
Research Article | DOI: https://doi.org/10.31579/2578-8868/232
1 Department of health care. 2Department of Ultrasound Medicine, Yantaishan Hospital, Yantai
2 64008, Shandong Province, China.
*Corresponding Author: Ji-Ming Zou, Department of Health Care, Yantaishan Hospital, 264008,Shandong Province, China
Citation: Chao Han, Xiao-Yu Li, Ji-Ming Zou (2022). Medium Term Study of Incidence, Risk Factors and Type of Stroke in Hypertensive Patients. J. Neuroscience and Neurological Surgery. 11(4); DOI:10.31579/2578-8868/232
Copyright: © 2022 Ji-Ming Zou, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 01 January 2022 | Accepted: 25 February 2022 | Published: 07 February 2022
Keywords: hypertension; stroke; prognosis; risk factors
Background and Aims: To investigate the incidence and risk factors of stroke in hypertension patients over 60 years of age, and to investigate the correlation.
Methods: A retrospective analysis of 454 hypertension patients who were diagnosed through examination were divided into 4 groups, of which included group A (hypertension plus type 2 diabetes) were 4 cases, group B (hypertension plus hyperlipidemia) were 367 cases, group C (hypertension plus type 2 diabetes and hyperlipidemia) were 47 cases, and group D (hypertension) were 36cases. Every patient was given observation after definite diagnosis and treatment of 54 months, and to investigate the incidence of acute cerebral infarction, cerebral hemorrhage.
Results: There were 44 patients occurred acute cerebral infarction in all 4 groups. Of these cases, there were 1 case in group A, 31 cases in group B,10 cases in group C and 2 cases in group D. In group B, 3 cases occurred cerebral hemorrhage. Logistic regression analysis showed systolic blood pressure (OR=1.106, P=0.001), fasting glucose (OR=2.059, P=0.000) and low-density lipoprotein cholesterol (LDL-C) (OR=0.104, P=0.025) were risk factors for stroke.
Conclusions: Higher levels of blood glucose and/or blood lipid associate with higher risk of stroke in patients with hypertension.
Hypertension leads to the over-activation of sympathetic nervous system, resulting in the excessive release of catecholamines. Kidney causes water and sodium retention, blood volume overload; Overactivation of renin-angiotensin-aldosterone system causes water and sodium retention; Vascular endothelial function is reduced, carbon monoxide release is reduced, causing excessive vasoconstriction. Diabetes mellitus lipid metabolism, vascular endothelial dysfunction, platelet dysfunction. Elevated blood lipids in the blood lipid easier to deposit on the blood vessels in the membrane, lipid and compound carbohydrate gathered in the lining of the blood vessels, causing the lining of the blood vessels inflammatory reaction, and further lead to fibrous tissue hyperplasia, calcium precipitation, gradually lose the artery wall elasticity, gradually hardens, thickening, blood vessel lumen, if there is a blood vessel is blocked, or brittle strengthen blood vessel walls, Rupture bleeding and other problems, easy to cause infarction, cerebral hemorrhage and other problems.
Stroke is one of the leading causes of death and disability in adults worldwide [1]. It is a group of acute cerebrovascular diseases with cerebral tissue ischemia or hemorrhagic injury as the main clinical manifestations, including cerebral hemorrhage, cerebral infarction and subarachnoid hemorrhage. This study investigated the incidence of stroke in patients with hypertension who were first diagnosed by physical examination, aiming to understand the relationship between the levels of risk factors such as blood glucose and blood lipid and the occurrence of stroke in patients with hypertension.
The subjects were enrolled in the physical examination department of yantai mountain hospital on June 1, 2008 and December 31, 2011. The inclusion criteria were as follows: 454 patients with ≥60 years of essential hypertension (EH) were found and diagnosed for the first time, including 425 males, aged from 61 to 75 years old, with an average age of (65.2±3.9) years. There were 29 females aged from 60 to 74 years old, with an average age of (64.7±4.1) years. According to the fasting blood glucose (FBG), triglyceride(TG), total cholesterol(TC), low density lipoprotein cholesterol(LDL- C) level is divided into four groups,4 cases of Type 2 diabetes mellitus (T2DM) were combined with EH (Group A).All are male. There were 367 cases in EH combined hyperlipidemia group (Group B), including 353 males and 14 females. There were 47 EH patients with T2DM and hyperlipidemia (Group C), including 41 males and 6 females. There were 36 cases in simple EH group (D group), including 27 males and 9 females. There were 7 cases with a history of T2DM and 119 cases with a history of hyperlipidemia, all of which did not receive standard treatment in community hospitals. No history of cerebrovascular and renal disease. Family history of stroke. The occupation was workers (1 case in Group A, 235 cases in group B, 11 cases in Group C, 5 cases in Group D), and the others were teachers and civil servants.
