the areas where it occurs most frequently [5].
However, the existence of metastatic disease is the most crucial prognostic marker, and even patients who are diagnosed with locally limited cancer are at significant risk of developing metastatic disease while receiving local therapy [6].
While Ewing sarcoma is primarily a bone cancer, it rarely metastasize to the pancreas [7]. In this case report, we present a 38-year-old man with cytogenetically confirmed metastatic ES to the pancreas.
A 38-year-old male, was initially diagnosed with EES of the soft tissue on the plantar surface of the left foot (8*3,6cm) with immunochemistry showed expression of CD99. He underwent surgical resection below knee amputation with biopsy showed small round blue cell destructing the bone and infiltrating the soft tissue.
After 6 months he developed mild acute pancreatitis with CT scanner of the abdomen showed edematous pancreatitis of the tail of the pancreas. MRI (figure 1) showed a well circumscribed mass measuring 14 mm is present at the junction of the body and tail. It is of high signal intensity on T2 low T1 with minimal internal septal enhancement. It is communicating with the pancreatic duct which distally in the tail is at the upper limits of normal measuring 3 mm.
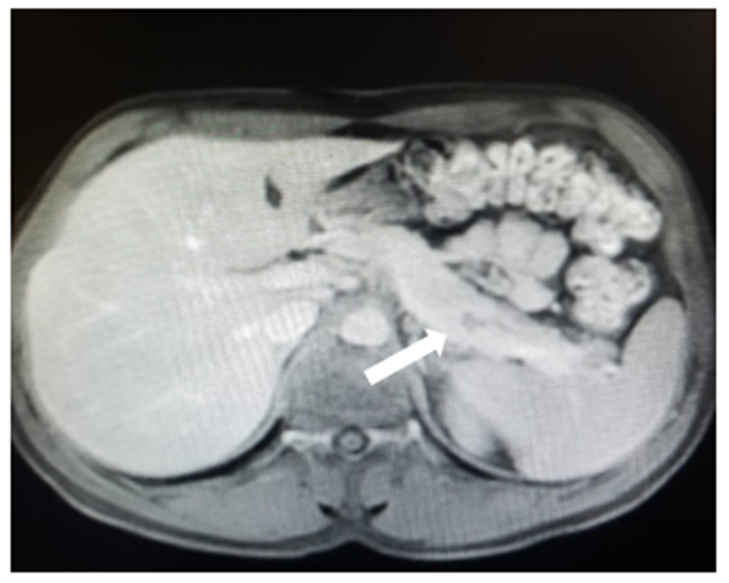
Figure 1: Well circumscribed mass measuring 14 mm at the junction of the body and tail of the pancreas (white arrow).
Echo endoscopic ultrasound showed a 13 mm cystic lesion obstructing the wirsung (figure 2). FNA and core biopsy was positive for a small blue cell tumor and positive for CD99. These findings were consistent of extension of Ewing sarcoma (figure 3).
He was then treated with chemotherapy Docetaxel based but unfortunately patient had disease progression, developed lung metastasis with recurrent pleural effusion and died for pulmonary failure.
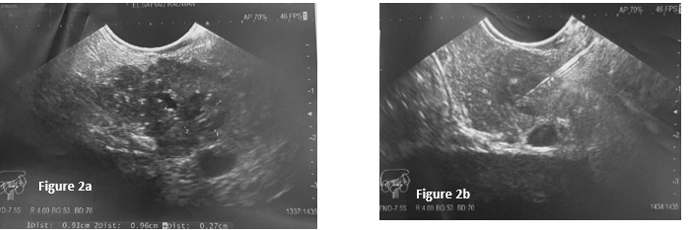
Figure 2a: 13 mm cyctic lesion obstructing the wirsung which is dilated upstream.
Figure 2b: FNA needle 22G inside the lesion.
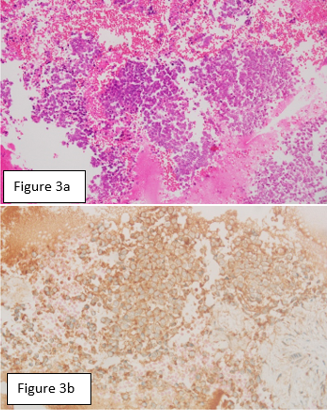
Figure 3a: Small round blue cell in H&E stain.
Figure 3b: Cells showing diffuse membranous expression of CD99 on immunohistochemistry
Pancreatic metastasis are rare, accounting for only 2% of all pancreatic cancer [8]. The primary tumors that metastasize frequently to the pancreas are lung cancer, renal cell carcinoma, breast cancer, melanoma and colon cancer [9].
Ewing sarcoma is a rare bone tumor and depending on whether metastases were present at diagnosis, patients with ESFT have considerably different five-year overall survival rates (OS) ranging from 70% if localized to 9–41% for metastatic disease10.
Hyma et.al reviewed a 39 cases of ESFT involving the pancreas, with only four of them being metastatic lesions11. The 4 cases were younger then 30 years of age, with two of them testing positive for CD 99 and one testing positive for PAS in terms of pathologic features. There is also a male predominance with only one female case.
The diagnosis of pancreatic metastases can be made safely and effectively with endoscopic ultrasonography (EUS) with confirming the diagnosis using immunohistochemistry9. Out of the 39 cases described in the literature, CD99 is the most frequently reported marker linked to ES. Other related markers that are less precise are synaptophysin, vimentin, and neuron-specific antigen [11].
Radiation, chemotherapy, and surgical resection were used to treat these individuals; however, the prognosis was poor with two resulting in death from the disease. Similarly our case was young male patient with positive CD 99 in terms of pathologic features.
The prognosis for ESFTs has significantly improved after multiagent chemotherapy was added to surgery and/or radiation treatment. Children with localized illness who get combined-modality treatment had a 65% to
70% progression-free survival rate (PFS) [12]. While The EURO-EWING 99 trial demonstrated that patients who received local treatment for both the primary and metastatic disease had a three year event-free survival rate that was significantly higher compared to patients who only received local treatment for the primary or metastatic disease [13].
In conclusion, we present a rare case of ES metastasis to the pancreas in a 38-year-old male with prior diagnosis and treatment of ES of the left foot unresponsive to chemotherapy. Our case emphasizes the rarity of pancreatic ES metastases, since only four previous cases have been documented in the literature. Pancreatic metastasis can be diagnosed with immunohistochemistry stain, with CD99 being the most frequently found marker linked to ES.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
