
Review Article | DOI: https://doi.org/10.31579/2640-1053/222
1Department of Pathological Anatomy, Arrazi Hospital, University Hospital of Mohammed VI - Marrakech / Faculty of Medicine and Pharmacy of Marrakech - Cadi Ayyad University Marrakech/Morocco
2Faculty of Medicine and Pharmacy of Guelmim – Ibnou Zohr University Agadir, Morocco
3Department of Neurosurgery, Ibn Tofail Hospital, University Hospital of Mohammed VI - Marrakech / Faculty of Medicine and Pharmacy of Marrakech - Cadi Ayyad University Marrakech/Morocco
4Department of Hematology, University Hospital of Mohammed VI - Marrakech / Faculty of Medicine and Pharmacy of Marrakech - Cadi Ayyad University Marrakech/Morocco
*Corresponding Author: Imane Boujguenna. Faculty of Medicine and Pharmacy of Guelmim – Ibnou Zohr University Agadir, Morocco.
Citation: Hind Rachidi, Imane Boujguenna, Badr Darai, Khalid Aniba , Soumia Lahiaouni, Fatima Ezzahra Lahlimi et. al., (2024), Meningeal large B-cell lymphoma: Beware of the meningioma trap! A case report with review of the literature, J Cancer Research and Cellular Therapeutics, 8(8); DOI:10.31579/2640-1053/222
Copyright: © 2024, Imane Boujguenna. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 27 November 2024 | Accepted: 03 December 2024 | Published: 16 December 2024
Keywords: primary meningeal lymphoma; meningioma; large cell b lymphoma
Primary meningeal lymphoma of the central nervous system is extremely rare. Over the past decade, a number of these tumors have been reported to resemble meningioma clinically, intraoperatively and radiologically. We report the clinical, radiological, histopathological and evolutive features of a primary parieto-occipital meningeal lymphoma in a 27-year-old man, which clinically and radiologically resembled an aggressive high-grade meningioma. The patient was initially treated by surgery and then referred to hematology for possible further chemo-radiotherapy. The unfavorable evolution of the patient was due to the neurological sequelae of the surgical resection despite the regression of the tumor process objectified by follow-up imaging. Therefore, primary meningeal lymphoma of the central nervous system should be included in the differential diagnosis of meningioma and warrants anatomopathological and immunohistochemical examination of any surgical specimen and follow-up imaging.
Central nervous system CNS lymphomas occur mainly as a result of secondary spread of a distant non-Hodgkin's lymphoma [1]. Primary non-Hodgkin's lymphoma of the CNS is rare and accounts for 1% of intracranial tumors [2]. Meningeal sites of primary CNS lymphoma are extremely rare and their incidence is unknown [3]. Over the last decade, a number of these lesions have been reported to resemble meningioma clinically, intraoperatively and radiologically [4].
The aim of this paper is to report the clinical, radiological, histopathological and evolutive features of a case of primary parieto-occipital meningeal lymphoma that clinically and radiologically resembled an aggressive highgrade meningioma.
We report the case of a 27-year-old immunocompetent man, with no particular pathological history, admitted to the neurosurgery department for headaches associated with an occipital mass progressively increasing in size. The clinical examination was normal except for a left occipital tumefaction measuring 7 cm in long axis. Magnetic resonance imaging MRI of the brain showed an endo and exocranial process in the left occipital region with a meningeal origin, suggesting in the first place a meningioma. The latter was associated with leptomeningeal thickening. The tumor process was T1 hypointense Figure 1: A, T2 intermediate signal Figure 1: B and intensely and homogeneously contrast-enhanced Figure 1: C. The endocranial mass measured 3.4x2.5cm in diameter while the exocranial mass measured 7x4,7 cm in diameter. The intracranial process had a broad meningeal implantation base and was separated from the brain parenchyma by cerebrospinal fluid CSF. It invaded the superior sagittal sinus with thickening of the internal table and bone lysis opposite. An arteriogram was performed, revealing a large vascular blush with bilateral occipital projection, more pronounced on the left, which required arterial embolization before surgery. The surgical procedure consisted of scalp detachment with cranial flap, monobloc removal of the lesion, sampling of the dura mater and scalp with sampling of the fascia lata for cranioplasty. Macroscopic examination of the surgical resection specimen showed a skin flap scalp with a whitish neoplasm measuring 2x1x1cm Figure 2: C. A cranial flapsurmounted by aneoplasm measuring 11x11x8.5cm which appeared to infiltrate the bone Figure 2: A, and a fibrous wall meninges with multiple neoplasms measuring between 1 and 3cm in long axis Figure 2: B. On section, the neoplasm was lobulated, whitish in color and firm in consistency.
Figure 1: Brain MRI
A: SagittalT1 sequence showing a T1hyposignalendocranial and exocranial tumor process.
