
Case Report | DOI: https://doi.org/10.31579/2690-1919/378
1Cancer Research Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran
2Department of pathology, Shohada-e-Tajrish Educational Hospital, School of Medicine, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
*Corresponding Author: Efraín Sánchez González, Cancer Research Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran
Citation: Atieh Akbaria , Parisa Behravana , Azadeh Rakhshanb , Mohammad Esmaeil Akbaria, (2024), Metaplastic breast carcinoma with squamous differentiation: report of nine cases, J Clinical Research and Reports, 16(1); DOI:10.31579/2690-1919/378
Copyright: © 2024, Mohammad Esmaeil Akbaria. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 14 May 2024 | Accepted: 24 May 2024 | Published: 05 June 2024
Keywords: Breast cancer; squamous;metaplastic; treatment; carcinoma
Breast metaplastic carcinomas are a rare form of malignancy that exhibit epithelial and sarcomatoid components, including primary squamous cell carcinoma. Primary breast SCC and tumors with squamous differentiation are subtypes of breast metaplastic cancer. The prevalence of primary squamous cell carcinoma (PSCC) of the breast is estimated to be between 0.06% and 0.2% of all breast cancers, and less than 0.1% of invasive breast cancers. At our Cancer Research Center, we have managed and treated 9 patients with PSCC aged between 24-67, and all of them except one were of reproductive age, out of a total of 4000 breast cancer cases during the last two years.
Metaplastic carcinoma of the breast refers to a heterogeneous group of rare malignant tumors that have mixed epithelial and sarcomatoid components, including primary squamous cell carcinoma.[1] Primary squamous cell carcinoma (PSCC) of the breast is an extremely rare type of invasive breast carcinoma, comprising approximately 0.06-0.2% of all breast cancers and less than 0.1% of invasive breast cancers.[2]PSCC of the breast is an aggressive form of cancer that is marked by larger tumors, quick growth, frequent recurrences, and a high death rate.[3]Although this condition often manifests in postmenopausal women, it has also been recorded in young, pregnant, and breastfeeding females.[4]
The treatment outcomes for patients with breast squamous cell carcinoma (SCC) are uncertain. Currently, the ideal therapy for breast SCC is not known, as therapeutic choices have been based on experience with breast infiltrating ductal carcinoma (IDC). This means that the prognosis and optimal treatment for breast SCC are still a matter of debate.[5]
The most thoroughly reported form of pathogenesis is complete metaplasia of the ductal epithelium.[6]
Here, we describe nine patients with breast PSCCs who were treated and monitored at our cancer research center.
In the last two years, our center has served as a referral center for breast cancer patients in the country. During this time, we have treated approximately 4,000 patients. Out of these patients, only nine were diagnosed with metaplastic carcinoma of the breast, and they received surgical and follow-up care at our center. A summary table of the patients' clinical and pathological information is included in the case report section, just before the beginning of the discussion. (Table 1), as well as the detailed and comprehensive explanation table of the patients’ information is uploaded in the supplementary file (Table 2)
All the patients in this study, except one, were of reproductive age and between the ages of 24 and 67, having palpable masses in different breast areas. One of the patients (No. 8) was 34 weeks pregnant when she was diagnosed with cancer, and she had a cesarean section at 38 weeks due to this issue.Two patients had diabetes, and one had a history of neurofibromatosis, but none of the other 6 patients had underlying disorders. Immunohistochemistry (IHC) of five patients was triple negative, two of the patients were HER2-enriched (positive for human epidermal growth factor receptor 2 (HER2) and negative for estrogen receptor (ER) and progesterone receptor (PR)), and one of the patients was positive for ER/PR and negative for HER2. In the majority of immunohistochemistry studies, PSCC is p63 positive; Cytokeratin(CK) 5/6 positive; and ER, PR, and HER2 negative. IHC study for ER, PR, and HER2 was performed. Staining with ER [ Rabbit anti-human Estrogen Receptor Monoclonal antibody, clone SP1] and PR (Rabbit anti-human Progesterone Receptor Monoclonal antibody, clone 16) were considered negative if less than 1% of tumoral cells showed nuclear positivity in the presence of appropriately stained internal control.
