
Case Report | DOI: https://doi.org/10.31579/2693-2156/039
1 Professor of cardiac surgery, faculty of medicine, Cardiovascular Research Center of Mazandaran Heart Center, Mazandaran University of medical sciences, Sari, Iran
2 Cardiovascular Research Center of Mazandaran Heart Center, Mazandaran University of medical sciences, Sari, Iran
*Corresponding Author: Alireza Sanei Motlagh. Cardiovascular Research Center of Mazandaran Heart Center, Mazandaran University of medical sciences, Sari, Iran.
Citation: Shervin Ziabakhsh Tabary,Alireza Sanei Motlagh. (2022). Massive right ventricular and pulmonary artery emboli in-transit after cardiac surgery: consideration of non-surgical treatment, J.Thoracic Disease and Cardiothoracic Surgery, 3(2) DOI:10.31579/2693-2156/039
Copyright: © 2022 Alireza Sanei Motlagh. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 20 April 2022 | Accepted: 24 May 2022 | Published: 04 July 2022
Keywords: pulmonary embolism; in-transient emboli; deep vein thrombosis; cabg
Background:Pulmonary embolism (PE) is a complication of open-heart surgery that accounts for 0.6% of all cases and its mortality rate varies from 50% to 100%. Here, we describe a case of right ventricular and pulmonary artery emboli in-transit.
Case report: A 56-year-old female presented with complain of dyspnea and palpitation and history of recent coronary artery bypass graft (CABG) surgery. Edema of the right leg was noted. Trans-esophageal echocardiography (TEE) performed and revealed severe tricuspid regurgitation due to stucking clot in tricuspid valve. A large clot in right ventricle (RV) and right ventricle outflow tract (RVOT) with the size of 55 × 13mm was noted. There was also a clot with the size of 22 × 10mm in right pulmonary artery (RPA). Early in the ICU, patient received 10 units (18mg) of reteplase (IV) over 2 minutes and then 10 units was given with the rate of 1mg/hour after the first dose, with 30 minutes intervals. IV Heparin (18mg/Kg/h) was also co-administered with reteplase.There was no visible clot in RV and pulmonary artery in follow-up echocardiography. Patient transferred to CCU with stable hemodynamics and finally discharged with normal condition.
Discussion: Surgery is an alternative in patients with massive PE but our patient had a prior cardiac surgery which re-operation had a high risk for her. Due to massive in-transient emboli of right heart and PA in our patient, we decided to proceed the treatment with reteplase. The patient was monitored carefully for hemodynamics and coagulation parameters and she was discharged without any systemic complication.
Pulmonary embolism (PE) is referred to occlusion of pulmonary arteries with dislodged thrombus usually from deep veins of the lower limbs, pelvis, or arms. The first successful pulmonary embolectomy by means of cardiopulmonary bypass (CPB) was reported by Cooley and colleagues in l961 [1]. PE is a life-threatening complication of post-operation venous thromboembolism (VTE) which accounts for 0.6
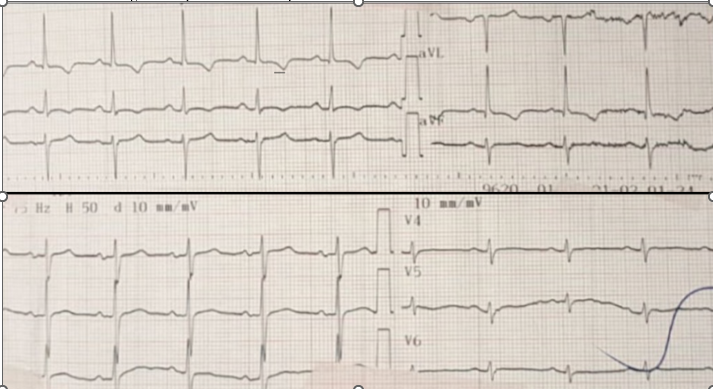
A 56-year-old female presented to the heart center with complain of dyspnea and palpitation. Past medical history of recent coronary artery bypass graft (CABG) surgery (just a week ago), hypothyroidism, hypertension, dyslipidemia, and kidney stone were noted for her. She was medically managed with levothyroxine, propranolol, aspirin, and rosuvastatin. She had no history of diabetes mellitus. The patient had tachypnea and diaphoresis at the arrival. On physical examination, edema of the right leg was noted. The finding of skin, musculoskeletal, and neurological examinations were normal. Pulse rate was 110 beats/min, blood pressure was 110/60 mmHg, respiratory rate was 26 breaths/min, and the patient's axillary temperature was 37.1oc. The patient had tachypnea and tachycardia. T-wave inversion in leads I, II, aVL, and upright T wave in lead aVR were noted on ECG [figure 1].
