
Case Report | DOI: https://doi.org/DOI:10.31579/2690-1919/421
1 Department of Oral and Maxillofacial Surgery Plastic Surgery, University of Mainz, Augustusplatz 2, 55131 Mainz, Germany.
2 Institute of Forensic Medicine, University of Freiburg, Albertstr. 9, 79104 Freiburg, Germany.
*Corresponding Author: Sigrun Chrubasik-Hausmann, Department of Oral and Maxillofacial Surgery Plastic Surgery, University of Mainz, Augustusplatz 2, 55131 Mainz, Germany.
Citation: Kaya S., Vlachojannis J., Chrubasik-Hausmann S, (2024), May Phytomedicines Play a Role in Cardiovascular Risk Reduction?, J Clinical Research and Reports, 17(1); DOI:10.31579/2690-1919/421
Copyright: © 2024, Sigrun Chrubasik-Hausmann. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 17 October 2024 | Accepted: 22 October 2024 | Published: 15 November 2024
Keywords: agla cardiovascular risk score; myocardial infarction; cocoa–black garlic extract; coenzyme q10; black seed oil
C.F. suffered myocardial infarction despite low cardiovascular risk as defined by the Swiss Working Group on Lipids and Atheriosclerosis (AGLA). C.F. wished replacement of his synthetic blood pressure lowering and antilipidemic medication by phytomedicines. A combination of standardized cocoa and black garlic extracts with coenzyme Q10 plus black seed oil with 30 mg thymoquinone in the daily dose normalized total cholesterol and maintained low blood pressure. However, the AGLA desired setpoint of LDL cholesterol (below 1.6 mmol/L) was not achieved. Since such low LDL cholesterol concentrations are not necessarily associated with less mortality, we agreed that C.F. continued with the phytomedicines because his quality of life was better than during the intake of the synthetic medications.
AGLA : Swiss Working Group on Lipids und Atheriosclerosis,
CV : Cardiovascular,
HBMP : Home blood pressure measurements,
MI : Myocadial infarction,
Chol : Cholesterol,
CoQ10 : Coenzyme Q10
SD : Standard deviation
There is no doubt that among the herbal armamentarium cocoa [1], black garlic [2] and black seed and its oil [3] have a great impact on cardiovascular (CV) health [1-3]. However, for successful treatment of CV risk factors, an appropriate dose of the active principle in herbal medicinal products are required. Kuna Indians who consume about 900 mg of cocoa flavanols with their daily cocoa beverage do not suffer from arteriosclerosis, hypertension or hyperlipidemia [1]. The daily flavanol dose was recalculated from the content of flavanol metabolites excreted in urine. If Kuna Indians move to America, getting rid of their cocoa beverage habit and eating fast food, their protection from CV risk is gone [1]. Odourless garlic with 2.7 mg of S-allyl-cysteine in the daily dosage has decreased arteriosclerosis, hypertension and hyperlipidemia [2]. The leading substance of black seed and oil, thymoquinone, should be given in a daily dose of 30 mg [4]. We report here a case with the replacement of synthetic CV medication by a mixture of standardized phytomedicines.
