
Research Article | DOI: https://doi.org/10.31579/2641-5194/008
Department of Pediatric Surgery, Alexandria Faculty of Medicine, Alexandria, Egypt
*Corresponding Author: Mostafa Kotb, Department of Pediatric Surgery, Alexandria Faculty of Medicine, Alexandria, Egypt. Email: mostafa.rashad@alexmed.edu.eg
Citation: Mostafa Kotb, Marwa Beyaly. Megacystis Microcolon intestinal hypoperistalsis syndrome: An overview J. Gastroenterology Pancreatology and Hepatobilary Disorders. 3(1). DOI: 10.31579/2641-5194/008
Copyright: © 2019 Mostafa Kotb. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 10 February 2019 | Accepted: 15 March 2019 | Published: 20 March 2019
Keywords: megacystis; microcolon intestinal; hypoperistalsis syndrome; CIC; MMHIS
Megacystis Microcolon Intestinal Hypoperistalsis Syndrome (MMIHS) is a rare congenital anomaly that is considered the most severe form of functional obstruction of the gastrointestinal tract. This devastating condition is composed of non-obstructed urinary bladder, microcolon with decreased or absent intestinal peristalsis. This study was designed to describe the incidence and outcome of MMIHS.
A PubMed search was performed for the key words ‘‘megacystis microcolon intestinal hypoperistalsis’’ with no restriction on publication language. All studies reporting patients with the diagnosis of MMIHS in the period from 1976 to date were included. Detailed information with emphasis on epidemiology, diagnosis, surgical findings and outcome were recorded and critically analyzed.
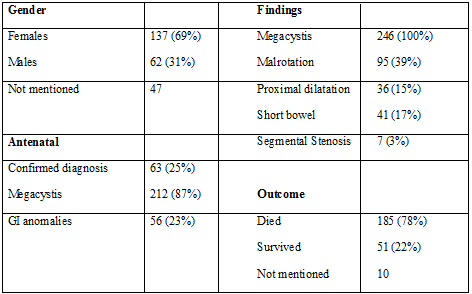
To our best knowledge, a total number of 246 patients were identified in the literature during the period from 1976 to 2018 (4). Prenatally, diagnosis was confirmed in one quarter of the cases, where 87% showed megacystis. In nine cases only, parents accepted the option of termination of pregnancy after prenatal diagnosis of MMIHS and genetic counseling. Gender was mentioned in 199 cases. Of these, 137 patients (approximately 69%) were females, whilst 62 (31%) were males. The female-to-male ratio was 2.2:1. In about half of the patients (129 patients), one or more surgical interventions were reported. As its name implies, megacystis and microcolon were the most frequent findings at autopsy or surgery. Moreover, malrotation was reported in 95 patients, dilated proximal small bowel in 36, short bowel in 41, and segmental stenosis of small bowel in 7. A range of interventions was reported including gastrostomy, jejunostomy, ileostomy, cecostomy, segmental resection of jejunum and ileum, adhesiolysis, rectal biopsy and internal sphincter myectomy. Vesicostomy was reported in 47 patients. Outcome was reported in 236 patients. Out of those, 185 patients (78.4%) died and 51 patients (21.6%) were alive at the time of publication (Table 1). The most common cause of death was overwhelming sepsis followed by multiple organ failure and malnutrition. The majority of the survivors were maintained on TPN, while only 12 patients underwent multivisceral transplantations. According to the obtained data, the majority of the survivors were independent of parenteral nutrition, yet, bladder dysfunction persisted and clean intermittent catheterization (CIC) has been reported.
Since first described in 1976 by Berdon on five girls, 2 of whom are sisters (5), few hundred cases of MMIHS have been reported and contributed to a better understanding of this devastating disease. As long as there is neither definitive medical nor surgical treatment have proved to improve the intestinal and bladder dysfunction, the majority of MMIHS patients are therefore dependent on TPN to prevent malnutrition, beside the known complications such as sepsis and renal failure (6).
