
Case Report | DOI: https://doi.org/10.31579/2768-2757/137
1General Surgeon, Department of Surgery, Medical Faculty, Zahedan University of Medical Sciences and Health Services, Zahedan, Iran.
2Associated professor of nephrology, Department of Internal medicine, Nephrologist, Ali Ibne Abitaleb Hospital, Zahedan University of medical Sciences, Zahedan, I.R. Iran.
3Dentist, Dental faculty, Zahedan University of Medical Sciences and Health Services, Zahedan, Iran.
*Corresponding Author: Ahmad Reza Shahraki., General Surgeon, Department of Surgery, Medical Faculty, Zahedan University of Medical Sciences and Health Services, Zahedan, Iran.
Citation: Ahmad R. Shahraki, Elham Shahraki, Elahe Shahraki, (2024), Meckel's Diverticulum and Complications in A 75 Years Old Man: A Case Report, Journal of Clinical Surgery and Research, 5(6); DOI:10.31579/2768-2757/137
Copyright: © 2024, Ahmad Reza Shahraki. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 13 August 2024 | Accepted: 03 September 2024 | Published: 19 September 2024
Keywords: Meckel’s diverticulum
Meckel’s diverticulum (MD) is a congenital outpouching or bulge in the lower part of the small intestine. It is the most common congenital defect of the gastrointestinal tract. MD is usually asymptomatic but when symptomatic, typically presents in childhood. Meckel’s diverticulum is the most common congenital anomaly of the gastrointestinal system. It originates from failure of the vitelline duct to obliterate completely, which is usually located on the antimesenteric border of the ileum. Its incidence is between 1% and 3%. Meckel’s diverticulum occurs with equal frequency in both sexes, but symptoms from complications are more common in male patients. Most of the Meckel’s diverticula are discovered incidentally during a surgical procedure performed for other reasons. Hemorrhage, small bowel obstruction, and diverticulitis are the most frequent complications.
This case was a 75 years old male with abdominal pain and signs and symptoms of acute appendicitis that in surgery has a complicated Meckel's diverticulum that resected and anastomosis of small intestine was done and discharge with no complication and healthy.
In summary, although Meckel’s diverticulum is the most prevalent congenital abnormality of the gastrointestinal tract; it is often difficult to diagnose. The complications of Meckel’s diverticulum should be taken into account in the differential diagnosis of small bowel obstruction. Surgical resection has always been the treatment of choice in symptomatic MD. However, there has been debate about the proper management of asymptomatic MD if incidentally discovered during laparotomy or laparoscopy. Fewer studies discouraged the prophylactic removal of MD.
Meckel’s diverticulum (MD) is a congenital outpouching or bulge in the lower part of the small intestine. It is the most common congenital defect of the gastrointestinal tract. MD is usually asymptomatic but when symptomatic, typically presents in childhood [1]. Meckel's diverticulum (MD) is the most common congenital anomaly of the gastrointestinal tract. Most cases are asymptomatic and when symptomatic, preoperative diagnosis of MD is poor. Intestinal obstruction, Malena or hematochezia, and inflammation are major symptoms [2]. Meckel's diverticulum (MD) is the most common congenital anomaly of the gastrointestinal tract that ensues as a result of partial closure and persistence of the vitelline, or the omphalomesenteric duct during embryogenesis [3]. It is a true diverticulum containing all the layers of the small intestine and is known to contain ectopic gastric mucosa [4]. The reported prevalence of MD is between 0.3% and 2.9% of the general population and its frequency is higher in male patients than in females with a ratio of 1.5:1–4:1 [5,6]. Meckel’s diverticulum is the most common congenital anomaly of the gastrointestinal system. It originates from failure of the vitelline duct to obliterate completely, which is usually located on the antimesenteric border of the ileum. Its incidence is between 1% and 3%. Meckel’s diverticulum occurs with equal frequency in both sexes, but symptoms from complications are more common in male patients. Most of the Meckel’s diverticula are discovered incidentally during a surgical procedure performed for other reasons. Hemorrhage, small bowel obstruction, and diverticulitis are the most frequent complications [7]. Histologically, heterotopic gastric and pancreatic mucosas are frequently observed in the diverticula of symptomatic patients. Involvement of the mesodiverticular band of the diverticulum is rarely seen. This case report presents the diagnosis and management of a small bowel obstruction due to mesodiverticular band of a Meckel’s diverticulum [8].
Key words: Adult meckel’s diverticulum, acute intestinal obstruction, diverticulectomy, Meckel's diverticulum, Gastroenterology, Congenital diverticulum.
