
Research Article | DOI: https://doi.org/10.31579/2641-0419/139Copyright
1Bundeswehrzentralkrankenhaus Koblenz, Klinik I, Rübenacher Str. 170, 56072 Koblenz, Germany 2Medizinische Klinik und Poliklinik II, Universitätsklinikum Bonn, Venusberg-Campus 1, 53127 Bonn, Germany 3GFO Kliniken Bonn, Robert-Koch-Str. 1, 53115 Bonn, Germany
*Corresponding Author: Debabrata Dash, Department of Cardiology, Zulekha Hospital, Sharjah, UAE
Citation: Debabrata Dash, Sreenivas Reddy, Rohit Mody, Shahid A Merchant., (2021) Managing Calcified Coronaries: the Bugaboo of Percutaneous Coronary Intervention. J. Clinical Cardiology and Cardiovascular Interventions, 4(5); Doi:10.31579/2641-0419/139
Copyright: © 2021 Debabrata Dash, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 02 February 2021 | Accepted: 19 March 2021 | Published: 26 March 2021
Keywords: percutaneous coronary intervention; atherectomy; lithotripsy
Background
Percutaneous coronary intervention (PCI) of lesions with heavily coronary artery calcium (CAC) still represents a challenge for interventionists, with increased risk of immediate complications, late failure due to stent underexpansion and malapposition, and consequently poor clinical outcome. In this focused review, we provide the summary of principles, technique and contemporary evidence for various existing and emergent plaque modifying strategies.
Main text
PCI of lesions with heavy CAC still poses a challenge for the interventionists due to an increased risk of incomplete lesion preparation with subsequent suboptimal stent deployment and higher rates of acute and chronic stent failure. With the emergence of many novel devices and technologies, the treatment of lesions with heavy CAC has become increasingly feasible, safe and predictable. It seems likely that combining enhanced intravascular imaging modalities with traditional or new dedicated tools for the treatment of such lesions grant better lesion preparation. This optimizes delivery and deployment of drug-eluting stents translating into improved patient outcome.
Conclusion
The lesions with significant CAC are likely to surge due to aging population and increased rates of diabetes and chronic renal disease. The optimal therapy for such lesions is multi-adjunctive and requires the availability of several modalities including intracoronary imaging which could impact the clinical outcome favourably.
Heavy coronary artery calcium (CAC) poses a real challenge for successful percutaneous coronary intervention (PCI). Treatment of such calcified lesions lead to higher rates of procedural complications, [1] with higher rates of target lesion revascularization (TLR), restenosis, and major adverse cardiac events (MACE). [2-5] Heavily calcified lesions are prone to stent underexpansion and malapposition, which are associated with higher rates of stent thrombosis as well as in-stent restenosis. [6-7] Several strategies and technologies have been crafted to treat CAC with the aim of optimal lesion preparation followed by successful stent deployment. Advances include balloon-based (cutting and scoring balloon, super high pressure balloon and lithoplasty balloon etc) and atherectomy (rotational, laser, and orbital) techniques. Here, the author describes the utility of such modalities in contemporary practice.
2.1 Pathophysiology of CAC
CAC is an active process reflecting a wider systemic inflammatory status, typically observed in patients with metabolic syndrome, diabetes mellitus, or chronic kidney disease. [8,9]It is more common in men older than 70 years of age (>90% in men vs. 67% in women). [10]The incidence of CAC varies according to the imaging modality used. The moderate to severe CAC can be encountered in up to one-third of coronary lesions in coronary angiography (CAG). [11] Atherosclerotic CAC is dysmorphic calcium precipitation created by chondrocyte-like cells and linked to expression of inflammatory factors, such as cytokines released by tissue macrophages and foam cells. It is likely that inflammation precedes calcification and plays an important role in its progression, with the two processes coexisting and promoting each other. [12]CAC is commonly associated with larger plaque burden, multivessel disease and a greater degree of lesion complexity including involvement of coronary bifurcation or chronic total occlusion.11Moreover, specific patterns of CAC, such as calcified nodules and coronary microcalcifications, are related to plaque instability and vulnerability. [13] Typically, these lesions are challenging to cross with standard devices and are less likely to respond to conventional balloon dilatation. Inevitably, inadequate lesion preparation before stenting increases the risk of stent loss, stent underexpansion/fracture and the rate of intraprocedural complications, such as no reflow, coronary dissection, or perforation. [11]Interestingly, the passage of drug-eluting stents (DES) through areas of heavy CAC has also been related to polymer damage with consequent impairment of drug elution.
