
Review Article | DOI: https://doi.org/10.31579/2637-8892/241
Indian Ports Association, Indian Statistical Institute, Indian Maritime University
*Corresponding Author: Satyendra Nath Chakrabartty, Indian Ports Association, Indian Statistical Institute, Indian Maritime University.
Citation: Satyendra N. Chakrabartty, (2024), Measurement Issues in Mental Health, Psychology and Mental Health Care, 8(1): DOI:10.31579/2637-8892/241
Copyright: © 2024, Satyendra Nath Chakrabartty. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 11 December 2023 | Accepted: 27 December 2023 | Published: 09 January 2024
Keywords: mental health; likert items; geometric mean; cosine similarity; monotonic; responsiveness
The paper discusses limitations of existing self-reported measures of mental health and suggests transforming ordinal item scores to continuous, monotonic scores satisfying desired properties including meaningful aggregation. Here, an item scores with response-categories marked as 1, 2, 3, 4, 5, and so on are combined by [1] transforming to normally distributed scores, [2] angular similarity and [3] function of Geometric Mean (GM) for measuring mental health of individuals. Each proposed measure avoids selection of weights, scaling and considers all chosen domains, even if they have different correlations with scale scores. Each method can identify poorly performing domains and assess overall improvement/decline of a patient across time. However, changes over time need to be validated with clinical findings. Proposed mental health scores help better comparisons, ranking, classifying and testing of mean and variance for a sample. Approach [3] may be preferred for additional features like constant domain-elasticity, time-reversal test, chain indices.
Mental Health (MH), an integral part of general health and well-being is a basic human right (WHO, 2022). Measurement of multidimensional Mental Health is complex because of differences in cultures and social and psychological confounders, methodological limitations of measurement from scales/tests, etc. Psychological, social and behavioral features associated with mental illness vary in conceptualizations and are difficult to measure. Measurement of Mental Health is complex because of its multidimensional nature, differences in cultures and social and psychological confounders, methodological limitations of measurement from scales/tests, etc. Psychological, social and behavioral features associated with mental illness vary in conceptualizations and are difficult to measure. Need for community-based MH systems and services were outlined by World Health Organization (2021). Measurement issues of MH are important for accurate diagnosis, assessing severity; monitoring, tracking path of recovery of both individuals and sample. MH systems and services were outlined (WHO, 2022). Measurement issues of MH are important for accurate diagnosis, assessing severity; monitoring, tracking path of recovery of both individuals and sample. Attempts to measure outcomes of MH frequently using International standards for diagnosis of mental illnesses are: International Classification of Disease version 10 (ICD-10) and Diagnostic Statistical Manual version 5 (DSM-V). However, DCM–V contains heterogeneous diagnostic categories since pragmatic criteria undermine the diagnostic model (Kate et al. 2019). Structured Clinical Interview for DSM-IV and Best-estimate consensus diagnoses showed poor agreements and use of diagnostic interviews in clinical contexts are questionable (Kvig and Nilssen, 2023).Major purposes of such tools are to identify cases, screen those at risk of developing mental disorder and monitor the progress, classify, compare and rank individuals and also to track impact of interventions/ treatments. While diagnostic tools assess clinical symptoms involving clinical interviews and multi-expert assessments, screening tools attempt to assess severity of a mental health disorder and track changes of one or a group of patients or response to treatments.
Commonly used tools to assess MH include:
Self-assessed scales and interviews cover a limited range of problems like anxiety and depression and may not capture isolated, short-lived cases or mild-cases requiring early treatments.. Major concerns are scoring based on nature of data generated from such MH measuring tools and non-satisfaction of properties like monotonically increasing continuous scores along with their responsiveness, reliability, sensitivity, specificity, etc. Significant variations in the questionnaires for 16 common depression identification tools were found (Williams et al. 2002).
The paper aims at reviewing limitations of existing self-reported measures of mental health and suggesting transformations so that the transformed scores facilitate meaningful application of operations and satisfy desired properties of measurement.
Literature survey:
Tolls for assessing MH differ in terms of number and format of items, scoring methods, dimensions considered viz. clinical (depression, anxiety, schizophrenia, etc.) and social (social support, etc.), and are not comparable. For example, 109 different measurement tools in health literature were identified for social isolation only (Cordier, 2017). Illustrative assessment tools along with their uses, features and observations are given in Table-1.

