
Research Article | DOI: https://doi.org/10.31579/2690-4861/165
1 D Amico Foundation for Renal Disease Research, Milan, Italy, Retired from Nephrology and Dialysis Unit, Azienda Ospedaliera Ospedale San Carlo Borromeo, Milan, Italy.
*Corresponding Author: Claudio Bazzi, D Amico Foundation for Renal Disease Research, Milan, Italy.
Citation: C Bazzi. (2021). May be Urinary Excretion of α2-macroglobulin (mw 720 kda) a Proteinuric Marker of Podocytopathy? Insight from Analysis of 204 Patients with Glomerulonephritis (gn) and Nephrotic Syndrome, 177 with Functional Outcome. International Journal of Clinical Case Reports and Reviews. 8(3); DOI:10.31579/2690-4861/165
Copyright: © 2021 Claudio Bazzi, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 19 August 2021 | Accepted: 01 September 2021 | Published: 04 September 2021
Keywords: urinary excretion; α2-macroglobulin; proteinuric marker; podocytopathy; glomerulonephritis; nephrotic syndrome
Background: In IgAN with cellular crescents (CIgAN) urinary excretion of α2-macroglobulin (α2m/C, MW 720 kDa) may be a marker of podocytes damage induced by crescents. The purpose of the study was the evaluation of the clinical significance of α2m/C excretion in 177 patients with glomerulonephritis (GN), nephrotic syndrome (NS) and functional outcome.
Methods: In all 177 patients α2m/C excretion was measured; the patients were divided in 2 groups: α2mC=0 (n. 72) and α2m/C >0 (n. 105); for each group were assessed the outcomes considered in combination: Remission & persistent nephrotic syndrome (PNS) with long lasting NRF designed “Remission & NRF”; ESRD & eGFR < 50% & PNS with CRF designed “Progression and progression risk”.
Results: In 72 patients with α2m/C=0 “Remission & NRF” was 78% and “Progression & progression risk” was 22%; in 105 patients with α2m/C>0 “remission & NRF” was 52% and “Progression & progression risk” was 48%. “Remission & NRF” in each GN type with α2m/C=0 was: 100% in MCD and LN; 82%, 79%, 67% in FSGS, IMN, MPGN; in α2m/C>0 “Progression and progression risk” was 0%, 38%, 46%, 54%, 56%, 85% in MCD, LN, IMN, MPGN, FSGS, CIgAN with cellular crescents, respectively.
Conclusion: Urinary excretion of α2m is a very simple marker available in all clinical practice laboratories, marker of damage of podocytes at least in CIgAN and LN with crescents and marker of GFB damage in different GN types and useful to predict outcome and treatment responsiveness.
In 2001 Bakoush et al. published the article “High proteinuria selectivity index based upon IgM (IgM-SI) is a strong predictor of poor renal survival in glomerular diseases” [1]. The study included 84 patients with glomerulonephritis (between them also IgAN and nephroangiosclerosis) without indication if all patients have nephrotic syndrome (NS). Among patients with high IgM-SI (n. 51) or low IgM-SI (n. 33) 11(22%) with high IgM-SI and 0% with low IgM-SI started dialysis after a follow up of 39 and 43 months, respectively. The Authors concluded that IgM‐SI value is a strong predictor of clinical outcome in proteinuric glomerulopathies. In subsequent 20 years unfortunately no one study evaluated the clinical significance of urinary excretion of the other high MW proteins α2m (MW 720 kDa) whose excretion presuppose a severe alteration of glomerular filtration barrier (GFB). In a recent study [2] we assessed the urinary excretion α2m/C in 58 patients with Crescentic IgAN (CIgAN) (37 with cellular and 21 with fibrous crescents) and in 125 patients with IgAN and persistent non-nephrotic proteinuria (PP). The comparison of urinary excretion of α2m/C between the 58 CIgAN patients and 125 IgAN PP patients showed that α2m/C excretion in CIgAN was 12.9 times higher than in IgAN PP (6.3 vs 0.49, p=0.0002) and 18.2 times higher in 37 CIgAN patients with cellular crescents versus 125 IgAN PP patients (8.94 versus 0.49, p= 0.0003). The comparison between 37 patients with cellular crescents and 21 patients with fibrous crescents showed that α2m/C was 7.07 times higher in patients with cellular crescents (8.94 vs 1.38, p = 0.001). In 21 patients with CIgAN and fibrous crescents compared