
Case Report | DOI: https://doi.org/10.31579/2693-4779/189
Public Health Consultant, Bengaluru, India.
*Corresponding Author: Suresh Kishanrao, Public Health Consultant, Bengaluru, India.
Citation: Suresh Kishanrao (2024), Managing chronic constipation & IMPACTED STOOL IN INFANTs and young children in smaller settings, Clinical Research and Clinical Trials, 9(4); DOI:10.31579/2693-4779/189
Copyright: © 2024, Suresh Kishanrao. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 02 February 2024 | Accepted: 23 February 2024 | Published: 15 March 2024
Keywords: infant; young child; toddlers; constipation; chronic constipation; impacted stool; laxatives; stool soothers; enema; digital evacuation and dilatation; general practitioners or family physicians; paediatricians and paediatric gastroenterologists
A normal stool in the infants and children is soft, easy to pass, and its colour may vary from green, yellowish to brown. The rectum is usually empty until it’s time for bowel movement. If the stool remains in large bowl for long it becomes hard due to absorption of water and results in hard stool and makes it difficult for these young children for bowel movement ending in constipation. Defecating less than three time a week, or a complaint of a painful bottom, a bloated tummy, passing large hard stools, excessive straining while pooing, loss of appetite, and irritability are some of the common signs of constipation. Faecal impaction is a condition when the constipation becomes so severe that children are unable to pass any formed stool. All the poo in their bottom clumps together to form a large mass, making it difficult to expel. Daily addition of poo in the large bowel, leads to the children passing of small bits of stools, and lots of gas with bad odour.
Usually, a faecal impaction can be identified by palpating a hard mass of stool in left iliac fossa on physical examination or finding a large amount of stool in a dilated rectum on rectal examination or finding excessive stool in the colon on an abdominal radiograph.
As there is no uniform definition of childhood constipation reported prevalence rates range between 1% and 30%. It is the principal complaint in 3-5% of all visits to outpatient clinics and as many as 35% of all visits to Paediatric gastroenterologists. It is important to differentiate these two conditions as the management changes. When there is an evidence of a faecal impaction, therapy should be directed at evacuating the colon. Apart from stool softeners and laxatives, digital evacuation comes to rescue in cases which do not respond to conservative management.
This article is based on 2 cases managed by the author, one in January 2024, and another in 1990 both resolved by digital evacuation of impacted stool and dilatation of the anal sphincters apart from managing such 1-2 cases annually out of about 100 cases of chronic constipation each year.
Materials and Methods:
Details of 2 cases managed by the author, one in January 2024, and another in 1990 both resolved by digital evacuation of impacted stool and dilatation of the anal sphincters at home apart from managing such 1-2 cases annually in the clinics. Global Literature review on the subject and practices adds to the personal experience.
A normal stool in the infants and young children is soft, easy to pass, and its colour may vary from green, yellowish to brown. The last portion of the large bowel called rectum is usually empty until it’s time for bowel movement. If the stool remains for long in large bowel, it becomes hard due to absorption of water and results in hard stool and makes it difficult for the infants and children for bowel movement ending in constipation. The young children become frightened an experience of straining and pain and they start holding the poo worsening the situation. Pooing less than three time a week or more than 3 times a day, or a complaint of a painful bottom, a bloated tummy, passing large hard stools, excessive straining while pooing, loss of appetite, and irritability are some of the common signs of constipation [1].
A child is said to have faecal impaction when the constipation becomes so severe that they are unable to pass any formed poo. All the poo in their bottom clumps together to form a large mass, which the child is unable to pass. More and more poo will be added daily in the large bowel, but the infant can’t expel the same. This leads to the children passing of small bits of stools, and lots of gas with bad odour in addition to signs of constipation listed above. Both constipation and Impacted stool causes stretching of the bowel, needing more time to return to normal. The infants with impacted poo may pass small bits of poo or loose motions several times a day. If the constipation lasts for more than 4-weeks, it is called chronic constipation. It is difficult to differentiate between constipation and Impacted stool. Constipated Infants and Children pass infrequent large and hard formed stools, whereas a child with Impacted stool is unable to pass formed stools altogether, instead pass loose, or mushy, semi-solid poo or small bits of hard stools. It is important to differentiate these two conditions as the management changes [1].