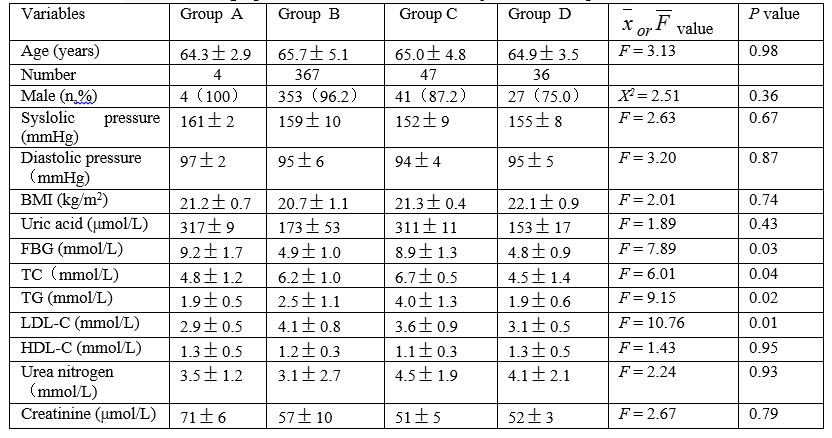
The data of cases, age, sex, initial blood pressure, smoking, and Body Mass Index (BMI) were normally distributed in each group. After multiple mean anova tests, there was no statistically significant difference between the four groups in terms of each indicator (P >0.05).There was no significant difference in urea nitrogen, creatinine and uric acid among the groups (P >0.05).The comparison of clinical data of the 4 groups before treatment is shown in Table 1.
Treatment Methods
Roche Roche-PPE instrument in Switzerland. Philips Brilliance 64 row volume CT or GE MRI Signa HDxT 1.5T cranial scan. Blood pressure was measured with OMRON electronic sphygmomanometer after 10 minutes of rest.
Relevant standards
All the selected patients met the diagnostic criteria formulated by the fourth National Academic Conference on Cerebrovascular Disease and The Chinese Guidelines for diagnosis and Treatment of acute ischemic stroke 2014[2], and the Oxfordshire Community Stroke Plan typing method was used to determine the subtype of the patient [3].It was divided into total anterior circulation (TACI), partital anterior circulation (PACI), posterior circulation (POCI), lacunar Coinfarction (LACI). T2DM and EH are in accordance with the target standards for diagnosis and control of T2DM according to the 2007 Chinese Guidelines for prevention and Treatment of Type 2 diabetes and the 2005 Revised Chinese Guidelines for prevention and Treatment of hypertension. Dyslipidemia is determined by The Chinese Guidelines for the Prevention and Treatment of dyslipidemia in Adults (2007) [4]. Analysis was performed on the two-factor factorial design data, count data were compared for X2 test, and logistic regression and Cox's proportional hazards regression model analyses were used for correlation test. P <0>
Standard of treatment for 4 groups of patients
(1) Blood pressure < 140 mmHg=0.133kPa).>
Incidence of cerebral infarction and cerebral hemorrhage in the 4 groups
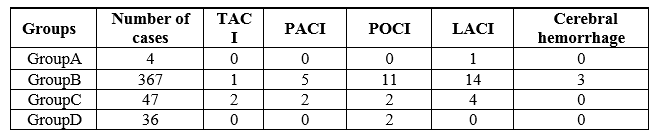
There were 44 cases of acute cerebral infarction and 1 case of LACI in group A.There were 1 case of TACI, 5 cases of PACI, 11 cases of POCI and 14 cases of LACI in group B.There were 2 cases of TACI, 2 cases of PACI, 2 cases of POCI and 4 cases of LACI in group C.POCI was found in 2 patients in group D.The incidence of TACI, PACI, LACI and POCI was 0.66%, 1.54%, 4.19% and 3.30%.There were 3 cases of cerebral hemorrhage, which occurred in group B, with a history of physical activity before the onset of the disease. The bleeding volume was about 18ml, 11ml and 7ml.Are shown in table 2. 33 cases of coronary atherosclerotic heart disease occurred during follow-up treatment, including 22 cases in group B, 8 cases in group C, and 3 cases in group D.There were 4 cases of acute myocardial infarction, including 2 cases in Group B, 1 case in group C, and 1 case in group D. No other vascular events occurred.
