
Case Report | DOI: https://doi.org/10.31579/2640-1053/115
1 Jinhua Municipal Central Hospital, Jinhua, Zhejiang, China.
2 Bone Marrow Transplantation Center, Department of Hematology, The First Affiliated Hospital, School of Medicine, Zhejiang University, Hangzhou, China
*Corresponding Author: Cancan Lu, Jinhua Municipal Central Hospital, Jinhua, Zhejiang, China.
Citation: Cancan Lu, Yishan Ye, Jimin Shi, Yamin Tan. (2022). Massive digestive tract bleeding caused by EBV-triggered Hemophagocytic Lymphohistiocytosis and digestive tract vascular malformation. Cancer Research and Cellular Therapeutics. 6(3); Doi:10.31579/2640-1053/115
Copyright: © 2022 Cancan Lu, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 23 March 2022 | Accepted: 30 May 2022 | Published: 10 June 2022
Keywords: hemophagocytic lymphohistiocytosis(hlh; severe; eb virus infection; digestive tract vascular malformation; gastrointestinal bleeding
We introduced a patient with fetal EBV-triggered who finally developed multidrug-resistant septicemia, perianal abscess, massive alimentary tract bleeding due to gastrointestinal vascular malformation, and acute respiratory distress syndrome. His EB virus maintained chronically active under multiple drug treatments. Interestingly, continuous EB virus infection and a probable idiopathic gastrointestinal vascular malformation might be the cause of the severe digestive tract bleeding.
Hematopoietic lymphocytic tissue disease (HLH), also known as hematopoietic cell syndrome (HPS), is a series of clinical syndromes caused by genetic or acquired immunodeficiency [1]. The most common clinical features of HLH are fever, enlargement of the liver, spleen, lymph nodes, progressive pancytopenia, abnormal liver function, blood coagulation dysfunction, etc. It may also be accompanied by an abnormality in central nervous system. HLH could be either idiopathic or secondary, with idiopathic mainly happened in children or teenagers and secondary in adults. It is mainly caused by infections (bacteria, fungi, Epstein -Barr virus), autoimmune diseases or tumors [2]. Chronic active Epstein-Barr virus infection (CAEBV) is one of Epstein-Barr virus (EBV) -positive T or NK lymphoproliferative diseases. Epstein-Barr virus-associated hemophagocytic lymphohistiocytosis s (EBV-HLH) is a blood cell lymphocytic histiocytosis caused by the activation of EB virus infection, which is more severe than other HLH types, and has a high death rate and a poor prognosis [3].
A 25-year-old, previously healthy young man from China showed fever and discomfort in the nasopharynx in July 2019. Nasopharyngoscopy showed bilateral nasal mucosal erosion. The Blood routine: WBC 3.0×10 ^ 9 / L, HGB 113 g / L, PLT 87×10 ^ 9 / L, CRP13.53mg / L,Bone marrow morphology showed a small population of abnormal lymphocytes with immature morphology and abnormal nuclear, monocytes and monocytes were occasionally seen. A second bone marrow morphology showed the proportion of myeloid primordial cells was not high and no obvious abnormalities were seen. Immunotyping showed no obvious abnormalities in the phenotype. Bone marrow biopsy showed no obvious abnormalities of lymphocytes. Meanwhile the blood EB virus DNA was 32657.0 copies / ml. The tonsillary biopsy showed reactive lymphocyte hyperplasia with EBV infection. A ferritin level > 500μg/L, hepatosplenomegaly, lymphadenopathy, hypofibrinogenemia, according to all these he was diagnosised of “EB virus infection, hematopoietic syndrome”.
