
Review | DOI: https://doi.org/10.31579/2768-0487/182
1Gynecology obstetrics residents at Chu Ibn Rochd Casablanca, Morocco.
2Assistant professor of Gynecology obstetrics at Chu Ibn Rochd Casablanca, Morocco.
3Professors of Gynecology obstetrics at: Gynecology Department A, Chu Ibn Rochd Casablanca, Morocco.
*Corresponding Author: Fatim Zohra El Hachami., Gynecology obstetrics residents at CHU IBN ROCHD Casablanca, Morocco.
Citation: Madyani H., El Hachami.Fz., Imami.Y., Laaliaoui.A., Taous.C., et al, (2025), Meningioma and Pregnancy: A Case Report and Literature Review, Journal of Clinical Surgery and Research, 6(6); DOI:10.31579/2768-0487/182
Copyright: © 2025, El Hachami.Fz. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 04 August 2025 | Accepted: 20 August 2025 | Published: 28 August 2025
Keywords: meningioma; pregnancy; surveillance; surgery; radiotherapy
Common symptoms include headaches, cranial nerve deficits, seizures, cognitive disturbances, neurological impairments, dizziness, balance disorders, sensory disturbances, exophthalmos, or syncope (22). Diagnosis relies on neuroimaging, using CT scan or MRI with contrast enhancement. Meningiomas typically appear as round, solitary masses arising from the dura mater, with intense enhancement after contrast injection.
Meningiomas are intracranial tumors more frequently observed in women and are often promoted by pregnancy. Cyproterone acetate, a synthetic progestin with anti-androgenic effects, has been associated with an increased risk of meningioma, in a dose-dependent manner. This effect has also been reported with other progestins (chlormadinone acetate, nomegestrol acetate). The diagnosis of meningioma involving the eye should be made as early as possible due to the associated visual and potentially life-threatening risks. Our case further highlights the role of pregnancy in the progression of meningioma, which must systematically be considered in any pregnant woman presenting with visual impairment and ocular involvement. [1] In the presence of any optic neuropathy, a thorough and systematic ophthalmologic examination must be performed, followed by cerebral and orbital imaging. This rigorous approach helps to prevent diagnostic errors that could lead to serious consequences.
Observation:
A 20-year-old female patient, with no significant past medical history, pregnant at 27 weeks of gestation, presented with symptoms of increased intracranial pressure (ICP) evolving over two months. The initial presentation included vomiting and headaches, which later worsened with a decrease in visual acuity, without other associated signs. On admission, clinical examination found a drowsy patient with a Glasgow Coma Scale score of 13/15, hemodynamically and respiratorily stable. Her visual acuity was limited to disoriented light perception. The afferent photomotor reflex was impaired, and fundoscopic examination revealed a mass compressing the optic chiasm and fully encasing the right optic nerve in its intracranial portion. A non-contrast orbital and brain MRI showed a large extra-axial lesion with a broad base of attachment to the sphenoidal jugum, extending to the suprasellar and right petroclival regions, measuring 64 x 48 x 42 mm at the time of examination. The mass compressed the right temporal and basifrontal lobes, the mesencephalon, and the right diencephalon, with leftward displacement of midline structures and signs of early subfalcine herniation. The lesion also encased and narrowed the caliber of the M1 segment of the middle cerebral artery, the posterior communicating artery, and the right optic nerve.
In summary: the MRI findings were consistent with a large suprasellar extra-axial mass measuring 67 x 49 x 52 mm, causing right temporal and central subfalcine herniation, suggestive of a meningioma.
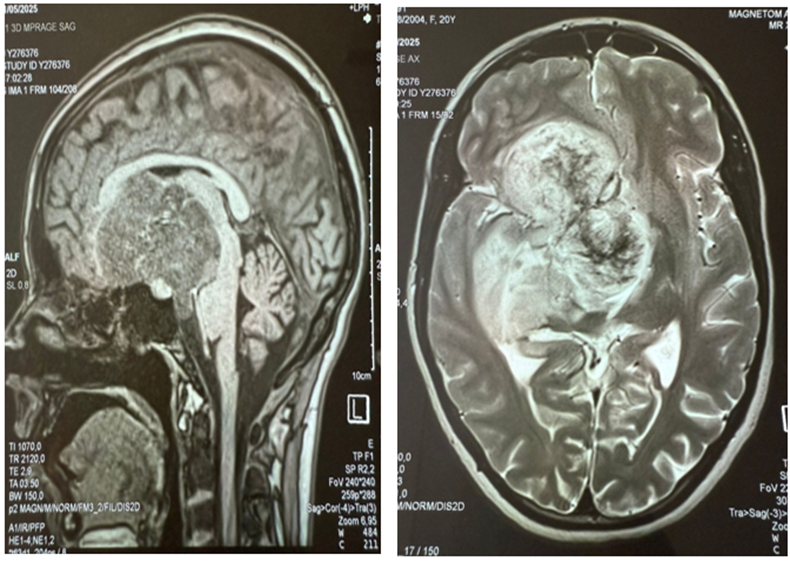
Figure 1-2: Suprasellar extra-axial meningioma causing a mass effect measuring 67 x 49 x 52 mm.