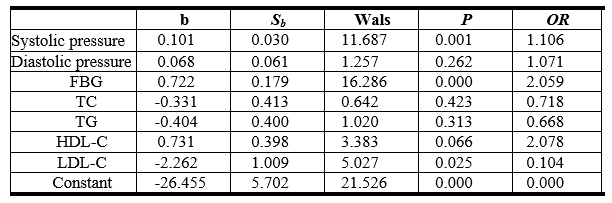
Risk factors for stroke
Logistic regression analysis showed that systolic blood pressure (OR =1.106, P =0.001), fasting blood glucose (OR =2.059, P =0.000) and
LDL-C (OR =0.104, P =0.025) were risk factors for stroke, as shown in Table 3.
The relationship between hypertension subtypes and stroke incidence
The incidence of stroke in the study cohort was the highest in the simple systolic hypertension group (1.12/100 person-year), and the HR of total stroke and hemorrhagic stroke in patients with this subtype of hypertension was significantly higher than that in other hypertensive groups (P <0>
Hypertension is the primary and interventional risk factor for stroke. Increased blood pressure is in direct proportion to the occurrence of stroke, and effective control of blood pressure can reduce the incidence of stroke [5]. Hypertension has been troubling countless people for many years, often accompanied by disorders of fat and sugar metabolism and changes in heart, brain, kidney, retina and other organs. Gong Tao reported the statistics of the Ministry of Health in 2007 in China, cerebrovascular disease ranks the first among public death diseases [6]. Stroke is the most common type of cerebrovascular disease, among which ischemic stroke accounts for 80% ~ 85% of all strokes. Hypertension leads to hyaline or fibrous changes in the wall of the small artery at the skull base and pathological changes such as focal hemorrhage, ischemia and necrosis, etc. The strength of the wall of the vessel is weakened, resulting in localized dilation and formation of tiny aneurysms. On this pathological basis, the cerebral vascular rupture of the lesion causes hypertensive intracerebral hemorrhage. Patients with cerebral hemorrhage before the presence of emotional excitement, excessive physical activity or other factors can induce a sudden increase in blood pressure. There were also three cases of cerebral hemorrhage in 454 hypertensive patients.
Data show that the global incidence of ischemic stroke is 169/100,000 and the incidence of stroke increases with age [7]. Acute progressive stroke refers to progressive or stepped-up progression of neurological deficit symptoms within 48h after stroke onset. It is a clinical process rather than an independent disease unit. Patients often suffer from deterioration of the condition due to aggravation of brain damage, with significantly increased disability rate and fatality rate. Tei H et al. reported that the study of oxfordshire Community Stroke Project(OCSP) showed that the incidence of progressive Stroke was 41.9%, 6.3%, 26.2%, and 21.7%, respectively, among the four types of TACI, PACI, LACI, and POCI, with the highest incidence of progressive Stroke among TACI patients[8]. In this study, 5 cases of progressive stroke occurred in the 4 groups, including group B and Group C. The incidence of progressive stroke in patients with TACI, PACI, LACI and POCI was 33.3%, 0%, 13.2% and 7.7%, respectively. It was also confirmed that TACI patients had the highest incidence of progressive stroke, indicating that the identification of subtypes of acute cerebral infarction is of great significance to the prognosis of patients and the formulation of treatment plans.
It has been reported in the literature that smooth muscle cell recombination occurs in the arteriole wall, extracellular matrix, especially collagen increase, arteriole wall thickening and lumen thrombosis during hypertension, and hypertension is one of the major independent risk factors. Hypertension leads to increased vascular shear stress, hypertrophy of the inner wall of blood vessels, changes the ability of vascular endothelial cells to release vasoactive substances, brain circulatory regulation dysfunction, and right shift of the regulation curve [9]. Chen Yuhui et al. showed that the incidence of hypertension, hyperfibrinogenemia, atrial fibrillation and carotid artery plaque was higher in elderly patients with ischemic stroke, and systolic hypertension was the most important risk factor for elderly patients with ischemic stroke [10]. Xu Xin et al. found in their study that the important influencing factor of first cerebral infarction in hypertensive patients was compliance with antihypertensive drug therapy, good compliance was a protective factor, and poor compliance and last treatment for hypertensive patients were prone to cerebral infarction [11]. Vemmos KN et al. showed that blood pressure was positively correlated with the occurrence of stroke regardless of gender, age and type of stroke [12]. Therefore, sufficient attention should be paid to the active and effective control of blood pressure in the secondary prevention of cerebrovascular diseases. The benefits of antihypertensive treatment mainly come from the antihypertensive itself. It is necessary to understand the antihypertensive ability of various antihypertensive drugs under the guarantee of safety.