In November 2022, male patient C.F. suffered a myocardial infarction (MI) despite his low AGLA (Swiss Working Group on Lipids and Atheriosclerosis) CV risk score of 10
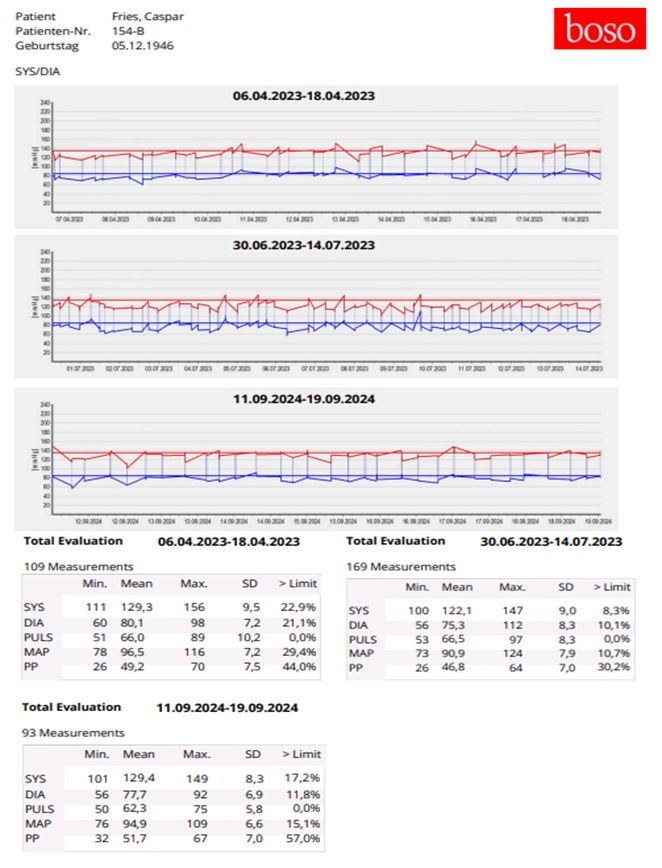
Figure 1: Details of the home blood pressure measurements (SD standard deviation).
According to the AGLA guideline recommendations, the primary care physician started treatment with acetylsalicylic acid 100 mg, ticagrelor 2 x 90 mg, pantoprazol 40 mg, bisoprolol 1.25 mg, lisinopril 2.5 mg and atorvastatin 2 x 40 mg per day. Until January 2023, C.F. received 6 coronary stents. In January 2024, the statin was changed to ezetimibe/rosuvastatin 10/20 mg because of liver enzyme increase (Table 1)
C.F. consulted us in April 2023 because he wished to have replaced synthetic medication by phytomedicines. At that time, total cholesterol (Chol) was 3.6 nmol/L and LDL Chol 1.5 nmol/L (the ideal AGLA guideline setpoint would have been 1.4 nmol/L or lower). On April 6, we started with CardiovascR, a proprietary cocoa-black garlic extract supplemented with coenzyme Q10 (CoQ10), 400 mg of flavanols, 942 mg
black garlic extract* and 200 mg CoQ10/day. During the CardiovascR treatment, total cholesterol increased to 5.3 nmol/L (upper range 5.6 nmol/L) but increased further into the pathological range until January 2024 (Table 1). So, we doubled the CardiovascR dose and added 6 capsules of black seed oil with 3 mg of thymoquinone/day. Since serum total cholesterol increased to 5.7 nmol/L after a drop (5.3 nmol/L) and LDL Chol increased to 3.6 nmol/L in the follow-up until May 2024, we exchanged the black seed oil with an oil with 30 mg of thymoquinone per day. After that, serum total Chol stabilized in the normal range (Table 1) but LDL Chol did not reach the desired AGLA guideline set point of 1.6 mmol/L or below. We discussed this with C.F. who enjoyed the quality of life during the phytomedicine treatment. C.F. wished to continue with the herbal medication, although the AGLA guideline requirement was not fulfilled.
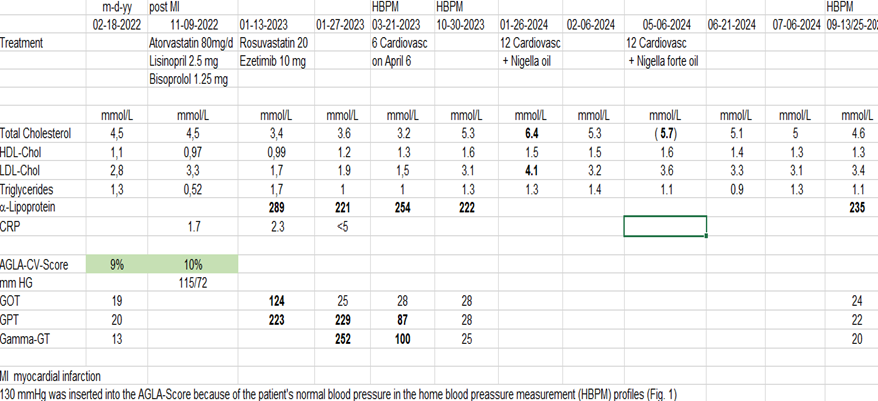
Table 1: Visits, treatment and laboratory values before and after the myocardial infarction.