with 125 patients with IgAN PP α2m/C excretion was 2.82 times higher (1.38 vs 0.49, p = 0.22). The functional outcome was assessed in 34 of 37 patients with cellular crescents and evaluated according to quartiles of cellular crescents and α2m/C. The quartiles of cellular crescents showed a progressive increase of percentage of glomeruli with cellular crescents from 1° to 4° quartile (from 6.2 to 41.8%, p= 0.0006); the quartiles of α2m/C show a significant increase of α2m/C from 2.9 to12.2 (P= 0.04). In 1° quartile of α2m/C remission with normal renal function was 67% and ESRD was 0%, while in 4° quartile Remission with NRF was 0% and ESRD 62.5%. By contrast, the functional outcome of quartile of cellular crescents shows different predictive value: in 1° quartile Remission with NRF 54% and ESRD 31%; in 4° quartile Remission with NRF 22% and ESRD 11%. This difference may be dependent on that α2m/C excretion assess the overall GFB damage, while the percentage of glomeruli with cellular crescents may be dependent on the various size of biopsy samples in different patients. On the basis of these data it was hypothesized that cellular crescents localized in the space between parietal epithelial cells of Bowman capsule and podocytes may damage the podocytes and slit-diaphragm [3, 4, 5] allowing the passage of the high MW protein α2m/C. Thus it may be suggested that α2m/C excretion could be a proteinuric marker of podocyte damage consequent to presence of cellular crescents. On the basis of these data the purpose of the study was the evaluation of the urinary excretion of α2m/C in a large cohort of patients with GN (n. 177) to assess the clinical significance of α2m excretion: whether urinary excretion of α2m may be a marker of podocytopathy in GN with crescents and/or marker of GFB damage in GN patients without crescents.
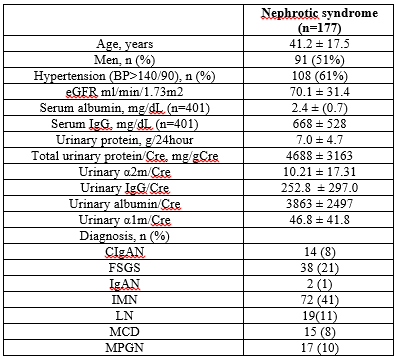
The patients cohort included all patients attending the Nephrology and Dialysis Unit of San Carlo Borromeo Hospital, Milan, Italy, between January 1992 and April 2006 with renal biopsy diagnosis of GN with NS (n. 204); in 177 of them the functional outcome was available and these patients were the object of the study with the following types of chronic primary glomerulonephritis (GN) and Lupus Nephritis (LN) (Table 1): Focal Segmental Glomerulosclerosis (FSGS, n. 38) (6), Idiopathic Membranous Nephropathy (IMN, n.72) (7), Minimal change disease (MCD, n. 15), Membrano-proliferative glomerulonephritis (MPGN, n. 17: type I n. 11; type II n. 1; type III n. 3; fibrillary type n. 29) (8); Crescentic IgAN (CIgAN, n. 14)] and Lupus Nephritis [LN, n. 19: (LN classes: 3+5 n. 2, 4 n. 15; 5 n. 2)]; IgA Nephropathy (IgAN n. 2). Inclusion criteria: nephrotic syndrome (proteinuria ≥3.5 g/24h); at least six glomeruli in renal biopsy; typical features at light and immunofluorescence microscopy; no clinical signs of secondary GN except for LN. The functional outcome was available for all the 177 patients with rather long follow up: mean 86±72 months (2-331). Five types of outcome were considered: 1) Remission of NS: complete: proteinuria ≤ 0.30 g/24h; partial: proteinuria ≤ 2.0 g/24h; 2) persistent NS with long lasting normal renal function (NRF) [follow up: 77±53 months (12-200)]; 3) progression to end-stage renal disease (ESRD) ; 4) eGFR reduction ≤ 50% of baseline; 5) persistent NS with chronic renal failure (CRF) and progressive eGFR reduction (from 49.3 to 39.1 ml/min/1,72 m2). Usually in prediction studies the outcomes considered are Remission and ESRD. We decided to evaluate not only each type of outcome considered independently but also the combination of outcomes with similar prognostic significance: Remission was evaluated in combination with persistent NS with long lasting NRF, afterwards indicated as “Remission & persistent NRF”; ESRD and eGFR ≤ 50% were evaluated in combination with persistent NS with CRF characterized by eGFR progressive reduction and thus candidate for progression to ESRD, afterwards indicated as “Progression & progression risk”. The diagnosis and clinical presentation of patients are reported in Table 1.