B: Axial T2 sequence showing an intermediate T2 signal tumor process.
C: Axial T1 sequence after injection of godalinium: The tumor process is intensely and homogenously enhanced.

Figure 2: Macroscopic examination of the surgical resection specimen.
A: Cranial flap surmounted by a neoplasm measuring 11x11x8.5cmwhich appears to infiltrate the bone macroscopically.
B: Fibrous wall (meninges) with multiple neoplasms measuring between 1 and 3 cm.
C: Skin flap (scalp) with a whitish neoplasm measuring 2x1x1cm.
Microscopic examination of the above described neoplasms showed a malignant round cell tumor proliferation of high cell density. It was organized in diffuse layers Figure 3. The tumor cells were medium to large in size, with round or oval nuclei, hyperchromatic in places, vesicular and nucleolated in others, with abnormal mitoses estimated at 16 mitoses/10 CFG. The cytoplasm was of medium abundance eosinophilic. The stroma was richly vascularized with large foci of tumor necrosis, without psammomas Figure 4. This tumor proliferation infiltrated the adjacent bone. Four of the lateral skin resection borders scalp were tumorous. An immunohistochemical study was indicated to clarify the nature of this proliferation. Surprisingly, the tumor cells did not express meningioma markers such as EMA Figure 5, Vimentin and PS100, nor the glial tumor marker GFAP Figure 6, whereas they strongly expressed the lymphoid markers CD45 Figure 7 and CD20 Figure 8. The plasma cell nature was eliminated with the anti-CD138 antibody Figure 9, as well as the anaplastic type by the anti-CD30 antibody, which were negative. Ki67 Figure 10 was expressed by 40% of the tumor cells Figure3. The diagnosis of large cell B lymphoma was made.


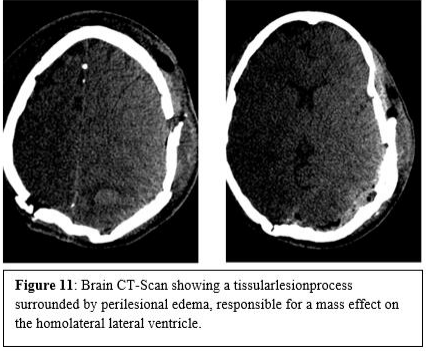
The patient was subsequently referred to the hematology department for possible management. Clinically, the patient was conscious, the neurological examination showed a right hemiparesis and limited oculomotricity of the left eye. Meningitis occurred in the postoperative period. The CSF analysis showed hypoglycorrhachia at 0.44 g/l and hyperproteinorrachia at 0.55g/l with isolation of staphylococcus homanis sensitive to ciprofloxacin and vancomycin. An extension work-up with cervico-thoraco-abdomino-pelvic CT and osteomedullary biopsy was negative. The patient had undergone a postoperative CT-scan which revealed a persistent extra-axial tissular lesion process measuring 38x32x28mm, spontaneously hyperdense, in the left occipital region, surrounded by perilesional edema, responsible for a mass effect on the homolateral lateral ventricle associated with significant infiltration of the soft tissues of the scalp Figure11.
After treatment of the infection, the patient received immuno-chemotherapy consisting of Rituximab 375mg/m², high dose methotrexate 3.5 g/m² and vincristine 1.4 mg/m² combined with intrathecal chemotherapy. The evolution after 4 courses was marked by a clinical-radiological discordance. On the one hand, the appearance of generalized tonic-clonic seizures with suspension of speech and motor deficit of the right upper limb and both lower limbs. On the other hand, the brain MRI showed a significant regression of the left parieto-occipital lymphomatous infiltration with persistence of a left parieto-occipital cortico-subcortical hypodensity area having a density similar to the CSF. The EEG showed a background theta rhythm and alpha rhythm with no obvious epileptic abnormalities on the tracing. Anticonvulsant therapy was started with good response and regression of the tonic-clonic seizure.
