
Case Report | DOI: https://doi.org/10.31579/2578-8965/207
Family Physician & Public Health Consultant Bengaluru.
*Corresponding Author: Suresh K, Family Physician & Public Health Consultant Bengaluru.
Citation: : Suresh K, (2024), Medical Management of Uterine Fibroids-A hope for Fertile Women! J. Obstetrics Gynecology and Reproductive Sciences, 8(3) DOI:10.31579/2578-8965/207
Copyright: © 2024, Suresh K. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 01 March 2024 | Accepted: 14 March 2024 | Published: 21 March 2024
Keywords: fibroid; leiomyoma; serm; pbac score; mifepristone; ormeloxifen; pelvic inflammatory diseases (pid); estrogen and progesterone receptors; botanical drug; polyherbal
Uterine fibroids or Myomas or Leiomyoma of uterus are the most common type of benign tumor of uterus and most common pelvic tumour in women with unclear etiology.
Uterine fibroids or Myomas or Leiomyoma of uterus are the most common type of benign tumor of uterus. In India the incidence of fibroids is most common in women of 31- 40 years of age i.e. as more than 1/3 (35%) of them get affected.
Recent understanding of etiology suggests increased number of estrogen and Progesterone Receptors, increased COMT gene expression and TGF-B3. Risk factors for developing fibroids are age, early age at menarche, reduced fertility, frequent caffeine consumption, obesity, hypertension, diabetes mellitus, alcohol consumption and previous pelvic inflammatory disease (PID). Rural women are at a much higher risk of uterine fibroids than urban women in India. (37.65% vs.24%) probably due to multiparty at a young age disturbing Estrogen and Progesterone Receptors.
Treatment options for symptomatic uterine fibroids include medical, surgical, and radiologically guided interventions. Although curative treatment relies on surgical therapies- either myomectomy or hysterectomy, medical treatments are considered the first-line treatment to preserve fertility and avoid or delay surgery. Medical therapy is in nascent stage in India.
Medical treatment must be individualized based on age, signs & symptoms, sustained reduction of the size and sustenance of fertility if desired with minimal side effects.
Materials and Methods: This article is based on a literature review on medical therapy being tried on a case the author is managing now. The initial results are encouraging and need to monitor the reduction of the size or volume of the Fibroid in coming months.
Uterine fibroids or Myomas or Leiomyoma of uterus are the most common type of benign tumor of uterus and most common pelvic tumour in women. Exact etiology is not known but the cause estimated to be is estrogen and progesterone which proliferate tumour growth as fibroid rarely occur before menarche and reduces after menopause. Risk factors for developing fibroids are age, early age at menarche, reduced fertility, frequent caffeine consumption, obesity, hypertension, diabetes mellitus, alcohol consumption and previous pelvic inflammatory disease (PID). The prevalence of uterine fibroids varies with geographical and racial influences and environmental factors.
Globally, the age-standardized incidence of uterine fibroids has been increasing in recent years. In contrast, age-standardized DALY rates have exhibited a decreasing trend. Eastern Europe, Tropical Latin America, Brazil, and India experience the greatest uterine fibroid burden. Uterine fibroids or Myomas or Leiomyoma of uterus are the most common type of benign tumor of uterus and most common pelvic tumour in women. as reflected in the higher incidence rates among these age groups. From 1990 to 2019, the global age-standardized incidence of uterine fibroids increased by 6.87% from 225.67 to 241.18 per 100 women.
In India the incidence of fibroids is most common in women of 31- 40 years of age i.e. as more than 1/3 (35%) of them get affected [1]. There is a difference in incidence in rural and Urban India. Rural women are almost at one and half times risk of uterine fibroids than urban women in India. (37.65% vs.24%) and urban India (24%) women. Incidence in Pakistani women was 78%. The main symptoms are a heavy menstrual flow, abnormal uterine bleeding, pelvic pain, frequent urination, and constipation.
The medical treatment for uterine fibroids includes i) Gonadotropin-releasing hormone (GnRH) agonists- which reduce fibroids by blocking the body from making the hormones estrogen and progesterone ii) Gonadotropin-releasing hormone (GnRH) antagonists, iii) Progestin-releasing intrauterine device (IUD), iv) Tranexamic acid (Lysteda, Cyklokapron) and v) Other medicines.
This article is based on current experience of trying medical therapy for a case of single posterior submucosal Fibroid. The author is of the opinion the accessibility to Scanning in the last decade more and more women can be diagnosed at early stage and managed medically.