We initiated anti-inflammatory treatment with methylprednisolone, anti-infection with meropenem, and symptomatic supportive treatment such as sodium phosphonate antiviral and infusion of plasma. The patient still had daily high fever, progressive enlargement of liver and spleen, reexamination of EB virus DNA showed 5.9×10 ^ 3 copies /ml, sCD25: 22050pg /ml. Because the disease is out of control, the fever persists, we added ruxolitinib in 2019-08-12, and the maximum dose was increased to 20mg twice daily. 2019-08-27 PET-CT showed a. The left lower inferior parietal mucosa is thickened, and FDG metabolism is significantly increased; b. hepatosplenomegaly, FDG metabolism is unevenly increased; c. the whole-body bone marrow FDG metabolism is increased (the 7th rib on the right was serious), the rest were not significantly abnormal. Because of the poor effect of early treatment, we decided to use first-line chemotherapy for hemophagocytic syndrome. From 2019-08-28, Treatment was initiated based on the HLH-2004 protocol with DXM 10mg/m2 qd for 2 weeks, VP-16 100mg/m2, biw×2 weeks, and gradually reduced, 225 mg of cyclosporine twice daily. Because this person is young, in order to figure out the cause of hemophagocytic and distinguish between primary and secondary, we did a genetic test and a heterozygous mutation (NM_001099856: exon5: c.G753C: p.Q251H) was detected in the IKBKG gene, as well as the same mutation in his mother. The level of EB DNA is still high and the fever persists after chemotherapy, we decided to use the second-line regimen.
Since 12th September in 2019, we give him chemotherapy as Hyper-CVAD part A (CTX 600mg q12h d1-3; VDS 4mg d4, d11; Ridox 60mg d4; DXM 40mg d1-d4, d11-14). The liver and spleen contracted slightly, but the EB virus level was still high. 3 days after finish of chemotherapy, blood culture showed positive for Pseudomonas aeruginosa (multidrug resistance), and perianal abscess.
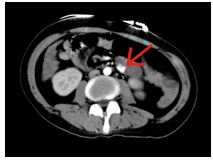
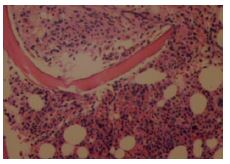
12th October in 2019, the results of routine blood test showed that WBC 5.3×10 ^ 9 / L, RBC 1.65×10 ^ 12/L, HGB 48g/L, PLT 51×10 ^ 9/L. And since 12th October he Began to relieve a large amount of black stools, enhanced abdomen CT examination revealed nodular enhanced foci in the upper cavity of the jejunum, considering as vascular malformations (Figure 1), partial resection of the small intestine was operated on 13th October, and pathology suggested mild inflammation of the small intestinal mucosa. On 21th October, a new bone marrow morphology showed one type of abnormal lymphocytes and hemophagocytic, considering the possibility of lymphoma. Bone marrow biopsy showed a large number of EBER-positive T lymphocyte infiltration with hemophagocytic, considering as a T-lymphocyte proliferative disease related to severe EBV infection (Figure 2). Immunohistochemistry showed CD3 +, TIA +, EBER +, ≥100 / HPF, CD20-, CD30 individual +, CD56-, and hemophagocytic can be seen. Subsequently, the patient suffered from acute respiratory failure, septic shock, and acute renal insufficiency, and his Parents decided to give up treatment, he died shortly after leaving the hospital on 31th October.
We report a case of HLH that turn into a worse rapidly with bleeding from a gastrointestinal malformation of the digestive tract. Kumakura et al [4] proposed a disease called autoimmune-associated hemophagocytic syndrome (AAHS) in 1997. The pathogenesis of AAHS can be explained by autoantibody-mediated, immune complex-mediated, or cytokine-mediated mechanisms: First, autoantibodies may react with blood cells, and thus pass-through stimulated tissue cells through Fc receptors (mainly in the bone marrow). Second, blood cells sensitized by the immune complex may be engulfed by tissue cells through complement-receptor interactions. Finally, uncontrolled production of inflammatory cytokines may activate tissue cells [5-7]. HLH pathophysiology is based on the cytotoxic function of natural killer lymphocytes (NK cells) and cytotoxic T lymphocytes (CTL), hyperproliferation and subsequent absence of cytokine storms [8].