*The garlic extract was tested at the University of Aachen for its antioxidative effect, which was 10 times higher than that of the aged garlic extract tested in clinical studies [5].
Side headings/Subheadings
Phytomedicines for CV risk reduction
The case report indicates that in individual cases, the AGLA CV Score is not a reliable predictor of high CV risk. C.F. suffered MI despite a low AGLA risk of 10% and when it happened was classified as high CV risk patient [6] and was given treatment according to the AGLA guidelines. When the patient wished to receive herbal replacement for this treatment, we started with a combined cocoa and black garlic extract supplemented by CoQ10 and, according to the patient’s total cholesterol, increased the dose of active principle or added other options (Table 1). Dose-finding studies are now required to evaluate the optimum dose of the individual components, including CoQ10 [7].
CoQ10 is one of the dietary antioxidants with a high tolerability and safety profile [8-10]. By adding 120 mg CoQ10 to 1200 mg of odourless black garlic extract, vessel elasticity and endothelial function had improved compared to placebo [11] and arterial calcification assessed by computer tomography and the proinflammatory marker C-reactive protein had decreased [12]. In patients with chronic heart insufficiency and impaired left ventricular ejection rate, a dose of >100 mg CoQ10 daily over 6 months reduced CV mortality by 55% [13]. Especially patients with hyperlipidemia and diabetes mellitus profited from an additional 100 or 200 mg CoQ10 [14]. A systematic review and meta-analysis including 12 studies (650 patients) suggested that the CoQ10 primary prevention in diabetic patients was caused by the CoQ10-induced decrease of total and LDL Chol [15].
Future studies must clarify why about 30 percent of the population or more do not respond to odourless garlic extract with a decrease of CV risk factors [16]. It may well be that a genetic Chol disorder is one of the reasons. Likewise, non-response to cocoa extract has been observed [17, 18] and also to black seed preparations [19]. In a systematic review, the impact of black seed (oil) on blood pressure was lower than that known from black garlic and cocoa preparations [20]. Unfortunately, the articles
did not state the thymoquinone content in the daily dosages. We suppose that a daily dose of 30 mg of thymoquinone is a potent and safe CV risk-lowering medicine and/or drug enhancer for other phytomedicines [4]. This should be elucidated in further studies. It also remains to be showand n which signaling pathways are involved in the mechanism of action to which extent supplemental CoQ10 might increase the responsiveness to the phytomedicine mixture in non-responders.
In a retrospective cohort study over a median follow up of almost 6 years, the lowest LDL Chol group (< 1.8 nmol/L) had a higher risk of all-cause, CV disease and cancer mortality compared to the reference group gained from data on CV mortality validated in another independent cohort (LDL Chol 3.1 - < 3.6 nmol/L, 21). This had already been observed by Penson et al. [21] who showed in addition that low hs-CRP appeared to be associated with reduced risk of incident CV disease and mortality in a high-risk population. The low hs-CRP values in the case of C.F. did not indicate an associated inflammatory process. However, the “lipid paradox” that too low level of LDL Chol do not always confer protective effects on mortality outcomes in the population with high CV risk does not oppose continuing with the phytomedicines at least as long as the LDL Chol remains in the range of 2.6 to 3.6 nmol/L. The beneficial effect of LDL Col below 1.6 nmol/L is not yet proven beyond doubt [22]. The number of patients to be treated for one patient to profit from intensive LDL Chol lowering treatment is very high [6] and may not outweigh the inferior quality of life. In contrast to colchicine as co-treatment for LDL Chol reduction [23], standardized cocoa-black garlic extracts with CoQ10 and black seed oil were well tolerated and adverse events are not expected.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