IHC Staining for HER2 (Rabbit anti-human c-erbB2 monoclonal antibody, clone SP3) was interpreted based on the intensity and completeness of membrane staining. The result was considered negative (score 0 or score 1) if there was no staining or incomplete membranous staining that was faintly / barely perceptible.Before determining the operation date, the patients had a series of exams, including chest, and abdominal-pelvic computed tomography (CT) scans, to rule out the main site/metastasis and staging of the disease. The patients were scheduled to have cancer surgery (as described in detail in the table2), which was performed roughly two weeks later. Three patients were scheduled for modified radical mastectomy (MRM) and six of the patients had breast-conserving surgery (BCS). One of the patients underwent BCS surgery in another center in 1997(No.4), with the pathology of Invasive ductal carcinoma (IDC). Then in June 2014, she came to our center with a palpable mass at the site of the previous surgery and local recurrence and lung metastasis. The patient underwent a biopsy and became a candidate for surgical resection with a pathology report of metaplastic carcinoma.
The patients returned for a follow-up appointment around one week following surgery, and there was no specific problem, and the pathology results are provided in the supplementary table 2. Due to the contradiction with the patients' history and sonographies, as well as the rarity of SCC in the breast, the original pathohistological slides were reviewed by experienced breast pathologists in this facility for the present study,(confirming the diagnosis), which was SCC.
Seven of the patients were candidates for 6 cycles of paclitaxel and carboplatin-based adjuvant chemotherapy 3 weeks after surgery. Two of the patients underwent pre-operative neoadjuvant chemotherapy and then became a candidate for surgery.
All the patients were eligible for full breast irradiation. One of the patients received letrozole medication due to the presence of positive hormone receptors in IHC following surgery but the rest of the patients didn’t get hormone therapy due to negative hormone receptors. Other case-specific factors, such as tumor and axillary lymph node features on physical examination, sonography, and mammography, as well as the kind of surgery, therapy, and patient follow-up, are covered in length in the Table 1
Summary report of the demographic and pathological information of the patients
| Pathological and clinical characteristics | Cases from 9 patients(% ) | |||
| Family history | 4 (44) Positive | 5 (56) Negative | ||
| Physical examination | 9 (100) Palpable | 0 (0) Non-Palpable | ||
| Axillary lymph node | 6 (67) Positive | 3 (33)Negative | ||
| Size | 4 (44) (>4cm) | 5(56) (<4cm> | ||
Chemotherapy
| 2(22) Adjuvant Chemotherapy | 7(78)Neoadjuvant Chemotherapy | ||
| Surgery method | 3(33)BCS+SLND | 3(33)MRM | 3(33)BCS+ALND | |
| Grade | 0 (0)Grade 1 | 1(11)Grade 2 | 8(89) Grade 3 | |
| Lymph | 7(78)(N0) | 0 (0) (N1(1-3)) | 0 (0) (N2 (4-6)) | 2(22) (>N2) |
| ER*1 | 1(11) Positive | 8(89) Negative | ||
| PR*2 | 1(11) Positive | 8(89) Negative | ||
| HER2*3 | 2(22) Positive | 7(78)Negative | ||
| ki67 | 4(44) (<40> | 2(22) (>40%) | 3 (34) N/A*4 | |
Abbreviations:*1 ER: estrogen receptor /*2 PR: progesterone receptor /*3 HER2:human epidermal growth factor receptor 2 /*4 N/A: not available
Detailed report of demographic and pathological information of the patients
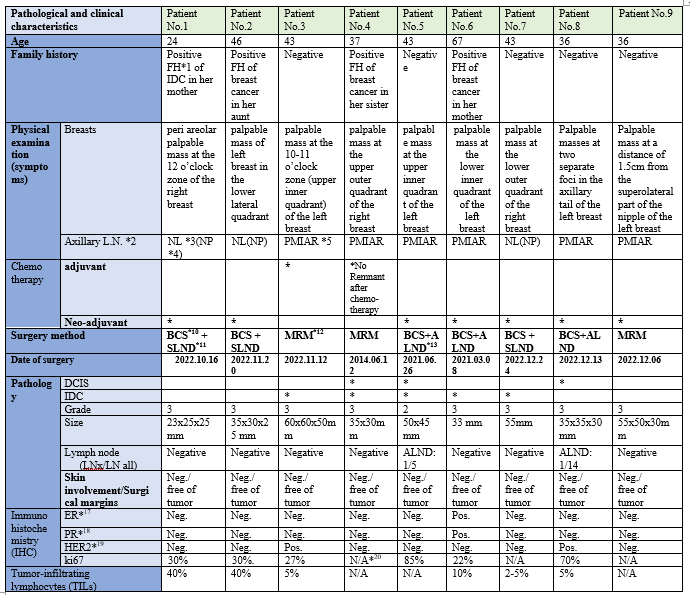
Abbreviations: *1FH: family history /*2 L.N.: lymph node /*3 NL: normal /*4 NP: not palpable /*5 PMIAR: palpable mass in the axillary region /*6 USG: ultra sono graphy /*7 CNB: core needle biopsy /*8 IDC: Invasive ductal carcinoma /*9 DCIS: ductal carcinoma in situ /*10 BCS: breast-conserving surgery /*11 SLND: sentinel lymph node dissection /*12 MRM: modified radical mastectomy /*13 ALND: axillary lymph node dissection /*14 SCC: squamous cell carcinoma /*15 DCIS: ductal carcinoma in situ /*16 NST: not specified tumor /*17 ER: estrogen receptor /*18 PR: progesterone receptor /*19 HER2:human epidermal growth factor receptor 2 /*20 N/A: not available.