Proteinuria was measured in 24 hour urine collection and second morning urine sample by the Coomassie blue method (modified with sodium-dodecyl-sulphate) and expressed as 24/hour proteinuria and protein creatinine/ratio (mg urinary protein/g urinary creatinine). Serum and urinary creatinine were measured enzymatically and expressed in mg/dL. Serum albumin and IgG and urinary IgG , α2-macroglobulin (α2m), Albumin and α1-microglobulin (α1m) were measured by immunonephelometry; urinary proteins were expressed as urinary protein/creatinine ratio (IgG/C, α2m/C, Alb/C, α1m/C). Estimated glomerular filtration rate (eGFR) was measured by the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) formula (9) Three types of renal lesion that are markers of disease severity in any type of GN were evaluated: percentage of glomeruli with global glomerulosclerosis (GGS%); extent of tubulo-interstitial damage (TID) evaluated semi-quantitatively by a score: tubular atrophy, interstitial fibrosis and inflammatory cell infiltration graded 0, 1 or 2 if absent, focal or diffuse (TID global score: 0-6) and extent of Arteriolar Hyalinosis (AH) evaluated semiquantitatively by a score: 0, 1, 2, 3 if absent, focal, diffuse, diffuse with lumen reduction, respectively (AH global score 0-4).
Continuous variables are expressed as means±SD. Categorical variables are expressed as the number of patients (%). The differences of mean were determined by t-test; categorical variables by the chi-square test. All statistical analyses were performed using Stata 15.1 (StataCorp LP, TX, USA). Two-sided p<0>
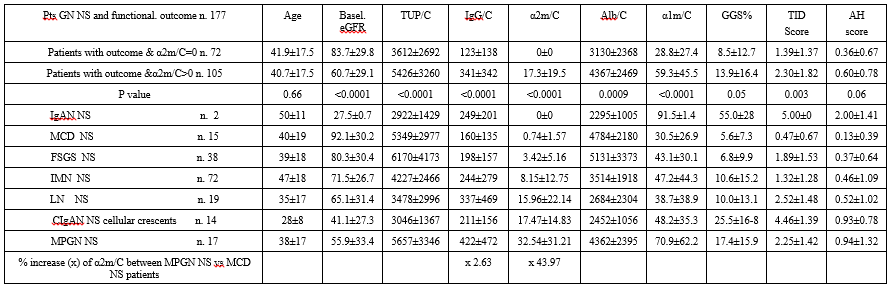
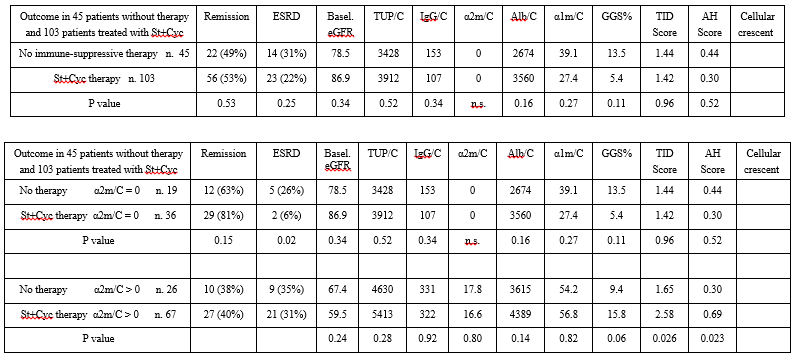
In 177 patients with GN and NS and functional outcome [follow up 86 ±72 months (2-331)] the mean α2m/C value was 10.2±17.2 (0-113.2). The α2m/C excretion increases from 0.74±1.57 in MCD to 32.54±31.21 in MPGN (x 43.9 times), while IgG/C increases from 160±135 to 422±472 (x 2.63 times). The α2m/C excretion increases progressively in different types of GN from MCD to FSGS, IMN, LN, CIgAN with cellular crescents and MPGN, respectively (Table 2). The high values of α2m/C are significantly associated with reduction of eGFR and increase of GGS%, TID score and AH score (Table 2). On the basis of these data showing very different α2m/C excretion in the various types of GN to evaluate how α2m/C excretion affects the functional outcome the patients were divided in two groups according to α2m/C value: α2m/C = 0 (n. 72) and α2m/C > 0 (n. 105); this classification is useful also to assess in every type of GN whether the outcome is different in patients with α2m/C = 0 and α2m/C > 0. The overall outcome in the 177 patients was: Remission: 98 patients [55%, follow up 107±79 months (12-331)]; PNS with long standing NRF: 13 patients [7%, follow up 77± 53 months (12-200)]; ESRD: 39 patients [(22%, follow up 41±32 months (2-119)]; eGFR reduction > 50% of baseline: 10 patients [6%; follow up 106±56 months (18-191)]; PNS with CRF n. 17 [10%; follow up 60±59 months (18-248)]. We decided to evaluate not only each type of outcome considered independently but also the combination of outcomes with similar prognostic significance: thus Remission