Primary meningeal dural lymphomas are defined as lesions with a dural insertion base, originating from the dura mater, and may involve the epidural or subdural space. Ninety per cent are aggressive diffuse large cell lymphomas and the remaining 10% are low grade MALT or marginal zone, Burkitt's or T-cell lymphomas [2,5] . They can occur either in immunocompetent patients, as it is the case in our patient, or in the context of immunodeficiency associated with Epstein-Barr virus EBV infection. Some authors have reported cases of dural lymphoma mimicking meningioma in immunocompetent patients treated either by surgery and radio-chemotherapy, or by chemotherapy alone with good results [6,7,8]. Primary meningeal lymphoma accounts for 7% of all central nervous system lymphomas, approximately 2% of all primary brain tumors and 0.8% of all lymphomas [5]. Primary dural lymphomas are known to be highly prevalent in middle-aged women [9]. The two largest series of primary dural lymphomas included 8 and 15 patients respectively and the observed female to male ratio was 3.1 and 4.1 respectively [7,10]. Our patient was middle aged as reported in the literature but male. The onset of symptoms is usually rapid. As with other processes affecting the leptomeninges, patients with primary meningeal lymphoma present with symptoms and signs of neurological and neuropsychiatric deficits with a high prevalence of cranial nerve palsies and lumbosacral radiculopathies, headache, pain and sometimes fever [10,11,12]. Our patient had isolated headache. MRI has a reported sensitivity of 20% to 37.5% for the detection of leptomeningeal lesions [13]. Diffuse meningeal large B-cell lymphoma appears on imaging non-specifically as contrast-enhanced, dural implantation base lesions, usually simulating a hyperdense meningioma on CT, hypointense on MRI [14]. Distant dural tail contrast enhancement may be seen. Hyperostoses and neighboring bone erosions are possible, sometimes extending to the scalp or through the base of the skull into the deep spaces, similar to those seen in meningiomatous lesions of superimposable location [7]. In our case, the initial imaging and location of the lesion led to an erroneous diagnosis of meningioma due to the lack of radiological specificity. The correct diagnosis was only established after anatomopathological and immunohistochemical examination of the surgical specimen. The diagnosis can be made by means of a dural biopsy, which reveals a lymphomatous proliferation in the dural tissue, arranged in confluent tumor layers, made up of large cells with round or ovoid nuclei having one or more nucleoli, with basophilic cytoplasm, surrounded by a mesh of reticulin fibres around the blood vessels. Mitotic activity is marked [6,13]. Macrophages, some with tingible bodies and a perivascular reactive lymphoid population composed of small lymphocytes are consistently associated. Necrotic changes are more frequent in cases of immunosuppression. Lymphoma cells express CD45, B markers, CD20 and also BCL2 and BCL6. The cell proliferation index is close to 60% [15]. In meningeal lymphomas, the CSF profile is always abnormal and findings may include leukocytosis, elevated protein concentration and hypoglycorrhachia. Definitive diagnosis can be established by detection of malignant lymphocytes on cytology, or a monoclonal population by flow cytometry or gene rearrangement study, which may be more sensitive. Nevertheless, there are patients with positive cytology despite negative flow cytometry, suggesting that a combined approach will give the best results [16]. Primary dural large B-cell lymphoma generally has a favorable prognosis compared to intra-parenchymal involvement or CNS metastases of systemic lymphoma [2]. The 5-year overall survival rate is over 86% [17]. However, an optimal treatment approach has not yet been established. As this tumor is potentially treatable by surgery due to the high degree of confusion with meningioma, chemotherapy and radiotherapy, it is advisable to maintain a high level of clinical suspicion when managing a case of meningioma. This is due to the rarity of cases and consequently there remains a lack of available large-scale randomized controlled trials. Therefore, most patients undergo either surgical treatment, radiotherapy, chemotherapy or various combinations of these treatment modalities without an established standardized approach [8]. The diagnosis of meningioma should be questioned in the presence of rapid local progression and rapid recurrence [14]. Our patient was initially treated by surgery and then referred to hematology for further chemo-radiotherapy. The unfavorable evolution of the patient can be explained by neurological sequelae due to the surgical resection despite the regression of the tumor process objectified by follow-up imaging. Regardless of the treatment approach, active long-term surveillance is necessary, given that patients with primary meningeal lymphoma are at increased risk of disease recurrence years after diagnosis and initial treatment [17,18]. As our understanding of the molecular pathways involved in pathogenesis continues to grow, the development of more specific and effective targeted therapy techniques against these tumors will also increase [14,17].
While leptomeningeal involvement of lymphoma can often occur as a late manifestation of systemic lymphoma, isolated leptomeningeal lymphoma is extremely rare. The latter should be included in the differential diagnosis of meningioma as it shares similar clinical and radiological features and warrants anatomopathological and immunohistochemical examination of any surgical specimen and follow-up imaging. As this tumor is potentially treatable by surgery, chemotherapy and radiotherapy, the diagnosis of meningioma should be questioned in the presence of rapid local progression and recurrence.
CNS: Central nervous system
CSF: Cerebrospinal fluid
CT: Computed tomography
EBV: Epstein-Barr virus
EEG: Electroencephalogram
MALT: Mucosa-Associated Lymphoid Tissue
MRI: Magnetic resonance imaging
The authors declare that they have no conflicts of interest.
Authors' contributions:
All authors contributed to the writing of this manuscript.
Consent to publication:
Written informed consent has been obtained from the patient for the publication of this case report and all accompanying images. A copy of the written consent is available for review by the editor-in-chief of this journal.
Financing:
The authors did not receive any specific funding for this study.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