Chronic constipation is common among children worldwide. It is common at three times in an infant's and child's life especially infants and young toddlers up to 2 years: i) after starting cereal and puréed foods as a process of weaning, ii) during toilet training, and iii) after starting school [2]. Constipation includes functional constipation (FC) and organic constipation (OC). A child with constipation may have bowel movements less frequently than normal, or their bowel movements may be hard, large-Caliber, or difficult and painful to pass. As most children with constipation do not have an identifiable underlying medical problem, early recognition of the causes and its subsequent complications is important [1,2,3]. Faecal impaction is a solid stool that is "stuck" in the rectum, typically because of chronic constipation [1,4]
As there is no uniform definition of childhood constipation reported prevalence rates range between 1% and 30%. It is the principal complaint in 3-5% of all visits to outpatient clinics and as many as 35% of all visits to Paediatric gastroenterologists. Nearly 15% of the infants and children coming to gastroenterology complaints, seek care for constipation. Generally regarded as less significant problem but chronic constipation is more troublesome to child as well as parents. Functional constipation is more common (prevalence in childhood = 0.7% to 29.6%) among constipation types. Organic constipation is more common in young children with a low body weight, stunted growth, mucus in the stool, and associated diseases, needing to be assessed for underlying organic causes of constipation.
A faecal impaction can be identified by palpating a hard mass of stool on physical examination or finding a large amount of stool in a dilated rectum on rectal examination or finding excessive stool in the colon on an abdominal radiograph. The differential diagnosis of childhood constipation includes Hirschsprung disease, spinal or neuromuscular abnormalities like spinal muscular atrophy, tethered cord, Currarino triad, cerebral palsy. When there is evidence of a faecal impaction, initial therapy should be directed at evacuating the colon.
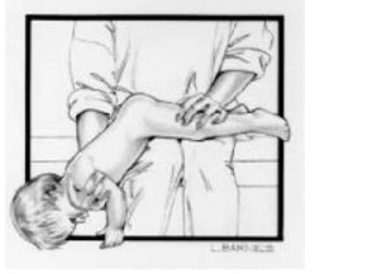
Therapy for constipation must begin with fruits like prunes, plums, pears, peaches which help soften the baby's stool. In terms of medication theoretically one can begin with use of oral cathartics such as polyethylene glycol, sodium phosphate, magnesium citrate, or a balanced electrolyte solution with polyethylene glycol. A cathartic is a substance that accelerates defecation by softening faeces. Alternately stimulant laxatives like bisacodyl, senna, danthron, and ricinoleic acid, which enhance motility through either nonspecific local mucosal irritation or a more selective action on the intramural nerve plexus of intestinal smooth muscle can be tried. It is possible for a substance to be both a laxative and a cathartic. Psyllium seed husks increase the bulk of the faeces. Practically, making an infant or a young child to ingest large amounts of oral cathartics to evacuate their colon is difficult; therefore, Pedia-Lax Laxative, Liquid Glycerin suppository or Polyethylene Glycol (PEG 3350) syrup are the recommended laxatives to be used in infants and children in India, as they oral syrups and suppositories are designed for kids and are a safe approach. Very few patients (1%) with severe constipation do not respond to conservative medical therapy and require digital evacuation or even surgery [1]. Digital disimpaction is the use of fingers to manually remove stool from the rectum, done by the parents of the infants or a medical professional. For this procedure, a single finger of a gloved hand is lubricated and inserted into the rectum. The stool is gently broken up and removed in pieces until the rectum is cleared.
This article is based on 2 cases managed by the author, one in 1990 and another in January 2024, both resolved by digital evacuation of impacted stool on 3-5 occasions. A discussion of surgical interventions like Sphincterotomy, in which the anal sphincter muscle is cut to open the anal canal, is beyond the scope of this article.