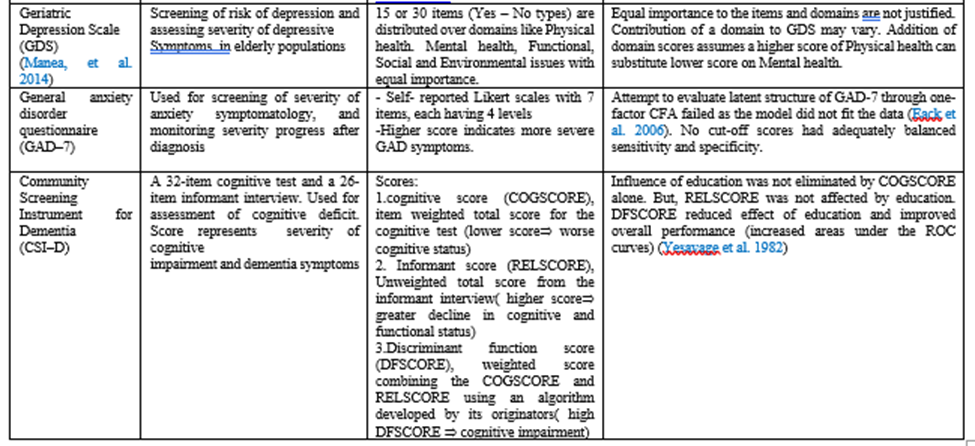
Table 1: Illustrative Assessment Tools
Table 1: Illustrative Assessment ToolsObservations:
Most of the MH assessing tools use summative scores of Likert items/NRS suffer from following limitations:
 is meaningless. Use of mean and SD for ordinal scales was disfavored (Liu et al. 2005).
is meaningless. Use of mean and SD for ordinal scales was disfavored (Liu et al. 2005).Possible solutions:
Major limitations of Kappa and weighted Kappa or kappa reliability coefficient as used in K 6 and K 10 to find degree of agreement among the raters are:
 may be surmised as large volume of incorrect evaluation of data (Simundic, 2008). For ordered categories, methods of deciding weights for weighted kappa vary and may give different values of weighted kappa.
may be surmised as large volume of incorrect evaluation of data (Simundic, 2008). For ordered categories, methods of deciding weights for weighted kappa vary and may give different values of weighted kappa.Other Limitations:
SF-36 was negatively correlated with GAD 7 and PHQ, presumably due to different domains measured by each of them. Multi-domains MH tools give equal importance to the domains. Such equal importance or no weights amounts to a compensatory approach, without differentiating essential and less important domains. As a result, low score of one domain gets countered by a high score of other domain. Theoretically, the domains may be given weights (considering relative importance of domains) and take MH score (Y) as a weighted sum. Here, ‘trade-off’ between a pair of domains since  is the amount of domain-2 that needs to be sacrificed to gain an extra unit of domain-1. Weights from Principal Component Analysis (PCA) poorly weigh those items which do not have strong correlations with Y, even if they are theoretically and practically important. Thus, PCA ignores judgments as to what are important. Assumptions of PCA include relatively homogeneous large sample size, normality of item scores, etc. If one variable has a SD which far exceeds the rest the variable, it will dominate the first eigenvector. Moreover, PCA weights vary over time and space and thus comparisons become difficult. No weighting system is above criticism (Greco et al. 2019). Similarly, there is no perfect aggregation scheme.
is the amount of domain-2 that needs to be sacrificed to gain an extra unit of domain-1. Weights from Principal Component Analysis (PCA) poorly weigh those items which do not have strong correlations with Y, even if they are theoretically and practically important. Thus, PCA ignores judgments as to what are important. Assumptions of PCA include relatively homogeneous large sample size, normality of item scores, etc. If one variable has a SD which far exceeds the rest the variable, it will dominate the first eigenvector. Moreover, PCA weights vary over time and space and thus comparisons become difficult. No weighting system is above criticism (Greco et al. 2019). Similarly, there is no perfect aggregation scheme.
Possible solution:
Multi-dimensional MH score (Y) may be defined by cosine similarity between the two vectors showing domain scores of the current period and base period or by geometric mean (GM) of ratios of current domain scores and respective domain score for the base period, to accommodate all relevant domains and facilitate computation of Y for an individual and also for a group of individuals.
Proposed methods:
Ignoring the issues of selection of indicators, following methods are proposed for measurement of multi-dimensional MH score (Y) avoiding scaling of raw data and choosing weights.
Pre-processing of data:
Method 1: For Likert items with equal number of response-categories, method suggested by 33 is described below:
Let  the raw score of the i-th individual in the j-th item, for
the raw score of the i-th individual in the j-th item, for  and
and  For a 5-point item,
For a 5-point item,  1, 2, 3, 4 and 5.
1, 2, 3, 4 and 5.
I: For i-th item find positive weights ( which are different for different levels and
which are different for different levels and  satisfying the equidistant condition i.e.
satisfying the equidistant condition i.e.  forms an Arithmetic Progression. A positive value of the common difference will ensure
forms an Arithmetic Progression. A positive value of the common difference will ensure 
One way to find such weights are:
i) Let  be the frequency of i-th item for the j-th level. For each item, find maximum (
be the frequency of i-th item for the j-th level. For each item, find maximum ( and minimum frequency (
and minimum frequency (
ii) Find proportions  . Note,
. Note, 
 = 1.
= 1.
iii) Put initial weights . Find the common difference
. Find the common difference 

 .
.
Define ;
; and
and 
Here, and  .
.
iv) Get final weights  =
=  so that
so that 
Weighted sum of raw scores gives equidistant scores (E) and provides meaningful arithmetic aggregations.
II: Normalize the scores obtained at I by 