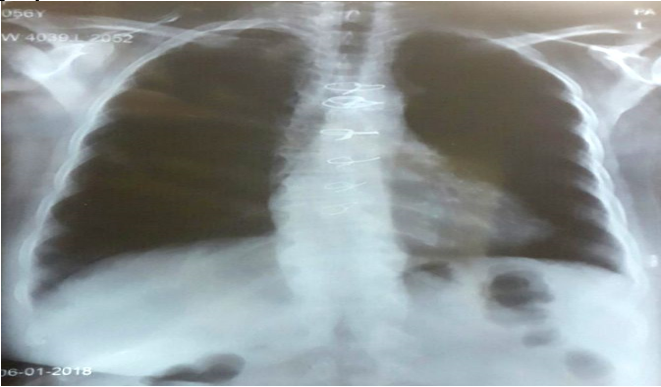
Chest x-ray findings indicated a mild cardiomegaly, blunted right pleural border, and patchy nodularity in right paracardiac border with the decreased filling in right lung [figure 2].
With the suspicion of a clot in the heart, trans-esophageal echocardiography (TEE) performed and revealed an ejection fraction of 55%, severe tricuspid regurgitation due to stucking clot in tricuspid valve, very large clot in right atrium (RA), right ventricle (RV), and right ventricle outflow tract (RVOT) with the size of 55 × 13mm. There was also a clot with the size of 22 × 10mm in right pulmonary artery (RPA) [figure 3].

Also, a mild RV enlargement and pulmonary artery pressure (PAP) of 55mmHg was noted. There wasn't any flow in popliteal veins (in neither of two directions) on color-Doppler ultrasonography of lower limbs. These evidences support the deep vein thrombosis (DVT) of both legs. All the external iliac arteries, femoral arteries (superficial and deep), popliteal arteries, tibialis arteries (anterior and posterior), and dorsalis pedis arteries were patent based on the report of color-Doppler and gray-scale ultrasonography. The patient was referred to intensive care unit (ICU). Nasogastric tube was inserted for parenteral nutrition. Also, triple-lumen central venous catheterization (CVC) of right subclavian vein performed by local anesthesia. Initial laboratory study showed a plasma pH of 7.13, platelet of 50 × 109/L, and hemoglobin of 8.3g/dL. Early in the ICU admission, patient received 10 units (18mg) of reteplase (IV) over 2 minutes and then 10 units were given with the rate of 1mg/hour after the first dose, with 30 minutes intervals. Heparin was also administered with the infusion rate of 18mg/Kg/h. At 3:00 a.m. the next day, bradycardia was developed which followed by cardiopulmonary arrest. Cardiopulmonary resuscitation (CPR) performed by chest compression, infusion of dobutamine and high dose epinephrine. Endotracheal intubation was accomplished during CPR. After that, the normal sinus rhythm was established but the patient had anuria. Laboratory results reported a high serum creatinine (2.8 mg/dL) and blood urea nitrogen (BUN) of 45 mg/dL which indicated acute renal failure. Thrombocytopenia with platelet count of 20 × 109/L, potassium level of 3.3mmol/L, partial thromboplastin time (PTT) of 41, and international normalized ratio (INR) of 1.70 was also noted on laboratory studies. Heparin was discontinued due to decrease in platelet count. Medical treatment continued with rivaroxaban (xalerban) 15mg po twice daily, aspirin 80mg po per day, and propranolol 10mg po twice daily. Potassium chloride was also administered due to hypokalemia. 3 units of packed red cells (p.c) and 3 units of platelets transfused during this course.
