
Case Report | DOI: https://doi.org/10.31579/2690-1897/171
1 Department of Maxillofacial Surgery Hospital of Specialities Rabat, Morocco.
2 Department of Otolaryngology and neck surgery Hospital of Specialities Rabat, Morocco
3 Faculty of Medicine and Pharmacy of Rabat. Mohammed V University in Rabat, Rabat, Morocco.
*Corresponding Author: Rajaa El Azzouzi, Department of Maxillofacial Surgery Hospital of Specialities Rabat, Morocco.
Citation: Rajaa El azzouzi, Othmane Bouanani, Babah Hassene ZA, Kawtar Ayyad, Malik Boulaadas, et al, (2024), Mandibular Osteonecrosis after Biphosphanates Therapy: An Atypical Clinical Presentation: Case Report and literature Review, J, Surgical Case Reports and Images 7(1); DOI:10.31579/2690-1897/171
Copyright: © 2024, Rajaa El Azzouzi. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 04 December 2023 | Accepted: 21 December 2023 | Published: 09 January 2024
Keywords: AAOMS; biphosphanates; case report; osteonecrosis
Introduction:
Osteonecrosis is a complication of long-term treatment with biphosphanates (BP) occurring mainly in patients treated for bone metastases or multiple myeloma. However, a few rare cases have been observed during per osteoporosis treatment. The mandible is the preferential location of this disease.
Presentation of the cases:
We report the case of a 56 year old patient treated for osteoporosis for 6 years with oral biphosphanates who consulted for cutaneous-oral fistulas of the chin region. The imagery showed osteo-condensing and fistulated foci related to mandibular osteonecrosis. After discontinuation of biphosphanates, the patient was put on long-term antibiotic therapy, corticosteroid therapy and received hyperbaric oxygen therapy. The evolution after 5 months was favorable.
Discussion:
During mastication, the maxillae are subjected to regular stress that stimulates remodeling activity leading to greater incorporation of biphosphanates, promoting bone necrosis. The clinical presentation of the disease can range from a poorly healing socket after tooth extraction to massive necrosis of the jaw. Faced with this rather rare but disabling and difficult to treat condition, it is important to identify patients at risk and apply preventive measures.
Conclusion:
Given the lack of objective data regarding the precise incidence, pathogenesis, and treatment of this complication, there is an urgent need for controlled studies to improve the management of these patients and ensure the best possible quality of life.
Osteonecrosis is a complication of long-term treatment with biphosphanates (BP) occurring mainly in patients treated for bone metastases or multiple myeloma. However, a few rare cases have been observed during per osteoporosis treatment. Given the particularity of our study which reports the case of a severe advanced form in a patient followed for osteoporosis under treatment with oral biphosphanates.
We report the case of a 56-year-old female patient followed for osteoporosis for 6 years on oral biphosphanates (Alendronate), who consulted for pain in front of the mandible and dental mobility associated with dental avulsions for 1 year, with an evolution marked by the appearance of two superinfected skin fistulas in the mental and submental regions; stage 3 according to the classification proposed by the American Association of Oral and Maxillofacial Surgeons (AAOMS) (Table 1), (Figure 1).

Figure 1: Image of the patient showing cutaneous-oral fistulas
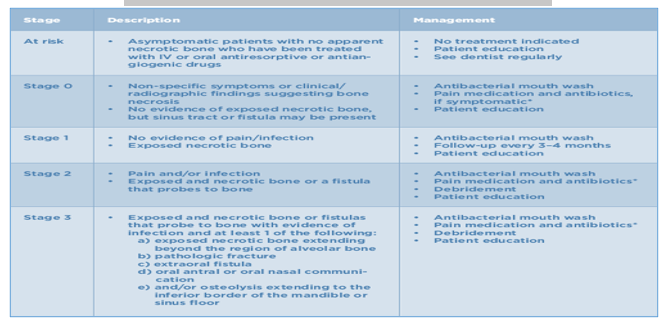
Table 1 : 2014 AAOMS Classification and Proposed Treatment Strategies
An extension workup was performed including an orthopantomogram, and a Denta-Scan showed osteo-condensing and fistulized foci related to mandibular osteonecrosis. (Figure 2)

Figure 2: Scannographic images showing mandibular osteonecrosis with foci of bone lysis
After discontinuation of biphosphanates, the patient was put on long-term antibiotic therapy, corticosteroid therapy, mouthwash with chlorhexidine and hyperbaric oxygen therapy. The evolution after 5 months was favorable.
BPs are synthetic analogues of pyrophosphates with a strong affinity for hydroxyapatite crystals.
A distinction is therefore made between first-generation bisphosphonates containing no nitrogen (etidronate, clodronate), first-generation amine derivatives (alendronate, pamidronate) and new-generation amine derivatives (zoledronic acid, risedronate) where the nitrogen is located on a heterocycle [1].
They are widely used in the symptomatic treatment of bone metastases and pathologies characterized by a deregulation of bone turnover, such as osteoporosis and Paget's disease.
Resorbed bisphosphonates bind to bone at sites of active metabolism, such as the maxillomandibular region, which is under constant pressure and trauma, where they reach their therapeutic concentration [2,3]. These molecules inhibit the dissolution of hydroxyapatite crystals and induce a decrease in bone remodeling and turnover [4,5]. During the bone resorption phase, PBs are internalized by osteoclasts and lead to their dysfunction.
Maxillomandibular osteonecrosis (MMO) is characterized by an area of exposed bone in the maxillofacial region that does not heal within 8 weeks of appropriate care, in patients who have received or are receiving PB and have not been treated with maxillofacial radiotherapy [6].
The most important risk factors are the dose and duration of exposure, especially if it is longer than 2 years, and the type of BP. The injectable form and the amino derivatives have a higher toxicity. The majority of osteonecrosis is therefore described on Zoledronate, reaching more than 10% of treated patients. Next, we find patients treated with Pamidronate followed by Zoledronate, then Pamidronate and lastly Alendronate. One in ten necrosis would be due to oral bisphosphonate for osteoporosis [7-9].
The location is mandibular in 2/3 of cases. A previous extraction is demonstrated in 60 to 77% of cases1. The average time of onset of bone necrosis after dental treatment is 6.6 months. The symptomatology is not very specific, ranging from a poorly healing socket after dental extraction to massive necrosis of the jaw [10]. Complementary examinations performed to assess the severity, extension and follow-up are primarily orthopantomogram and CT scan or Denta-Scan.
The treatment of these bone necroses is unsatisfactory. Local debridement maneuvers result in a more significant denudation of the treated area. In addition, since the entire bone is affected, it is difficult to resect the affected area macroscopically with healthy margins, as is the case in osteoradionecrosis resections. Cover flaps lead to significant fistulas. Hyperbaric oxygen therapy does not improve the situation. We are therefore limited to the use of chlorhexidine-based mouthwashes, antibiotics in case of superinfection and painkillers on demand. The removal of bone spurs that injure the surrounding tissues is performed for the patient's comfort. Discontinuation of bisphosphonates is without effect since their bone half-life is estimated to be more than 10 years [9].
Given the lack of objective data regarding the precise incidence, pathogenesis, and treatment of this complication, more controlled studies are needed to improve the management of these patients and ensure the best possible quality of life.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