Organ infiltration with high cytokine levels is associated with signs and symptoms of HLH. Long-term fever is caused by high levels of interleukin 1 (IL1), interleukin 6 (IL6), and tumor necrosis factor alpha (TNFα). Hemocytosis is due to high concentrations of TNFαand phagocytic cells. Macrophages infiltrate the bone marrow infiltration of hematopoietic components (red blood cells, white blood cells, platelets, precursors and cell debris [9-14]. Fibrosis increased by increased plasminogen activators expressed by activated macrophages, and serum plasmin levels increased, which led to abnormal HLH coagulation function caused by macrophage tissue infiltration, accompanied by liver dysfunction. Activated macrophages emit high levels of ferritin, and activated lymphocytes produce high concentrations of the soluble form of the IL-2 receptor (sCD25). HLH diagnostic guidelines by Henter et al released in 1991: (1) temperature > 38.5 ℃, lasting> 7 days), (2) splenomegaly, (3) cytopenia involving two of three cell lineages in the peripheral blood, (4) hypertriglyceridemia and / or a decrease in fibrinogen (<1> 2400 U/mL (sCD25≥6400pg / ml) [16]. Diagnosis of secondary HLH necessitates the fulfillment of five of the above eight criteria. Since not all of diagnostic criteria occur simultaneously, so diagnosis is often very difficult.
During the disease process, CAEBV can lead to two deadly diseases: hemophilic lymphocytic tissue disease and chemotherapy-resistant lymphoma. Treatment should be taken before the onset of these two diseases. Currently, allo-HSCT is the only effective treatment strategy to eradicate EBV-infected T cells or NK cells. Even if when the exact cause of the patient remains unknown, since the duration from the onset of disease to transplantation can be a factor that affects HLH progression and death, it is necessary to start looking for donors when being diagnosis of HLH. Transplantation should be used as soon as possible after the patient’s medication has been released clinically. Finally, non-steroidal anti-inflammatory drugs (FANS) such as indomethacin, naproxen and ibuprofen may work, but we are still lack of the previous treatment experience for patients with HLH.
This patient's gene mutation detection analysis report shows that a heterozygous mutation (NM_001099856: exon5: c.G753C: p.Q251H) was detected in the IKBKG gene, and this mutation was Inherited from his mother. IKBKG is associated with immunodeficiency type 33 and simple immunodeficiency, the main symptom of this type of disease are decreased immune system function, repeated infections, and abnormal growth of ectodermal tissue. In regard to this patient, the immune deficiency caused by this gene may be related to the CAEBV, but unfortunately we do not have data on his immune function before the onset of the disease.
Chronic EBV infection is very rare with gastrointestinal bleeding. As far as we know, the number of previously reported cases is not large, but most of them have a poor prognosis, whether it is patients with normal immune function or immune deficiency. Xu L et al have reported a case of chronic active Epstein-Barr virus infection in the small intestine of a 5-year-old Chinese boy. The patient later showed gastrointestinal bleeding and be diagnosed of an internal carotid aneurysm on the right. Hemorrhage improved and the right internal carotid aneurysm disappeared at a later follow-up [17]. Wang Y et al reported a case of middle-aged woman who went to the hospital for fever, blood in the stool, and after a partial bowel resection, the pathology confirmed that the disease was caused by EB virus infection, and the patient died shortly [18]. Denicola RP et al reported a case of acute gastrointestinal bleeding caused by EB virus-infected viral colitis in middle-aged and elderly women, who recovered and was discharged after active treatment [19]. Xu N et al Reported 21 adult CAEBV patients, 2 cases of gastrointestinal bleeding, one of which had underwent colectomy and was pathologically confirmed as colitis caused by CAEBV [20]. The CAEBV of this patient is clear, but the intestinal pathology did not indicate intestinal EBV infiltration, so we consider that the gastrointestinal bleeding is caused by congenital vascular malformation and severe infection.
We hypothesized that if the patient could obtain earlier treatment with HLH-04 or DEP-based combination therapy, there would be more chances to operate an allogeneic hematopoietic stem cell transplantation. But Arai et al reported that, OS 100
Author contributions: Cancan Lu wrote the manuscript.
Yishan Ye revised the manuscript, approved the final version, and is the article guarantor. Jimin Shi and Yamin Tan analyzed and interpreted the data.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