Shilpa, the Youngest Lady with Uterine Fibroids in 2024:
First February 2024 one of my nieces from a mofussil town in Karnataka India approached me for second opinion, sharing an Ultrasound scan of abdomen and Pelvis.
Shilpa is a young lady of 37 years, married about 15 years ago and has a 14-year-old daughter and 6-year-old son. The main complaints were Menorrhagia in the past 6 months, coupled with abdominal pain and weakness. A local gynecologist checked her physically and got her Routine blood laboratory test, which showed her to be anemic with HB=8.5 gm/ Dl and an abdomen and Pelvic report reading “Posterior Submucosal Fibroid size 3.5x3.1 cm. all other abdominal structure were reported to be normal. She was put on Tablet Sevista 60mg (Ormeloxifene-60.0 Mg) tablets basically a contraceptive twice a week, Iron & Folic acid, and Vit B12 supplementation. Ormeloxifene is an excellent drug in controlling dysfunctional uterine bleeding without effecting normal endocrinal and physiological parameters. It leads to a significant reduction in menstrual blood loss and a significant decrease in endometrial thickness without any major side effect. Her periods after use of 15 tablets over 1 month has shown a decrease in menstrual flow by 50% .


Uterine leiomyomas are the most common benign uterine tumours affecting around 20-25% women in the fertile age group [1]. They are the most common type of benign tumor of uterus and most common pelvic tumour in women. Exact etiology is not known. In India the incidence of fibroids is most common in women of 31- 40 years of age i.e. as more than 1/3 (35%) of them get affected. Fibroids may be tiny and described as “seedlings” or grow large enough to alter the shape and size of the uterus. Those that grow on the outer wall of the uterus, called the serosa, can develop on a narrow stem that supports the larger growth, called pedunculated fibroids. Fibroids can grow as a single nodule or in a cluster. Clusters of fibroids can range in size from 1 millimeter to more than 20 centimeters (8 inches) in diameter or even larger. For comparison, fibroids can be as small as a seed or as large as a watermelon. The pathogenesis of the tumour is still not well understood. Hence, medical management of this condition is still in its nascent stage. Fibroids can shrink when hormone levels drop as it happens after menopause and therefore, we see symptoms improving for better after menopause. Medical management uses this principle of modifying the hormone levels.
Types of Uterine Fibroids: These growths can develop within the wall of the uterus, inside the main cavity of the uterus or on the outer surface of the uterus. Based on where they grow, there are three major types of uterine fibroids. 1. Intramural fibroids grow within the muscular uterine wall. 2. Submucosal fibroids bulge into the uterine cavity. 3. Sub-serosal fibroids project to the outside of the uterus. 4. Pedunculated fibroids-the least common type, they attach to the uterus with a stalk or stem, often described as mushroom-like. In India Prevalence of submucosal fibroids is around 40%, intramural fibroids 19.3%, submucosal polyp 14.5%, seedling fibroid 13.9% and sub serosal fibroid 10.2% [1]. The size of the fibroids and the manifestations they exhibit decides the course of management. Based on the size i) Small Fibroids can be less than 1 cm to 5 cm, ii) Medium Fibroids range from 5 cm to 10 cm the size of a plum to an orange iii) Large Fibroids can be 10 cm or more, ranging from the size of a grapefruit to a watermelon. Surgical management is advocated for women with fibroids >3 cm in diameter causing significant symptoms, pain or pressure and wishing to retain their uterus may consider myomectomy, and if uterus can be removed hysterectomy are the treatment of choices. Intramural Fibroids of about 4 cm or more, can impact ovum implantation and might block the fallopian tubes, which can cause infertility. Sometimes fibroids can affect the mode of delivery of a baby.
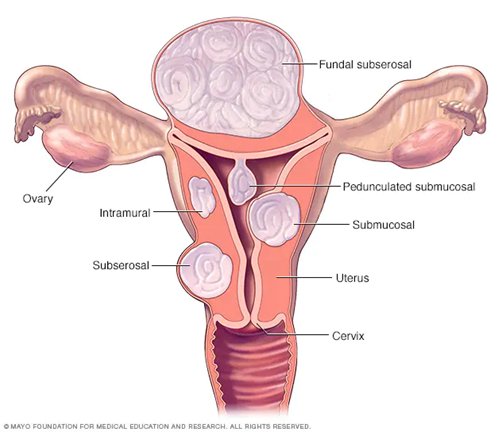
Figure 2: Types of Uterine Fibroids.