2.2. Imaging techniques
2.2.1 Coronary computed tomography angiography
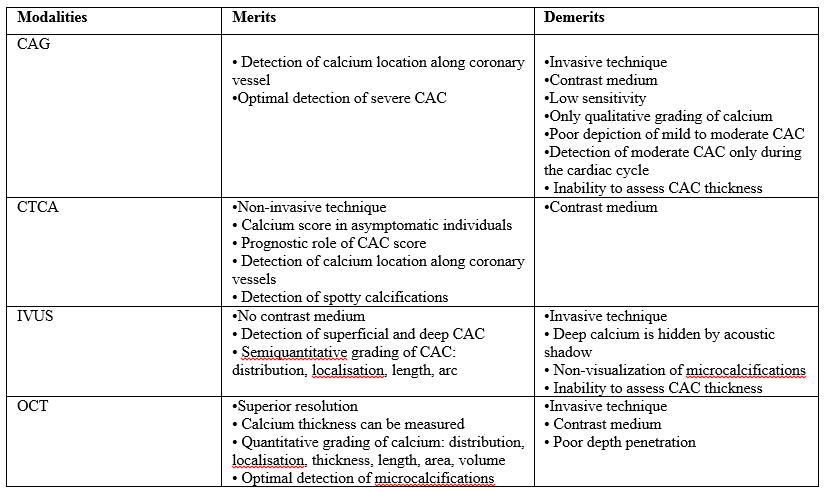
Coronary computed tomography angiography (CCTA) is the most important non-invasive imaging technique used. CAC is depicted as an area of hyperattenuation, defined as an area of at least 1 mm2 with >130 Hounsfield units or ≥3 adjacent pixels using the Agatston method. [14] A CAC score is calculated using a weighted value assigned to the highest density of calcification in each coronary segment that is multiplied by the area and summed finally for all arteries to give a total coronary calcium score correlated with the patient outcomes. [15] This score carries a strong prognostic factor for clinical events in the mid to long term in asymptomatic population. CCTA may uncover spotty calcification which is designated one of the signs of plaque vulnerability. This modality allows accurate identification and localization of calcium along coronary arteries thereby improving procedural success of PCI.
2.2.2 Coronary angiography
Coronary angiography (CAG) is often limited by underestimation of calcium, inaccurate grading, and inability to assess calcium depth within the plaque. CAC is classified as none or mild, moderate, or severe. The radiopacity observed only during the cardiac cycle before injection of contrast medium defines moderate CAC. Severe CAC is delineated as radiopacity observed without cardiac motion, visible on both sides of the arterial lumen, as a double track. [11] The calcium content tends to appear as hazy areas with inhomogeneous contrast staining and hence the differentiation from thrombus is difficult using CAG only. CAG is able to determine CAC only in 38% of cases and the identification seems to be dependent on the degree of the arch of calcification (60% for moderate and 85% for severe CAC) as demonstrated by Mintz et. [16]
2.2.3 Intravscular ultrasound
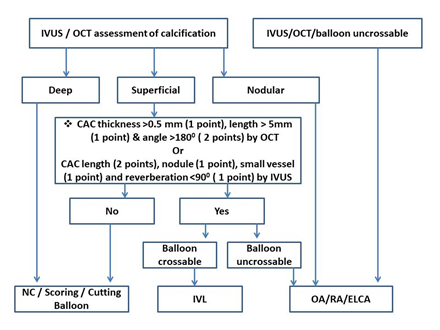
The hallmark of CAC on intravascular ultrasound (IVUS) is an echodense plaque that is brighter than reference adventitia with acoustic shadowing. One of the limitations of IVUS is that dense fibrous tissue may also cast a shadow similar to CAC. CAC brings about reverberations in contrast to dense fibrous tissue. IVUS enhances the sensitivity to in detect CAC significantly compared with CAG (73% of cases vs. 38%; p < 0.001). [16] Quantitatively (the arc of lesion), CAC has been classified into 4 classes on IVUS: Class I, 0°–90° calcification; Class II, 91°–180° calcification; Class III, 181°–270° calcification; and Class IV > 270° calcification. [17] Semiquantitative grading classifies CAC as absent or subtending 1, 2, 3, or 4 quadrants. IVUS determines abluminal calcified deposits within the deeper layers (media or adventitia) of the vessel wall. It allows only definition of the calcific arch, without offering insights into accurate thickness of CAC because of acoustic shadowing. Maximum circumferential extension of calcium >180° is linked to possible stent underexpansion. An IVUS CAC score (Figure 1) of ≥ 2 (2 points for calcium length >2700 > 5 mm, 1 point each for calcium nodule, smaller vessel diameter (<3.5 mm) and reverberation <900) emerges as a relevant predictor for stent underexpansion warranting adjunctive device. [18]

2.2.4 Optical coherence tomography
CAC is designated as signal-poor or heterogeneous region with sharp delineated borders in Optical coherence tomography (OCT). Unlike IVUS, where CAC is most often confused with dense fibrous tissue, OCT detected CAC very often simulates lipid or necrotic core; however, the signal-poor regions of CAC are sharply delineated whereas the signal-poor regions of lipid or a necrotic core have poorly defined or diffuse borders. [19] OCT can measure CAC thickness better due to higher resolution, but may miss deep calcifications because of insufficient penetration. OCT can measure CAC thickness, area, and volume, and automatic quantification of these parameters may be possible (Table 1). [20] A lesion with CAC score of 4 (2 points for CAC angle >1800, 1 point for CAC thickness >0.5 mm, and 1 point for CAC length >5 mm) in OCT has emerged as a reliable predictor for stent underexpansion (stent expansion <70%) as proposed by Fujino et al. [21]
2.3. Treatment modalities
A key concept in approaching heavily CAC involves facilitation of lesion crossing and plaque modification. The support wires, buddy wires, guide extensions, lesion predilatation and anchoring of the guide catheter with inflation of a second balloon in a side branch or distal vessel are possible means for lesion crossing. The underlying calcified plaque gets modified using the dedicated balloon-based (Table 2) and/or ablation (Table 3) devices.