MMHIS is more common in females, with female to male ratio of 2.2:1. Many authors claim that under diagnosis in males is due to the more severe form in males resulting in intrauterine deaths (7), whilst others state that MMIHS can be diagnosed as prune belly syndrome (PBS) instead, leading to a bias in female to male ratio (8). Overlap of MMIHS and PBS have occurred (9, 10) although most cases present as sporadic ones, MMIHS can occur in a familial fashion. In a study, familial MMIHS was evident in a total of 47 occasions, with 19 families had a pair of affected siblings, and a family had three children with MMIHS (11). It had been suggested that mutation in actin gamma 2 (ACTG2) on chromosome 2p13 and loss of leomodin genes, both are responsible for encoding of one of the six actin myoforms present in the smooth muscles of the urinary and gastrointestinal systems, resulting in their hypoperistalsis(12,13).
With improvement in antenatal care, MMHIS can be diagnosed prenataly. Up to 25% of cases were achieved via prenatal diagnosis. Enlarged bladder (megacystis) was the main finding in 87% of cases, whilst gastrointestinal anomalies were noted in 23% only (13). While megacystis is more common in male fetuses, it is usually associated with oligohydramnios and caused by mechanical lower urinary tract obstruction (LUTO). Therefore, MMIHS should not be excluded in male fetuses with megacystis, especially if there is no oligohydramnios. On the other hand, it is strongly suspected in female fetuses with accompanying polyhydramnios because LUTO is rare in females and oligohydramnios is an invariable finding (14). Moreover, amniotic fluid analysis for enzymatic changes, in addition to magnetic resonance imaging, has increased the accuracy of prenatal diagnosis of MMIHS (15). Therefore, parenteral counselling to ensure that they are aware of the pathology, prognosis, therapeutical options and care of MMIHS should be done in order to make a substantiated decision on the sequel of the pregnancy. Nine couples decided to terminate pregnancy due to prenatal diagnosis of MMIHS in the current literature.
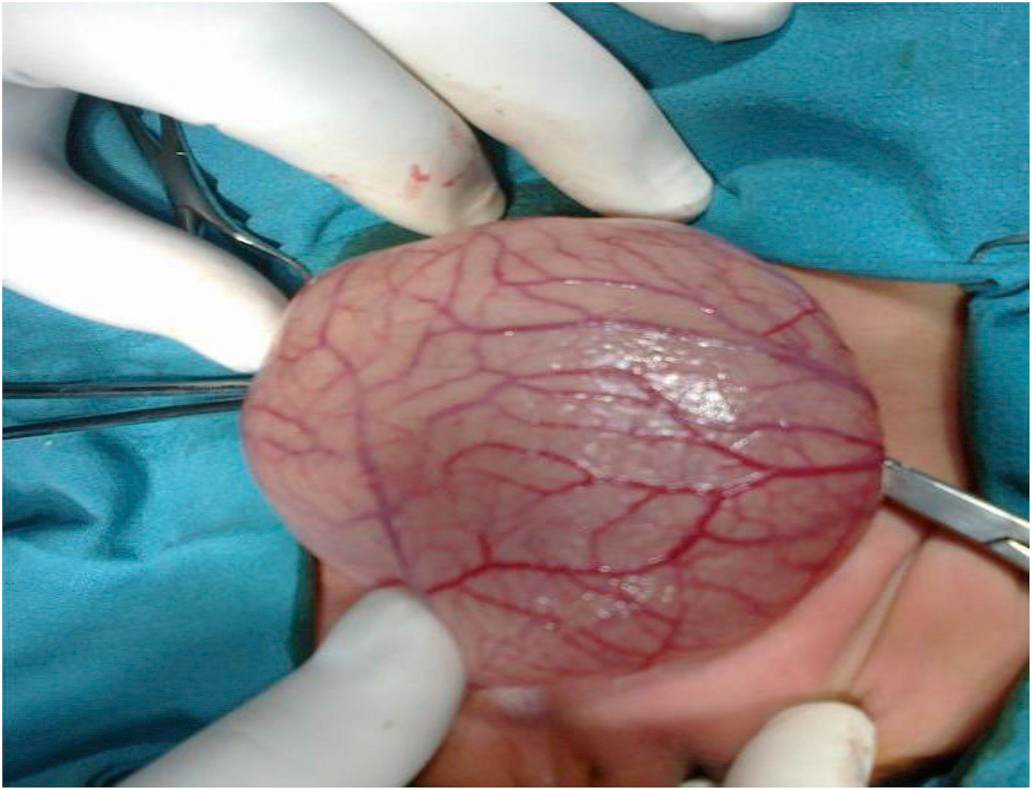
Management varied considerably among most publications and exact surgical procedures were reported inconsistently. Since the most frequent findings were megacystis (Figure 1), functional obstruction, and malrotation, therefore, all of the operations were performed mainly to decompress the intestinal and urinary systems. Surgeons frequently chose to perform diverting ileostomy to benefit from early oral feeding to avoid long term TPN, and biopsy to exclude Hirschsprung’s disease and other related motility disorders (16). Vesicostomy was reported in less than a fifth of cases only, after considering insertion of Foley catheter for initial decompression. While some authors consider vesicostomy only if catheter was not tolerated or caretaker was unable to manage CIC (17), a minority of surgeons perform vesicostomy at first glance in the setting of elevated BUN to protect the kidney and prevent the progression of overwhelming sepsis (16). Others believe that the dilated urinary tract will not collapse even with maintained catheter drainage, so they encourage peritoneal dialysis catheter insertion under vision to avoid iatrogenic GI and urinary injury (18). Other procedures occasionally performed including gastrostomy, jejunostomy and cecostomy in specific indications. Unfortunately, surgical interventions failed to improve enteral food intake, intestinal pseudoobstruction or bladder function 4. Hence, several authors now agree that the decision for surgical interventions should be made on individual basis and mostly restricted to supportive interventions such vesicostomy and enterostomy (2). Recently, multivisceral transplantation became a valuable therapeutic treatment for children with irreversible intestinal and/or total parenteral nutrition failure (19).