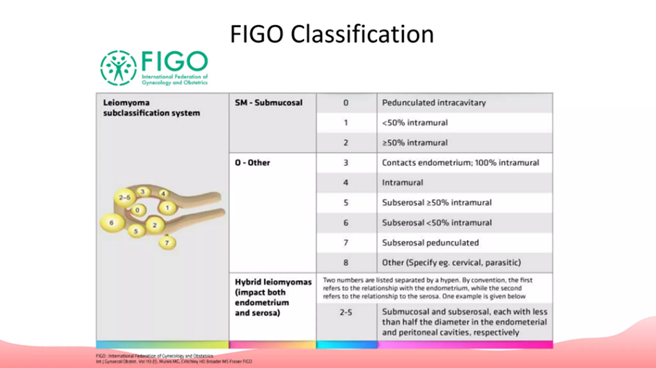
International Federation of Obstetrics & Gynecology (FIGO) subclassified fibroids as:
1. Sub-mucosal: i) 0= Pedunculated intracavity, 1=<50 xss=removed>50% intramural.
2. Others: 3=contacts endometrium-100% intramural,4=Intramural, 5=Sub serosal >50% intramural, 6= Sub serosal <50 xss=removed>
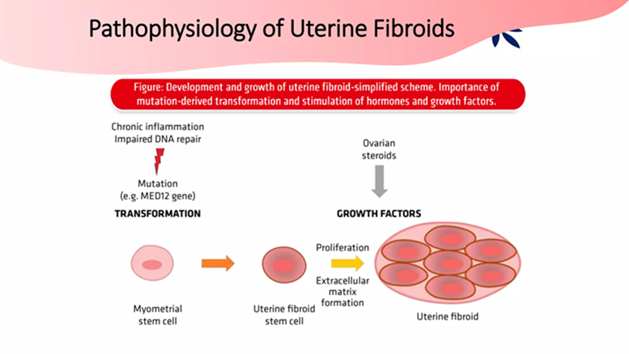
Etiology: Though exact etiology is not known, i) Estrogen has been implicated as Fibroids contain higher estrogen receptors than surrounding myometrium, as their size increases in pregnancy and estrogen therapy, they are not seen before menarche and regress after menopause ii) Progesterone as they increase mitotic activity and reduce apoptosis iii) Fibroids are monoclonal and about 40% have chromosomal abnormality- translocations between chromosomes 12 &14. Overall Fibroids overexpress Estrogens and Progesterone. iv) An analysis of the variability of the COMT gene in 44 patients by PCR-sequencing, showed that the Val158Met polymorphism
(rs4680) is the main cause of variation in COMT activity. This polymorphism is a causal factor in the incidence of uterine fibroids by allowing a higher estrogenic activity in myometrial cells [8].
Pathophysiology of Fibroids: Although Fibroids are benign, can significantly impact on the everyday physical and mental well-being of women. Fibroids are a result of the inappropriate growth of uterine smooth muscle tissue or myometrium. Their growth is dependent on estrogen and progesterone levels. Recent studies indicate involvement of the COMT gene in the occurrence of uterine fibroids.
Diagnosis: Transvaginal ultrasound (TSV) is the gold standard for imaging uterine fibroids with a sensitivity of around 90 to 99%. Saline-infused sonography Ultrasound increases the sensitivity for the detection of subserosa and intramural fibromas. Fibroid appearance is as a firm, well-circumscribed, hypoechoic mass. A simple ultrasound was sufficient in our case.[3]
Hysteroscopy: A hysteroscope is used to visualize the inside of the uterus, allows for better visualization of fibroids inside the uterine cavity and allows for the direct removal of intrauterine growths during the procedure.
Magnetic Resonance Imaging MRI: MRI has the benefit of providing a better picture of the number, size, vascular supply, and boundaries of the fibroids as they relate to the pelvis. It may not be needed routinely on the suspicion of the fibroids are. It has not been shown to differentiate leiomyosarcoma from leiomyoma.
Treatment: Treatment options for symptomatic uterine fibroids include medical, surgical, and radiologically guided interventions. Although curative treatment of this tumor relies on surgical therapies, medical treatments are considered the first-line treatment to preserve fertility and avoid or delay surgery. Treatment for patients must begin with trials of NSAIDs and hormonal therapy, and escalated only when symptoms are refractory, or unmanageable by medication. Minimally invasive treatment (hysteroscopic Myomectomy) options performed by gynaecologists or interventional radiologists can be an option if there is a need to preserve uterus. Hysterectomy is the definitive treatment for leiomyomas and must be opted for patients with high severity of symptoms, who do not mind infertility.