This case is a 75 years old male with abdominal pain that referred to surgery part with abdominal pain. We admit him and start examination that has low grade fever, RLQ tenderness, leukocytosis, nausea and vomiting but no evidence of peritonitis. Ultrasonography shows evidence of The acute appendicitis and surgery perform for him with diagnosis of acute appendicitis that in surgery we face with complicated Meckel’s diverticulum (MD) (figure1,2). We resect small bowel part contains complicated Meckel’s diverticulum (figure3), and anastomosis did. After surgery we follow and observe he and he tolerate PO on third days after surgery and we discharge him 5 days after admission healthy.
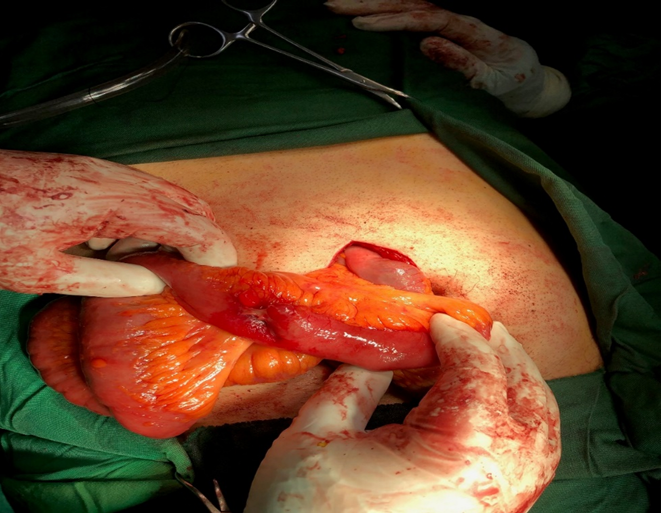
Figure 1: complicated Meckel’s diverticulum (MD).

Figure 2: complicated Meckel’s diverticulum (MD).
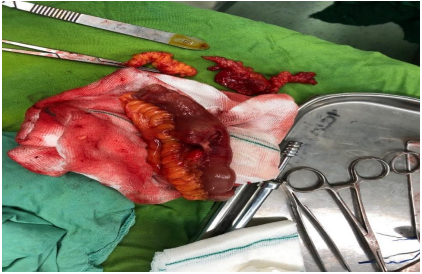
Figure 3: Resected complicated Meckel’s diverticulum (MD).
Meckel’s diverticulum was originally described by Fabricius Hildanus in 1598. However, it is named after Johann Friedrich Meckel, who established its embryonic origin in 1809. Meckel’s diverticulum is the most common congenital anomaly of the small intestine, with a prevalence of approximately 1-3%, and is a true diverticulum containing all layers of the bowel wall. The average length of a Meckel’s diverticulum is 3 cm, with 90% ranging between 1 cm and 10 cm, and the longest being 100 cm. This diverticulum is usually found within 100 cm of the ileocaecal valve on the antimesenteric border of the ileum. The mean distance from the ileocaecal valve seems to vary with age, and the average distance for children under 2 years of age is known to be 34 cm. For adults, the average distance of the Meckel’s diverticulum from the ileocaecal valve is 67 cm. Most cases of Meckel’s diverticulum are asymptomatic, and the estimated risk of developing lifetime complications of Meckel’s diverticulum is around 4% (9). Most patients are asymptomatic and the diagnosis is difficult to confirm preoperatively. Among the symptomatic patients, two types of heterotopic mucosa (gastric and pancreatic) are found histologically within the diverticula. The frequent complications of Meckel’s diverticulum are hemorrhage, intestinal obstruction and diverticulitis. Intestinal obstruction is the second most common complication of Meckel’s diverticulum [10]. There are plenty of mechanisms for bowel obstruction arising from a Meckel’s diverticulum. Obstruction can be caused by trapping of a bowel loop by a mesodiverticular band, a volvulus of the diverticulum around a mesodiverticular band, and intussusception, as well as by an extension into a hernia sac (Littre’s hernia) [11]. Similarly, as in our case; obstruction can be caused by trapping of a bowel loop by a mesodiverticular band. The important aspect of our case is clear demonstration of the mesodiverticular band of a Meckel’s diverticulum. Various imaging modalities have been used for diagnosing Meckel’s diverticulum. Conventional radiographic examination is of limited value. Although of limited value, sonography has been used for the investigation of Meckel’s diverticulum. High-resolution sonography usually shows a fluid-filled structure in the right lower quadrant having the appearance of a blind-ending, thick-walled loop of bowel [12]. On computed tomography (CT), Meckel’s diverticulum is difficult to distinguish from normal small bowel in uncomplicated cases. However, a blind-ending fluid or gas-filled structure in continuity with the small bowel may be revealed [13]. Abdominal CT is used for complicated cases such as intussusceptions. CT can help to confirm the presence of intussusception and distinguish between lead point and non-lead point intussusceptions [14]. In asymptomatic patients; whether all cases of incidental Meckel’s diverticula should be resected or not is an unresolved question. On the other hand, for the symptomatic patients; treatment should always include resection of the diverticulum or the segment of the bowel affected by the pathology [15]. MD can present with various complication spectrums, including small-bowel obstruction, peritonitis, and severe iron-deficiency anemia, which may cause difficulty in definitive diagnosis, particularly in children. Segmental small-bowel resection and primary anastomosis are effective surgical approaches and show good outcomes for MD patients [17].