Case 1. Pawan: Pawan my youngest son aged about 2 years then, when I moved from Bengaluru to Delhi, had a problem of chronic constipation in early 1990. He was diagnosed as a case of Noonan’s Syndrome (NS) after genetic evaluation in AIIMs New Delhi. About 18% of NS cases have gastrointestinal malformations or malfunctioning leading to chronic constipation coupled with pelvic muscles weakness. After trying multiple stool softeners and oral cathartics and a thorough check-up showing no structural problems, I tried digital evacuation at home, every 3-4 days for about half a dozen times. We had increased fibre in his diet by increasing fruits and green leafy vegetables and sugar consumption. After about 3 weeks of digital evacuation twice a week, he started passing stool himself on alternate days. Thereafter, I made him to sit on toilet for 10-15 minutes after breakfast each day. I and my wife tried toilet training cultivating a regular habit of daily bowel movement after breakfast and lunch keeping him engaged for 10-15 minutes for about 3 months. We provided the child foot support (a stool under his feet), high enough such that his knees were slightly above his hips as he was using an adult-sized toilet. Over a total of 6 months, he developed a regular bowel movement practice with no laxatives.
Case 2. Suhas 2024: Manisha a young first-time mother brought her infant Suhas of 7.5 months on 18 January 2024, with the complaints of constipation for 2 months, co-terminus with weaning by introducing solid foods. Current constipation episode was 4 days old. The infant would not pass stools for 4-5 days in a row. The family physician and a paediatrician had prescribed iron and multivitamin drops for last 3 months, which I stopped with immediate effect. They had also prescribed laxative pessaries, which facilitated bowel movement 2 times a week. On physical examination the child was calm, active. Abdominal palpation found stool mass left lower iliac fossa (in rectum & colon). I advised her to give the child the fruits Banana, Pears. After 3 days as there was no bowel movement, I advised the mother to try digital evacuation. After getting plastic gloves I demonstrated on 22nd evening how to do digital evacuation. On 23 mornings, as I was on travel Manisha called to report the success of digital evacuation.
Steps to followed /trained to Perform Digital Disimpaction:
A digital disimpaction is usually done daily or every other day, depending on the individual. The first step is to gather needed supplies, like Soap, washcloth, and towel & a water source, Lubricant, a plastic bag to throw waste in, toilet seat, commode, or shower chair and under pads. Sterile gloves are key to personal hygiene and avoiding infection and should be discarded after use.
iv) Faecal Matter Removal: Gently remove any faecal matter, repeating the process until there's no more stool.
Disimpaction was done successfully by the mother, and child passed stool on its’ own for next 3 days. The infant was advised to continue high fiber diet, and maintenance dose of polyethylene glycol PEG. After 1 week of disimpaction, the infant had again constipation for 4 days till 30 January 2024. As the parents were on travel, they are advised to continue PEG suppository and try digital evacuation twice a week on return. The child is being followed-up and hopefully will resolve in next 2-3 months after 6-8 attempts of digital dilatation & (DDE) evacuations. DDE stretches the anal sphincter muscles, helping easy evacuation of stools.
The "normal" amount of time between bowel movements and in infants or children depends upon their age and what they eat or drink. During the first week of life, most Indian infants pass approximately four soft or liquid bowel movements per day. Infants on formula feeds generally have fewer bowel movements than those who are exclusively breastfed. During the first three months of life, most breastfed infants have approximately three soft bowel movements per day, while some may have a bowel movement after each feeding, whereas rarely have only one-2 bowel movement per week. Infants who breastfeed are rarely constipated. Most formula-fed infants have two to three bowel movements per day depending upon the type of formula food given. Generally, Cows milk, or cow's or soy milk-based formulas cause harder bowel movements and constipation. Partially or completely hydrolysed milk proteins recommended for infants with an allergy or sensitivity to cow's milk, can cause loose bowel movements. By two years of age, a child typically has one to two firm but not hard bowel movements per day and by four years of age, a child usually has one or two formed bowel movements per day [1].
An infant who is constipated typically has bowel movements that look hard or pellet-like. The infant may cry while trying to move their bowels. Bowel movements less frequently than they used to, for example, having a bowel movement every one to two days rather than the previous normal of three to four per day. Chronic constipation is defined as having less than 2 bowel movements a week. Mothers get worried if their infant is straining during a bowel movement, causing their face to turn red. This happens for want of infant’s ability to coordinate muscle movements during bowel movement. Mother may have to help by gently bending their infant's hips and legs up toward the abdomen, which helps to relax the muscles in the pelvis, releasing the bowel movement. The infant probably is not constipated if they pass a soft bowel movement within a few minutes of straining.