Fifty one out of 236 patients were alive at the time of publication, which revealed an overall survival rate of 21.6% in this review. In a previous review (1976–2011), 43 out of 218 patients were alive at the time of publication (survival rate 19.7%) 4. In contrast, analysis of the more recent time period from 2011 to 2018 revealed an increase of the survival rate to 44% (8 out of 18 patients were alive at the time of publication). However, more cases are required in order to conclude a statistical significance. Unfortunately, no sufficient reports were performed to indicate long-term survival. The most frequently reported cause of death in MMIHS patients was overwhelming sepsis followed by multiple organ failure and malnutrition. There are several reasons for the development of sepsis in MMIHS patients. Firstly, intestinal conditions, such as malrotation and short bowel with the resulting functional obstruction of the bowel may cause bacterial overgrowth and translocation, hence, leads to bacteremia and subsequent sepsis. Moreover, urinary tract infections (UTI) as well as catheter-induced sepsis resulting from prolonged TPN can augment the sepsis (20). Lastly, in several cases, attempts to provide sufficient enteral feeding have resulted in fatal pneumonia (21).
Renal failure occurs as a consequence of aperistaltic urinary bladder with resultant reflux and repeated UTI leading to renal scarring. Liver dysfunction is a common complication. In a large survey conducted in Japan, it was reported in 84% of the cases, with 6 patients out of 9 died from liver failure. This failure was mostly attributed to the prolonged parentral nutrition with its devastating effect on liver, and less commonly due to enteritis and sepsis (22).
Only 12 transplantations were performed to date with a reported 3-year survival of 50% of those series. All survivors tolerated enteral feedings; however, bladder function did not improve and catheterisation had to be continued after transplantation(19). While there was a significant improvement of the results of multivisceral transplantation in the recent years (23), complications are inevitable. These include infection, rejection, and post-transplant lymphoproliferative disease (PTLD). Moreover, reports regarding long term complications and survival of MMIHS patients after transplantation are still lacking (24).
Although, recently, there was improvement in the survival rate of MMIHS compared to the past, yet, the mortality is still high. With the improvement in supportive care over time the life span of children with MMIHS may increase; however, intestinal transplantation appears to be the only viable therapy to restore gastrointestinal motility.
The authors have no conflicts of interests.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
We thank Prof. Sameh Shehata, Professor of Pediatric Surgery, Alexandria Faculty of Medicine for his continuous and endless support, and tips in the process of publication.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