The patient’s clinical course was marked by a worsening of her neurological status, prompting a follow-up brain MRI, which revealed an increase in tumor size, reaching 9 cm in its longest axis. Given this progression, a multidisciplinary discussion led to the decision to proceed with fetal extraction, followed by a neurosurgical intervention scheduled for the second postpartum day (D2). Delivery was performed at 34 weeks and 3 days of gestation. However, the patient developed hemodynamic instability, which worsened and progressed to brain death, followed by cardiopulmonary arrest on the fourth day after the cesarean section (D4).
Meningiomas are slow-growing tumors originating from the meninges and account for approximately 40% of primary central nervous system tumors [15]. They are generally histologically benign and are managed through radioclinical follow-up with MRI or surgical excision, often with favorable outcomes. However, in certain cases, these tumors can exert mass effect on brain tissue, leading to focal neurological deficits, headaches, or seizures. The onset of neurological symptoms typically warrants surgical intervention [16]. Approximately 20% of meningiomas exhibit more aggressive behavior, which complicates both prognosis and therapeutic decision-making. The clinical presentation of meningiomas is often nonspecific, depending on the tumor’s location, and usually relates to compression of adjacent neural or vascular structures. Common symptoms include headaches, cranial nerve deficits, seizures, cognitive disturbances, neurological impairments, dizziness, balance disorders, sensory disturbances, exophthalmos, or syncope [22]. Diagnosis relies on neuroimaging, using CT scan or MRI with contrast enhancement. Meningiomas typically appear as round, solitary masses arising from the dura mater, with intense enhancement after contrast injection. On MRI, they are usually iso-intense on T1-weighted images, iso- or hyperintense on T2 or FLAIR sequences, with homogeneous and strong gadolinium enhancement. The so-called "dural tail sign" (a dural thickening adjacent to the tumor) is observed in 72% of cases on T1 post-contrast MRI. However, this sign is not specific to meningiomas and can be found in other
dural tumors [23]. CT scans may also reveal intratumoral calcifications or bone changes (hyperostosis or bone invasion). Meningiomas are more frequent in women, with a female-to-male ratio of 2.3:1 across all ages, reaching 3.15:1 in women of reproductive age (3.8). Their size tends to increase during the luteal phase, during ovarian stimulation (e.g., for assisted reproduction), or during pregnancy, and to regress spontaneously postpartum [4,5]. A moderate association has also been observed between meningiomas and breast cancer [7]. The role of progesterone in the growth of meningiomas has been biologically confirmed [17,18], with approximately two-thirds of tumors expressing progesterone receptors [19]. This explains the volume increase during pregnancy and spontaneous regression after delivery [20,21]. Estrogen and androgen receptors have also been identified [6]. Hormone replacement therapy is associated with a moderately increased risk of meningioma (relative risk 1.35) [11]. Furthermore, progesterone intake is considered an independent risk factor [9,10]. The predominant role of progesterone is supported by the significantly increased risk associated with high-dose synthetic progestins, such as cyproterone acetate (CPA), chlormadinone acetate (CMA), and nomegestrol acetate (NOMAC) [11,13,14]. Recent advances in genetics and molecular biology have identified new prognostic markers and potential therapeutic targets, particularly in tumors refractory to surgery and radiotherapy. The management of meningiomas is individualized and includes radioclinical surveillance, surgery, radiotherapy (conventional or stereotactic), and, less commonly, chemotherapy. Surgical excision is the treatment of choice for symptomatic, progressive, or neurologically threatening lesions. Complete resection leads to cure in 70–80% of cases [12]. However, surgery may be challenging, especially in skull base locations or in cases involving critical neurovascular structures. Numerous clinical trials are ongoing to identify effective medical treatments, particularly for aggressive meningiomas. These studies will also help to clarify the role of radiotherapy, especially for atypical forms. Metabolic radiotherapy protocols targeting somatostatin receptors (e.g., Lutathera) are also under development.
Meningiomas can grow during pregnancy, primarily under the influence of hormones, particularly progesterone. The decision between simple monitoring and surgical intervention depends on the tumor size, the presence of neurological symptoms, and the gestational age. An appropriate multidisciplinary approach is essential to ensure the safety of both the mother and the fetus.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