A family physician brands the child as having constipation if child has fewer bowel movements than usual or complains of pain during a bowel movement. A child who normally has one to two bowel movements every day may be constipated if they have not had a bowel movement in two days. A child who normally has a bowel movement every two days is not constipated, if the bowel movement is reasonably soft and is not difficult or painful to pass. Faecal impaction is a condition when the constipation becomes so severe that children are unable to pass any formed stool. The causes and risk factors of faecal impaction include- Physical inactivity, Chronic or severe dehydration, Not eating enough fiber, holding in bowel movements, Opioid drug use, Barium enemas, foreign object obstruction, Celiac disease, irritable bowel syndrome (IBS), Inflammatory bowel disease (IBD) and Hypothyroidism, first three reasons being common among infants and young children. Rarely an infant may suffer from Dyssynerigic defecation, which occurs when the nerves and muscles of the pelvic floor do not work together smoothly to produce a normal bowel movement [2]. In grown up children (2+ yrs.) sometimes, functional constipation cases are misdiagnosed as functional abdominal pain because of inappropriate history and examination, as was reported in child of 8 years, who had a history of intermittent moderate to severe abdominal for 3 months refusing digital examination or evacuation. Basic blood investigations and ultrasound of the abdomen normal. Perianal examination revealed an Anal fissure in 6 ‘O’ clock position, and a plain X-ray of the abdomen (AP view) showed the fecoliths and help in the diagnosis [4].
Infants with constipation develop unusual habits when they feel the urge to have a bowel movement like arching their back, tighten their buttocks, and cry. Toddlers may rock back and forth while stiffening their buttocks and legs, arch their back, cross their legs, stand on their tiptoes, and wriggle or fidget or they may squat or get into other unusual positions, hiding in a corner while doing this “dance.”
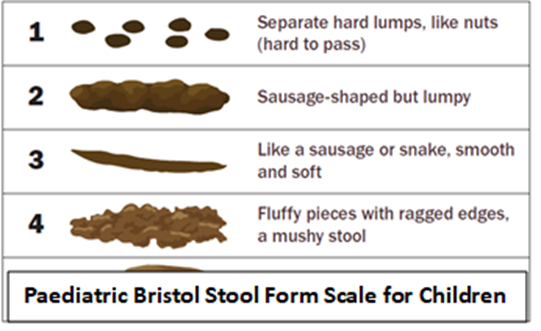
The most important aspect of pooping is the character (or "softness") of the poop. Family Physicians or Paediatricians in India use the Paediatric Bristol Stool Form Scale for Children (see figure) to determine if child's poops are the correct softness. The goal is to ensure poop Type 3 or a Type 4 on the scale.
A household or parents need to try using home remedies first to relieve your child's constipation, which work within 24 hours. some of the remedies for infants older than four months are:
i) Fruit juice About 50-100 mL of 100% Prune, Apple, or Pear juice fruit juice per day for children four to eight months old for a week or two. One can give double of that quantity (180-200 mL) of fruit these juices per day to infants 8 and 12 months old. Too much juice can be unhealthy for children's overall diet and growth, therefore should not be prolonged.
ii) High-fiber foods – If the infant has started eating solid foods, substitute barley cereal for rice cereal. Other high-fiber fruits and vegetables like apricots, sweet potatoes, peaches, plums, beans, peas, broccoli, or spinach. Mother can mix fruit juice with cereal or the fruit/vegetable and little (5-10G) of added sugar.
iii) Fluids –For Infants who are already weaned enough fluid is defined as 16-20 ounces (500-600 mL) of water or other non-milk liquids per day.
iv) A powdered fiber supplement (inulin, psyllium, and methylcellulose) mixed in juice or chewable tablets, can be given
What to avoid or stop at least temporarily:
i) Iron drops (if prescribed) containing higher Iron amount as they cause constipation. Formulas with small quantities of iron need not be stopped.
ii) Milk – Some children develop constipation because they are unable to tolerate the protein in cow's milk. If other treatments for constipation are not helpful, try having the child avoid all cow's milk (and milk products) for at least two weeks.
Approach to toilet training — If a child develops constipation while learning to use the toilet, stop toilet training temporarily. Restarting toilet training after two to three months break. When resumed, encourage the child to sit
on the toilet or potty as soon as they feel the urge to have a bowel movement and give positive reinforcement (for trying, whether the child is successful or not). Avoid punishing or pressuring your child.