Figure 1: Gross examination of the excised mass showing a solid and cystic tumor of patient No2

Figure 2: Metaplastic carcinoma of squamous cell carcinoma type of patient No.1 - Low power image shows sheets of atypical squamous epithelial cells.
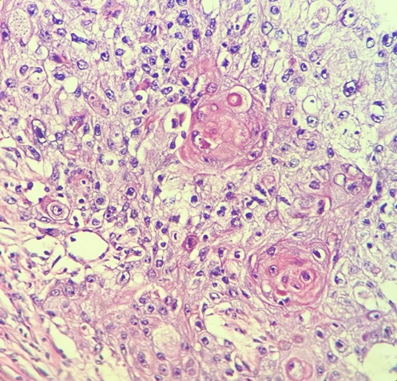
Figure 2: Metaplastic carcinoma of squamous cell carcinoma of patient No2 - High power image shows atypical squamous epithelial cells with vesicular nuclei, nuclear pleomorphism, increased mitotic activity, and keratin pearl formation.
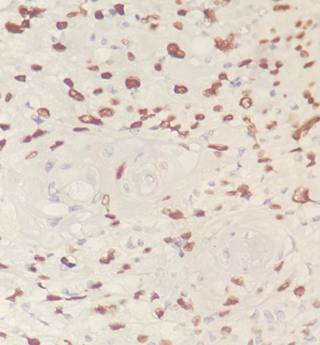
Figure 3: IHC staining for P63 reveals nuclear staining in tumoral cells in favor of squamous differentiation.
The specific etiology and pathophysiology of breast PSCC are still unknown, and there are several theories on the subject. Some have hypothesized that it develops from squamous metaplasia in benign breast disorders such as cysts, chronic inflammations, abscesses, fibro adenomas, or in association with breast implants.[7]
Metaplastic carcinoma is a heterogeneous group of breast carcinoma in which the neoplastic epithelial components differentiate into non-glandular (squamous or mesenchymal) elements and include metaplastic carcinoma with heterologous mesenchymal differentiation, spindle cell carcinoma, fibromatosis-like metaplastic carcinoma, metaplastic carcinoma with osteoclast-like giant cells, squamous cell carcinoma, low-grade adenosquamous carcinoma, and mixed metaplastic carcinoma.
Metaplastic SCC may be pure or mixed with other types of metaplastic carcinoma. Primary Squamous cell carcinoma of the breast should be distinguished from SCC of cutaneous origin and metastatic SCC ( e.g. from lung and cervix). [8]
Extramammary SCC and primary SCC are the two types of breast SCC. Whenever SCC is found in the breast, the lesion's etiology and the origin or the primary site should be investigated. This is because extra mammary SCCs tend to metastasize to the breast, with the lung, esophagus, cervix, and urinary bladder being the most common primary locations.[9] In contrast to IDC, primary breast SCC can spread to distant organs without lymph node involvement. [10]
If we cannot find a cause for breast SCC, it is the primary type of SCC. In our study, all of the reports of chest and abdominopelvic CT scans were normal, and we didn’t find any origin of metastasis in the assessments in all nine patients.
Few occurrences of SCC in young females have been documented in the medical literature.
In a 2017 study of 445 patients with breast SCC, in which data were extracted from the National Cancer Institute’s Surveillance, Epidemiology, and End Results Registry in USA, to identify women diagnosed with squamous cell carcinoma of the breast between 1998 and 2013, the median age at diagnosis was 67 years (range: 26–99 years), with the highest incidence recorded in the age group of 80–84 years, indicating that breast SCC is more prevalent in older women.[2] However, in our study, the eight patients are in their reproductive period. One reason may be that the age of breast cancer in our country is a decade lower than the average age of its occurrence in the Western world.[11]
Typically, these tumors grow rapidly and exhibit necrotic, hemorrhagic foci, cyst development, and inflammatory changes.[12]
Since squamous cell carcinomas are less likely to disseminate lymphatically than adenocarcinomas [13], we conduct sentinel lymph node biopsy (SLNB) if the patient does not have a noticeable lymph node on examination and imaging.