was evaluated in combination with persistent NS with long lasting NRF, afterwards indicated as “Remission & persistent NRF”; ESRD and eGFR ≤ 50% were evaluated in combination with persistent NS with CRF characterized by progressive eGFR reduction and thus candidate to ESRD progression, afterwards indicated as “Progression & progression risk”. In patients with α2m/C=0 “Remission & PNS NRF” is: 100% in MCD and LN, 82%, 79%, 67% in FSGS, IMN, MPGN respectively (CIgAN with cellular crescents is not valuable as only one patient is α2m/C=0). In patients with α2m/C > 0 the combined outcome “Progression & progression risk” is 0%, 38%, 46%, 54%, 56%, 85% in MCD, LN, IMN, MPGN, FSGS, CIgAN with cellular crescents, respectively. This markedly different increase of α2m/C in comparison to the other urinary proteins in the different types of GN and NS suggest that the excretion of α2m/C may be dependent on a peculiar type of GFB damage that allows mainly the passage of the high MW protein α2m, while the passage of other proteins even with high MW such IgG is markedly lower. In my recent study evaluating a2m excretion in patients with crescentic IgAN with cellular crescents the data were in support of the hypothesis that α2m/C excretion could be a proteinuric marker of podocyte damage consequent to presence of cellular crescents. The observation that α2m excretion in patients with CIgAN with cellular crescents may be a marker of podocytes damage is also supported by the data of 19 patients with LN (n. 19): 11 (58%) with crescents and 8 (42%) without crescents with α2m/C excretion 22.43 and 9.87, respectively. Thus it may be suggested that α2m/C excretion could be a proteinuric marker of podocyte damage in GN with cellular crescents. In patients without crescents α2m excretion may be a marker of different degree of GFB damage in every type of GN: absent in MCD, progressively increasing in FSGS, IMN, MPGN and very severe in LN and CIgAN with cellular crescent and in MPGN characterized in few patients (12%) by crescents and by an immunofluorescent pattern of massive granular deposits of C3 and IgG along the capillary wall that may be associated with severe GFB damage. In conclusion the data of this study performed in a large cohort of patients homogeneous for selection (GN with NS) and with prolonged follow up, suggests that the very simple dosage of α2m/C show a high outcome prediction ranging from 0% progression in MCD with α2m/C=0 to 85% of “Progression & progression risk” in CIgAN with cellular crescents and α2m/C>0. Moreover this classification of patients shows the opportunity to evaluate the outcome according to treatment: no immune-suppressive treatment (n. 45) versus treatment with Steroids & Cyclophosphamide (n. 103). In patients with α2m/C = 0 remission is 63% in 45 untreated patients and 86% in 103 patients treated with steroids and cyclophosphamide; the difference between treated and untreated is lower in patients with α2m/C > 0: remission 46% in untreated and 51% in patients treated with St+Cyc suggesting that patients with α2m/C > 0 the responsiveness to immunosuppression is lower eventually dependent on significantly higher data of TID score and AH score.