III: Take further weights to items to satisfy additional property of making the test scores equi-correlated with the items i.e. equal item reliability and thus justify addition of such converted item scores.
Method 2: For Likert scale consisting of subtests consisting of 3-point, 4-point, 5-point, 6-points items.
I: Consider all 3-point items in sub-test 1. Similarly, constitute sub-tests 2, 3, 4 and 5 by considering respectively all 4-point, 5-point, 6-point 7-point items and repeat Stage I of Method 1separately for each sub-test.
7-point items and repeat Stage I of Method 1separately for each sub-test.
II: Take Z- scores for each item. For the i-th item, 
 Sub-test score as a sum of item scores will also follow
Sub-test score as a sum of item scores will also follow 
III: Convert Z-score of an item to  in the range say [1, 100], by:
in the range say [1, 100], by:

 + 1
+ 1
Distributions of item scores for each K-point scale will be normal. However, range of sub-test scores as sum of converted item scores may vary. Variance of sub-test scores will also vary depending on correlations between pair of items.
IV: To have same distribution of different sub-test scores, further transformation may be used as follows:
Modified (


Modified test scores for each K-point scale will be 
 Thus, the K-point subtests for various values of K could be considered as Equivalent Forms having features of parallel tests.
Thus, the K-point subtests for various values of K could be considered as Equivalent Forms having features of parallel tests.
Methodology:
For one-dimensional tools:
Use Method 1 to find Y for a tool which is one-dimensional. For multi-dimensional tool, find scores of a domain consisting of Likert items by the above said method. Such scores of one-dimensional tools or domain scores are continuous satisfying equidistant property with a fixed zero point and has the following advantages:
i. Higher value indicates higher value of MH or domain score
ii. Generate monotonic scores since choice of j-th level will result in higher score than the choice of (j-1)-th level for any item for j =2, 3, 4, 5
iii. Rank a group of patients uniquely avoiding ties unlike the usual summative scores.
iv. Possible to find sample mean and SD for a group of patients.
v. If  denotes severity of the i-th patient in t-th time period, then
denotes severity of the i-th patient in t-th time period, then  will indicate percentage of progress/deterioration registered by the i-th patient in t-th time in comparison to (t-1)-th time period i.e. responsiveness of the scale.
will indicate percentage of progress/deterioration registered by the i-th patient in t-th time in comparison to (t-1)-th time period i.e. responsiveness of the scale.
For multi-dimensional tools:
Let  be the matrix for m-persons and n-domains where each row vector
be the matrix for m-persons and n-domains where each row vector  =
= represents scores of n- domains in the current period of a person. Here,
represents scores of n- domains in the current period of a person. Here, 
 have been obtained after the data pre-processing presented above. Let corresponding base period vector is
have been obtained after the data pre-processing presented above. Let corresponding base period vector is  =
= . Let
. Let
(1) and (2) are simple, avoid scaling and selection of weights. Each of (1) and (2) may be multiplied by 100 for general convention. Each measure satisfies the following:
(2) has additional features like:

 increase in Y if all others remain unchanged.
increase in Y if all others remain unchanged. or
or 
 .
. Chain-indices help to draw path of improvement/decline since the base period.
Chain-indices help to draw path of improvement/decline since the base period.Thus, the proposed method in terms of (2) with higher desirable properties is an improvement over the existent measures.
After reviewing major limitations of measuring mental health, the paper proposed methods of converting item-wise ordinal Likert scores to normally distributed scales, with equal and different number of response-categories for arithmetic aggregation of item scores. For combining domain scores, the paper proposed two indices in terms of angular similarity and function of Geometric Mean (GM) for measuring mental health. Each measure is non-parametric, simple, avoids scaling or finding weights or reduction of dimensionality and considers all chosen domains and indicators. Scores generated by each of the method were continuous, monotonic and assess progress/deterioration of a patient across time. Each depicts overall improvement or decline of a patient or a sample of patients in the current year with respect to base year or on Year-to-Year basis and facilitates better comparison, ranking, classification and assessing paths of progress. However, changes over time need to be validated with clinical findings. Measure based on of angular similarity and function of GM reduce level of substitutability among the indicators, not affected much by outliers and satisfies the principle of population replication. Both satisfy desired properties like monotonically increasing continuous function, assessment of responsiveness, which in turn helps drawing of path of improvement/decline over time. It is possible to compute mean and variance of mental health for a group of persons. Normality helps in estimating/testing population parameters.
Each proposed measure can be used to find mental health scores (Y) of a uni-dimensional tool or domain scores for multi-dimensional tool. GM approach is preferred for its additional features like linearity between gain in a domain and gain in mental health, time-reversal test, easy identification of critical areas requiring attention and contribution of the domains/indicators to the mental health.
Simulation studies with multi dataset to explore issues relating to dimensionality and rank robustness of tools and to find distribution of 
 and relationship between
and relationship between  are suggested for future studies.
are suggested for future studies.
Funding details: No funds, grants, or other support was received
Conflicts of interest/Competing interests: The author has no conflicts of interest to declare
Ethical approval: Not applicable since the paper does not involve human participants.
Consent of the participants: Not applicable since the paper does not involve data from human participants
Data Availability statement: The paper did not use any datasets
Code availability: No application of software package or custom code
Authors' contributions: Sole Author
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