In imaging, Ultrasound Sonography (USG) detects solid, hypoechogenic masses with complicated cystic components[14], similar to our patients’ USG reports.
Physically, squamous cell carcinoma looks the same as other types of breast cancer, except that sometimes large, keratin-filled cyst forms in the middle. However, it is similar to other types of breast tumors in examination and radiologic and mammographic features. Microscopically, the majority of cases appear to exhibit squamous metaplasia in invasive ductal carcinoma, suggesting that squamous cell carcinoma is a subtype of metaplastic carcinoma. infrequently accompanied by a conspicuous myxoid stroma. [15] Therefore, only a bulk biopsy can confirm a patient's diagnosis.
Although all patients in previous studies were negative for estrogen and progesterone hormone receptors, one of our patients (patient No.6) was positive for hormone receptors despite the recheck.
Similar to our study, the IHC of all patients was triple negative except patients No. 3 and No. 8 with positive HER2 but negative ER/PR, and patient No. 6 with positive ER/PR and negative HER2. This helps distinguish it from ductal carcinoma with localized squamous metaplasia.[16]
For breast SCC, the appropriate therapy method is yet uncertain. As the initial treatment for this condition, studies indicate that surgery should take precedence over chemotherapy.[17]
The majority of studies concluded that patients treated with breast-conserving surgery had comparable local control and survival outcomes to those treated with mastectomy.[18, 19]
Three of our patients received BCS + SLND, three received BCS + axillary lymph node dissection (ALND), and three received modified radical mastectomy (mastectomy + ALND). Dissected sentinel lymph nodes or axillary lymph nodes in all of these patients were reactive and negative for malignancy except for 2 patients.
Advanced SCC of the breast is not responsive to neoadjuvant chemotherapy.[20-22] It is debated which chemotherapy treatment is optimal. Chemotherapy with anthracycline, cisplatin, or Cyclophosphamide/methotrexate/fluorouracil (CMF) may be useful.[20]
In a recent multivariate analysis, postoperative radiation improved the overall survival of breast SCC patients. This is debatable because there are a lot of local relapses in irradiated areas, which shows that breast SCC is resistant to radiation.[23, 24]
Due to the aggressive nature of the tumor, however, our patients get radiation following the completion of chemotherapy, and it is intended to reevaluate the response to treatment following the conclusion of the treatment regimen. The patients tolerate chemoradiotherapy well or have tolerated it well and are doing well.
The absence of hormone receptors in the majority of malignancies causes to be endocrine therapy useless. These malignant tumors had a 5-year survival rate attributable to the underlying etiology of 63.5%. Age and tumor or nodal stage at presentation are independently predictive of a worse outcome in the affected area.[2] Although the prognosis is controversial, the majority of studies indicate that the disease is aggressive, with frequent local and distant relapses and mortality.[25]
Hennessy et al. discovered that 26% of 32 breast SCC patients with localized illness survived five years without recurrence. 40% lived for five years, with a median survival of 37 months (range 12-108 months). 14 months was the median survival following relapse (range 2-86 months).[10]
Most cancer recurrences occur in the first five years, so regular follow-ups should be considered for patients in the first five years.[26] Patient No. 4 has no recurrence after 9 years of follow-up, and patients No. 5 and 6 did not have any pathological findings after two years of surgery and treatment. Other patients have recently finished their adjuvant chemotherapy treatment and are undergoing follow-up.
The case series discussed here is noteworthy because it chronicles the experiences of women in their fertile years who were diagnosed with primary SCC of the breast. This indicates that this disease can occur at a young age. Specialized assessments are necessary for breast cancers, cystic breast masses, and tumors with rapid growth. As this is a rare disease, recurrences usually take place within the first five years. Therefore, it is important to consider regular follow-ups during the first five years for patients.
This article is taken from the cancer research center registry for registering information on patients with breast cancer, which was supported by the deputy of research and technology at Shahid Beheshti University of Medical Sciences (http://dregistry.sbmu.ac.ir).
None.
Mohammad Esmaeil Akbari was involved in the counseling and treatment of the patient. Azadeh Rakhshan examined and interpreted the pathology. Atieh Akbari and Parisa Behravan collected all the required case information, images, slides, and reports and contributed to writing manuscripts. All the authors reviewed the literature and contributed to both writing and editing the manuscript. All authors read and approved the final manuscript.
Ethical Approval
The patients were asked to sign an informed consent form and all identity and personal information of the patients remained protected.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