Patient's urine output was improved on the next days. According to the results of bed-side TEE, there was no visible clot in RA, RV, PA, and proximal of its right and left branches on the second day of ICU admission. The patient extubated on 5th day in the ICU, and blood oxygen saturation was acceptable. Patient's length of stay at the ICU was ten days. Laboratory results of the last day reported a hemoglobin value of 10.3g/dL, platelet count of 215 × 109/L, potassium level of 4.8mEq/L, BUN of 10 mg/dL, and creatinine of 0.94mg/dL. Coagulation study reported a PTT of 33 and INR value of 1.66. ECG showed a normal sinus rhythm but T-wave inversion on lead 1 was still noted. The patient transferred to the cardiac care unit (CCU) with stable hemodynamics. Total length of stay in the CCU was 7 days. It should be noted that despite the massive emboli in the right heart and pulmonary artery, redo cardiac surgery or inferior vena cava (IVC) filter insertion were not performed. The venous thromboembolism was managed by reteplase. Neurological examinations were normal. Patient was discharged with normal vital signs and referred to interventional cardiologist for further workup
The main presenting symptoms of pulmonary embolism (PE) are tachypnea, dyspnea, tachycardia, diaphoresis, and loss of consciousness [1]. Considering the history of cardiac surgery in our patient and hospitalization for some days, color-Doppler ultrasonography and TEE performed to determine whether an embolus is responsible for her sign and symptoms. According to 2014 ESC Guidelines on the diagnosis and management of acute pulmonary embolism, treatment of acute phase of PE is supported by hemodynamics and respiratory monitoring, administration of inotropes to improve RV function, anticoagulant agents, thrombolytic agents, percutaneous catheter-directed treatment for patients with absolute contraindications to thrombolysis, supra- or infrarenal placement of IVC filter, and surgical embolectomy [9]. Reports of surgical embolectomy indicate that early mortality rate has ranged from 4.4% to 21% [1]. Post-surgical complications included stroke, acute renal failure, lower respiratory tract infection, right ventricular dysfunction, wound infection, and sepsis [10-12]. Despite the risk of bleeding, thrombolysis can improve right-ventricular wall motion, and pulmonary perfusion which results in lower rates of death and recurrent PE [13]. In a randomized controlled trial (RCT) of Meyer et al. with 506 cases of intervention, the mortality rate related to administration of fibrinolytic agent tenecteplase was reported 1.2% compared with 1.8 % in control group (p-value= 0.42). Fibrinolysis was associated with major extracranial hemorrhage by 6.3% and hemorrhagic stroke by 2.0%, but the rate of recurrent PE was lower (0.2 in tenecteplase group vs. 1.0 in placebo group, P<0>
Due to massive in-transient emboli of right heart and PA in our patient, we decided to proceed the treatment with reteplase. Heparin was co-administered but by the fall in platelet count, it was discontinued and anticoagulant therapy was continued with rivaroxaban. Routine follow-ups are indicated in patients who were bedridden for long times after major surgery due to the risk for venous thromboembolism. Surgery is an alternative in patients with massive PE but our patient had a prior cardiac surgery which re-operation had a high risk for her. The problem with treatment by thrombolytic agents is the incidence of intracranial hemorrhage which can result in functional complications or death. Our patient was monitored carefully for hemodynamics and coagulation parameters and she was discharged without any systemic complication.
The authors declare that they have no conflicts of interests.
Written informed consent was not available because of the replacement of residence but oral agreement from the patient was obtained.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