Diabetes is an important risk factor for cerebrovascular disease. The incidence of stroke in diabetic patients is more than 1 times higher than that in non-diabetic patients, and about 20% of diabetic patients eventually die of stroke [13]. The measurement of HbA1c in high-risk population of cerebrovascular disease is very helpful to assess the risk of first stroke.HbA1c in diabetic patients can reflect the average blood glucose level 2 to 3 months before blood collection. Compared with fasting blood glucose, HbA1c is less affected by various factors, and is an important indicator to measure blood glucose control in diabetic patients. Daimon M et al. proved that increased HbA1c can induce and promote atherosclerosis [14]. Possible mechanisms of stroke in diabetes mellitus: (1) Hyperglycemia causes endothelial injury: Vascular endothelium specific injury is one of the characteristics of T2DM. The bioactivity of endothelial nitric oxide in brain circulation of diabetic patients is reduced compared with that of normal subjects. (2) Hyperglycemia causes accumulation of blood lactic acid: Accumulation of lactic acid causes intracellular acidosis, increases lipid peroxidation and produces free radicals, promotes intracellular calcium overload, destroys mitochondrial functional mechanisms, and aggravates and promotes ischemic brain tissue damage. (3) Hyperglycemia destroys the blood-brain barrier: hyperglycemia after stroke leads to the destruction of the blood-brain barrier, leading to cerebral edema and hemorrhagic transformation after ischemia. (4) Hyperglycemia promotes the accumulation of central excitatory amino acid glutamate: glutamate accumulates in the extracellular area and activates the post-synaptic glutamate receptor, which induces the over-opening of calcium channels and leads to mitochondrial damage and neuronal death.
Hyperlipidemia, which is a cause and effect of hypertension and diabetes mellitus, is an important risk factor for cerebrovascular disease. The European 4S test showed that statins and various lipid-lowering drugs may stabilize atherosclerotic plaques and promote plaque stability by improving vascular endothelial function, anti-inflammator and anti-sympathetic effects [15].SPARCL study also verified that further lowering LDL-C level, even if LDL-C≥2.60 ≤4.94mmol/L, can reduce recurrent stroke in patients with recent stroke or TRANSIENT ischemic attack [16]. Gong Tao pointed out the role of dyslipidemia in atherosclerotic stroke and the principles of clinical treatment [17]. Hypertriglyceridemia participates in the arteriosclerosis process by increasing small-particle LDL-C, lowering HDL-C and inhibiting fibrinolytic system. High concentration of LDL-C inactivates endothelium-derived relaxation factor or nitric oxide, reduces its deoxidization capacity, and induces excessive expression of plasminogen activator inhibitor-1 mRNA in vascular endothelial cells, thus increasing the plasma level. In the case of hypertriglyceridemia, lipidization of cholesterol in phagocytes is enhanced, which promotes the formation and aggregation of foam cells and reduces the stability of atherosclerotic plaque. Hyperlipidemia has a strong effect of causing cerebrovascular diseases, especially when accompanied by hyperinsulinemia, insulin resistance and hyperglycemia. Effective prevention and control of hyperlipidemia, hyperglycemia and hyperinsulinemia in clinical practice is of great significance for reducing the incidence and mortality of stroke. Inzitari D et al. reported that hyperlipidemia was also an independent risk factor[18].Pan Xiaodong et al. found that T2DM patients with dyslipidemia were relatively simple in their study on the detection of thrombus formation indicatorsT2DM patients are more likely to be in a state of high adhesion and high coagulation, and more likely to form thrombosis[19].