Encouraging healthy toilet habits —Encourage them to sit on the toilet for approximately 10 minutes once or twice a day after eating. The child is more likely to have a bowel movement after a meal, especially breakfast.
Providing a foot support: Providing a foot support to the child (a stool under their feet), as was done by me in my son’s case, especially while using an adult-sized toilet helps to relax the muscles in the pelvis and anus. It also provides a place for the child to push against as they bear down and helps the child feel more stable when sitting on the toilet. Let the foot support be high enough so that the child's knees are slightly above their hips level. Reading a story to the child or making them play with a toy or keeping them company while in the bathroom helps to keep the child's interest and encourage cooperation.
Enema cure for chronic constipation in Infants and Children:
An enema is a therapy used for relieving constipation (as a last-ditch effort), after lifestyle changes and stool softeners by mouth haven’t helped in bowel movement among adults or grown-up children. It is of use to treat faecal impaction. It is commonly used to flush out poop before radiological investigation of a mass in the colon or rectum or before surgery in colon or rectum to minimize the risk of infection during surgery. It is also used in inserting medicine directly into the colon to reduce inflammation associated with ulcerative colitis [6].
n enema involves inserting liquid directly into child’s rectum or soap which absorbs fluid in the rectum and facilitates to help the infant to poop. Most households in India traditionally (soap-soaked paper insertion) use them to relieve constipation that hasn’t improved as a last-ditch effort at home. This is resorted if the infant can't poop and lifestyle (increasing water and fiber intake) changes and pelvic floor muscle exercises and Stool softeners by mouth haven't helped to have a bowel movement. PEG and enemas have been proven to be equally effective in achieving disimpaction, but PEG is most recommended in infants because of the more invasive nature of enemas. Current evidence does not support addition of enemas to chronic use of laxatives in children with constipation [7].
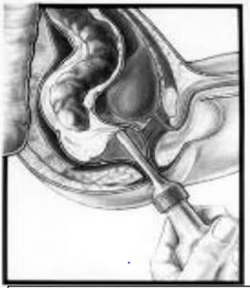
Figure 3: Administration of an enema.
Anal Dilatation:
Due to Dysfunction of the pelvic floor muscles are too tight and unable to relax, it becomes difficult for the infant to pass the stool. This leads to straining during a bowel movement which in turn causes the muscles to tighten even further. If laxatives and stool smotherers do not yield results over weeks in an infant one may have to try dilatation of these muscles and strengthen the pelvic floor muscles by exercises.
Anal Dilation can be done at home by the parents under the guidance of a professional for the first 2-3 times. While a single finger is used for evacuation, as detailed already in our 2nd case report, for dilatation two fingers are introduced and fingers are slowly and steadily stretched (widened) in the anal canal between external and internal sphincters, vertically and horizontally (6 & 12 ‘O’ clock and 3 & 9 ‘O’ clock positions), holding them stretched for about half to minute.
In the hospitals or primary care doctors’ clinics Dilation is done through a series of anal dilators of different sizes. These tools have cylindrical or tapered shapes in five different sizes. These plastic dilators have a rounded tip for smooth insertion, and they also have a disc-shaped base to hold on to during use. The rounded shape of a dilator helps the tool slide into the anal opening. After inserting a dilator, it is left in place for about 30 seconds to stretch the tissue.
For most infants and young children, this process will need to be repeated daily or 2-3 times a week over an extended period as was in our first case report. As progress is made, it can be slowly weaned off, to eventually stop dilation altogether.
Parents are often concerned about giving laxatives, fearing side effects or that the child will not be able to have a bowel movement when the laxative is stopped. Careful use of laxatives can prevent long-term problems with constipation by breaking the cycle of pain and withholding and helping the child to develop healthy toileting habits. Some children need to continue using a laxative treatment for months or even years. After the child has regular bowel movements and uses the toilet alone for at least six months, it is reasonable to decrease and eventually stop the laxative. Laxative use should be combined with dietary changes to reduce the risk of recurrence.
Behaviour changes: ●Encourage your child to sit on the toilet within 30 minutes after each meal (for 10 minutes two to three times per day). ●Design a reward system with your child to recognize the child's efforts.
When to seek professional consultation:
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