Currently among medical therapy tow possibilities are there, 1) Hormonal therapy consists of gonadotrophin-releasing hormone (GnRH) {GnRH agonists, GnRH antagonists}, Androgens (Danazol), Levonorgestrel releasing intrauterine system and selective progesterone receptor modulators (SPRMs- Ulipristal Acetate and Mifepristone) and 2) non-hormonal therapy Tripterygium Wilfordii, Epigallocatechin gallate (EGCG) and Vitamin D are the most effective medical therapies. Medical treatment needs repeated consultations and interventions.
GnRH agonists drugs include Leuprolide, goserelin, triptorelin and histrelin, they are synthetic GnRH products structurally analogous to natural GnRH, reduce Fibroid size by 30-40%. However, they have side effects of exacerbation of symptoms, development of vasomotor symptoms, and decreased Bone density.
The predominant GnRH antagonist is Degarelix.
Evidence is split as far as their ability of reduction of fibroid volume /size, but there in agreement on its effectiveness in preventing further growth of the tumour and menstrual bleeding significantly [3,4]
Incidence of fibroids is most common in 31-40 years of age i.e. 34.9%. Commonly observed symptoms were abdominal lump (41%) and abnormal uterine bleeding (24.1%).
In a prospective clinical observation to evaluate the efficacy of Ormeloxifene in uterine fibroid in reproductive age group were studied for primary outcomes of i) fibroid size, ii) uterine size, and iii) delta size and secondary outcomes of Secondary outcomes i) menstrual blood loss using the PBAC score, ii) hemoglobin concentration and iii) endometrial thickness. Forty-four (44) women aged 20–50-year age group diagnosed with fibroid uterus as outpatient cases. Both symptomatic and asymptomatic were given Ormeloxifene 60 mg was given orally twice a week for 6 months. Follow up after 6 months clinically and by USG. The Results showed i. No significant changes in the leiomyoma, uterine and delta size, ii) 91% fibroids remained unchanged at the end of 6 months. The difference in mean hemoglobin concentration, PBAC scores and endometrial thickness were reduced statistically significant (p<0.001). Hysterectomy was required in 5 (11.36%) cases. The inference was Ormeloxifene does not reduce fibroid size but prevents further growth of the tumour and significantly reduces menstrual blood loss in standard doses with minimum side effects for a short period [3].
Another study compared the effect of mifepristone and Ormeloxifen on symptomatology, size, and vascularity of fibroid and to compare the compliance and side effects of both these drugs in Allahabad, India, over a period of one year between 2016-2017 in 90 fibroid patients. Group A included 44 fibroid patients who were given mifepristone and Group B included 46 fibroid patients who were given Ormeloxifen by choice of the patients. Assessment of heavy menstrual bleeding by pictorial blood loss assessment chart, dysmenorrhea and dyspareunia by visual analogue scale, estimation of hemoglobin and repeat imaging to assess size, number, endometrial thickness, Doppler velocimetry of fibroid was done. Results showed that 97.7% patients in group A and 95.6% patients in group B were compliant towards treatment. Mifepristone and Ormeloxifen were equally effective for symptomatic relief in fibroid patients. Myoma size was significantly reduced by mifepristone only, with notable endometrial hyperplasia whereas Ormeloxifen causes significant reduction in endometrial thickness. No major side effects observed with any of them.
Non-hormonal Therapy: Tripttergium wilfordii decreases numbers and expressions of Progesterone and estrogen Receptors and decreases Aromatase Enzyme. It may be an effective therapy with few side effects.
EGCG (45%) decreases severity of symptoms and health related quality of Life Index Vit D3 with EGCG have shown reduction of volume after 4 months of treatment.
Botanical drugs are gaining attention in this era due to their cost effectiveness with a comparable and more potent therapeutic efficacy while demonstrating lesser adverse effects. A total of five botanical drugs and three polyherbal formulations have been reviewed which have potentials of becoming an alternative treatment choice for uterine fibroids. However, a validated testing protocol is needed to standardize the active constituents in botanical drug products for use as a uterine fibroid treatment in ensuring a reproducible therapeutic effect [9].
Conclusion:
Uterine Fibromas are commonest benign tumours of muscles and fibrous tissue in the walls of the Uterus affecting one third of the fertile women.
In India the incidence of fibroids is most common in women of 31- 40 years of age
Recent understanding of etiology suggests increased number of estrogen and Progesterone Receptors, increased COMT gene expression and TGF-B3
Treatment must be individualized based on age, signs & symptoms, sustained reduction of the size and sustenance of fertility if desired with minimal side effects.
Medical Therapies are both hormonal and non-hormonal and in near future some botanical drugs.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