In summary, although Meckel’s diverticulum is the most prevalent congenital abnormality of the gastrointestinal tract; it is often difficult to diagnose. The complications of Meckel’s diverticulum should be taken into account in the differential diagnosis of small bowel obstruction. Surgical resection has always been the treatment of choice in symptomatic MD. However, there has been debate about the proper management of asymptomatic MD if incidentally discovered during laparotomy or laparoscopy. Fewer studies discouraged the prophylactic removal of MD (16). Most of the MD are asymptomatic but when clinical manifestations arise from complications like obstruction, bleeding, or diverticulitis, MD must be included in the differential diagnosis. Young patients with small bowel obstruction are rarely diagnosed prior to surgery because of its indistinguishable features from other intraabdominal pathologies. The standard treatment of MD is definitive surgery, including diverticulectomy or ileal resection. Early surgery is required in order to prevent strangulation or gangrene. Significant morbidity and mortality can be prevented when clinicians promptly act to diagnose MD and manage it on time. There are several surgical approaches for MD, such as segmental small-bowel resection including MD and diverticulectomy only [18]. Some surgeons prefer to perform segmental small-bowel resection, including MD, because they want to include any possible intestinal ulceration within the resection samples, while other surgeons choose the latter because they consider that the ulcerated ileum is close to the ectopic gastric mucosa [18]. In conclusion, MD can present as various complication spectrums, including small-bowel obstruction, peritonitis, and severe iron-deficiency anemia, which may cause difficulty in definitive diagnosis, particularly in children. Segmental small-bowel resection with primary anastomosis are effective surgical approaches and show good outcomes for patients with MD. The diagnosis should be considered in any patient with abdominal discomfort without other explanation, nausea and vomiting or gastrointestinal bleeding. Treatment of symptomatic Meckel’s diverticulum is definitive surgery including diverticulectomy, wedge resection and segmental resection; the procedure depends on the integrity of diverticulum base and adjacent ileum [19]. In addition, it is also important to always try to expand the cavity inventory in the intraoperative period, especially in the absence of explanations for the previous clinical findings, with mandatory assessment of the small intestine from the ileocecal valve for, at least, the first 100 cm, in order to find a MD and its possible complications [20, 21, 22]. Although rare, its clinical presentation might be similar to acute appendicitis, which restate the importance of collecting a detailed clinical history and examining the small bowel in order to investigate a possible Meckel’s diverticulum complication in the differential diagnosis [23]. Although relatively rare in adults, MD should be considered in the list of differentials in patients with intussusception leading to SBO, especially on a background history unremarkable for the most common etiologies causing SBO including post-operative adhesions and hernias [24]. Laparoscopy can be useful in the diagnosis and treatment of Meckel’s diverticula. In addition, the laparoscope can be used to remove incidentally discovered diverticula [25].: Meckel’s diverticulum can be difficult to diagnose and require a higher level of suspicion. Although Meckel’s diverticulum is uncommon in adults, it should be considered a cause of small bowel obstruction [26].
Ethical Approval and Consent to participate:
The content of this manuscript is in accordance with the declaration of Helsinki for Ethics. No committee approval was required. Oral and written consent to participate was granted by her Family.
“Written informed consent was obtained from the patient's legal guardian for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.”
It is available.
The author declares that they have no competing financial interests and nothing to disclose.
There is no funding.
Surgical resection has always been the treatment of choice in symptomatic MD. However, there has been debate about the proper management of asymptomatic MD if incidentally discovered during laparotomy or laparoscopy. Fewer studies discouraged the prophylactic removal of MD.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