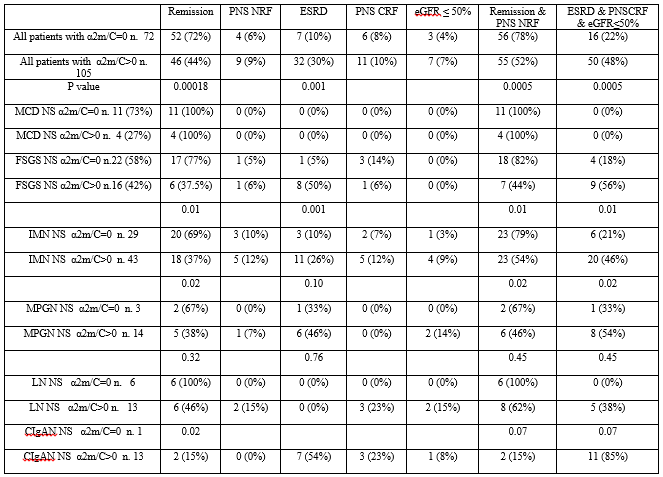
The evidence of a significant higher α2m/C excretion in Crescentic IgAN with NS and cellular crescents (CIgAN) in comparison to patients with IgAN PP and in Lupus Nephritis with crescents (10) in comparison with patients without crescents suggests that α2m/C excretion may by a marker of podocytes damage induced by crescents (11). The observation that α2m/C excretion progressively increases in other types of GN and NS without crescents such as MCD, FSGS, IMN, MPGN suggests that α2m/C excretion may be a marker of progressive damage of GFB whose degree may affect the functional outcome. This role may be supported by the observation of increase of favourable functional outcomes in patients with α2m/C = 0 in comparison with progressively unfavourable functional outcomes in patients with α2m/C > 0; in patients with α2m/C = 0 the combined outcome “Remission and NRF” is 100% in MCD and LN, and 82%, 79%, 67% in FSGS, IMN, MPGN respectively. In patients with α2m/C > 0 the combined outcome “Progression and progression risk” is 0%, 38%, 46%, 54%, 56%, 85% in MCD, LN, IMN, MPGN, FSGS, CIgAN with cellular crescents, respectively. These data may suggest that in patients without crescents α2m/C may be a marker of damage severity of GFB that according to value of α2m/C (= 0 or > 0) may be the responsible of increased percentage of favourable or unfavourable functional outcomes.
On the basis of the data of a large cohort of patients with different types of GN and NS, it is suggested that in all patients the level of α2m/C is a very simple marker available in all clinical practice laboratories and useful to predict functional outcomes and treatment responsiveness.
The study complies with the Declaration of Helsinki and local requirements for ethical approval. All patients gave their informed written consent. The article includes clinical research but no interventional studies. No financial support was received. The Authors have no ethical conflicts to disclose and no conflicts of interest to declare.
Research idea and study design: Claudio Bazzi
Data acquisition: Claudio Bazzi
Statistical analysis: Claudio Bazzi
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