Current research using stroke risk assessment tools, such as the Framingham stroke risk assessment (FSP), FSP using Cox proportional hazards model, to stroke risk factors (age, systolic blood pressure, high blood pressure, diabetes, smoking, have cardiovascular disease, atrial fibrillation and ecg showed left ventricular hypertrophy) as a covariate, score is calculated based on weighting coefficient model [20]. In some studies, FSP was used as reference for scoring, and indicators such as serum creatinine and stroke history were added [21,22]. Flossmann E et al. found that ischemic stroke was affected by genetic factors, and the risk of ischemic stroke increased by about 30% in those with positive family histories [23].The application of stroke risk assessment tools is helpful to identify high-risk patients with stroke, and the screened high-risk patients should adopt individualized intervention treatment according to specific risk factors.
The American Heart Association, stroke Association and Chinese Neurology Branch of the Chinese Medical Association point out in the guidelines of "Primary prevention of stroke" that screening and prevention management of high-risk groups for stroke should be strengthened in addition to general prevention [24-26]. Hypertension, diabetes, dyslipidemia and other factors have been recognized as important risk factors for recurrent cerebrovascular disease, also known as etiological vascular risk factors, and the incidence and level of etiological vascular risk factors can also affect the risk of recurrence [27]. Therapeutic lifestyle changes are not only the basis for the treatment of dyslipidemia in diabetic patients, but also the fundamental means to prevent dyslipidemia in diabetic patients [28]. Therefore, patients should be educated to adjust their diet and promote a healthy lifestyle, which includes weight loss, smoking cessation, alcohol control, salt restriction, aerobic exercise, attention to mental health, and optimistic and open-minded attitude towards life [29]. Gyundy SM et al. pointed out that statins can reduce LDL-C by 25% ~ 55%, and statins should be the first choice for both primary and secondary prevention[30].In the process of EH prevention and treatment, the treatment rate and control rate of EH can be improved through effective community intervention to improve patients' medication compliance [31] . In this study, 44 patients were followed up after 54 months of treatment for acute cerebral infarction, with the incidence of 9.69%, among which the incidence of TACI, PACI, LACI and POCI was 0.66%, 1.54%, 4.19% and 3.30%.The incidence of acute cerebral infarction was 25.00% in group A, 8.45% in group B, 21.28% in group C and 5.56% in group D. At present, sufficient evidence-based medicine has proved that the treatment of hypertension is beneficial to the primary and secondary prevention of stroke. The treatment of hypertension and the control of blood glucose and blood lipids, two risk factors, can reduce the risk of stroke, which has important clinical significance for the prevention of stroke.
Based on these considerations, the following recommendations are made.
(1) Antihypertensive therapy is recommended for patients with ischemic stroke and TIA to reduce the risk of recurrent stroke and other vascular events (grade I recommendation, Grade A evidence). Under the reference of advanced age, basic blood pressure, daily medication, tolerance, etc., the hypotensive target should generally be≤140/90 mmHg, and the ideal target is≤130/80 mmHg (gradeⅡ recommendation, Grade B evidence).
(2) The benefits of antihypertensive therapy in preventing recurrence of stroke and TIA were mainly derived from the antihypertensive therapy itself (grade I recommendation, Grade A evidence). Single drug or combination therapy is recommended for antihypertensive therapy (gradeⅡrecommendation, Grade A evidence). The selection of specific drugs and combination regiments should be individualized.
Funding
This study does not need any fund support, and all the work is completed within the normal work content and time. The data used in the study is also easy to access.
Conflicts of interest
We declare that we have no financial and personal relationships with other people or organizations that can inappropriately influence our work. There is no professional or other personal interest of any nature or kind in any product, service and/or company that could be construed as influencing the position presented in, or the review of this manuscript.
Ethics approval and consent to participate
We declare that all human participants, human material, and human data, have been approved by Yantaishan Hospital Ethics Committee and Yantai Medical Ethics Committee (the reference number: 2008027) and have therefore been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. We have to state that specific national laws have been observed, too. The informed consent of all subjects and/or their legal guardians has been obtained for all procedures performed in this study.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
Conceptualization : Ji-ming Zou, Xiao-yu Li, Chao Han.
Data curation : Xiao-yu Li.
Investigation : Ji-ming Zou.
Methodology : Ji-ming Zou, Chao Han.
Writing – original draft : Ji-ming Zou, Xiao-yu Li.
Writing – review & editing : Ji-ming Zou, Xiao-yu Li, Chao Han.
Thanks to our hospital and related departments for their strong support in this study, and thanks to all the participating patients for their understanding and support.
Consent for Publication(Not Applicable)
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