2.3.1 Balloon-based strategies
2.3.1.1 High and super high pressure non-complaint balloons
A non-complaint (NC) balloon may be the first choice in mild to moderate calcified stenosis with restricted calcium arc (<90°). However, the risk of eccentric balloon expansion because of the increased hoop stress conferred by severe CAC, is not fully mitigated by NC balloon. The focal points of resistance within a lesion result in nonuniform balloon expansion and "dog boning" with hyperexpansion in the more compliant segments of the vessel without fracturing the calcium.
Super high-pressure balloon technology incorporates a rapid-exchange NC balloon (OPN Sys Medical, Frauenfeld, Switzerland) with a twin-layer structure allowing inflation pressure up to 35 to 40 atm without bursting of the balloon (Table 2). This is considered as not only effective but also safe approach when experiencing extremely calcified lesions undilatable by conventional high-pressure NC balloon. Although this balloon can be used both before and after stent implantation, most evidence confirms safety and efficacy during post stenting dilation. The unique twin-layer technology ensures uniform balloon expansion over a wide range of pressures, reducing the risk of balloon rupture, vessel damage and coronary perforation. [21] The main limitation of the OPN NC balloon is its relatively high profile which, together with the stiffness of the twin-layer technology, undermines any attempt to recross when inflated. Guide extension catheter may assist successful delivery of such balloon. [22]
2.3.1.2 Cutting and scoring Balloons
The cutting balloon ([FlextomeTM], Boston Scientific, Natick, MA, USA) is a semi-compliant monorail over-the-wire (OTW) balloon with 3 or 4 microtomes mounted on its body, designed to cut the continuity of fibrocalcific plaque creating fissures on the plaque. The cutting balloon ensures a more controlled lesion predilation with less adjacent vessel wall trauma and less risk of dissection. The presence of cutting elements on the surface of the balloon allows effective dilation with a lower inflation pressure (Figure 2).

The microblades also prevent the balloon slippage is prevented by the microblades. One randomized trial failed to show a superiority of cutting balloon for type A/B lesions compared with standard balloons. [23] An IVUS-based study [24] indicated that cutting balloon achieves larger luminal gain compared to conventional balloon. It is limited by high rigidity that hinders lesion navigation through tortuous and calcified vessels. With its most recent iteration (Wolverine) the atherotome’s support thickness has been reduced, without affecting the functional height of the blade, resulting in an overall smaller crossing profile and improved crossability.
The principle of using a “buddy wire” to fracture calcified plaque promoted the development of the scoring balloon: a low-profile semicompliant balloons with a scoring element on the surface (AngioSculpt, Biotronik, Berlin Germany; Scoreflex OrbusNeich, Hong Kong, China; NSA Alpha BBraun, Melsungen, Germany). [25] During inflation, the radial force is mainly exerted on the scoring element and this is transmitted to the vessel wall causing plaque fissuration (Table 2). The embedded nitinol element ensures anchoring of the balloon with a lower risk of “melon-seeding” effects and a lower risk of dissection and perforation. It is likely that prolonged inflation might improve the device navigation with a “creep phenomenon”: a sustained tensile load ensuring microcrack formation and propagation leading to a phasic tissue elongation. [26] Scoring balloons have been considered as an alternative to cutting balloons in moderate calcification and, in recent years, have been preferred due to superior flexibility and deliverability, although no specific randomised control trials exist in the literature so far.
2.3.1.3 Constrained semi-compliant balloon (chocolate balloon)
The chocolateR balloon (TrirReme Medical, Pleasanton, CA, USA) is an OTW balloon with a mounted nitinol constraining structure specifically designed for uniform, controlled inflation and a rapid deflation ensuring an atraumatic dilatation obviating the need for cutting or scoring balloons (Table 2). The nitinol constraining structure generates balloon segments or "pillows" that make contact with the vessel and functions to minimize local forces. The "grooves" promote plaque modification. The distinctive pillows and grooves minimize vessel trauma, reduce the rate of dissection. [22]
2.3.1.4 Intravascular lithotripsy
Intravascular lithotripsy (IVL) is the most recent armamentarium for the treatment of lesions with heavy CAC. It delivers localized pulsatile sonic pressure waves, modifying preferentially calcific plaque without affecting the soft tissue, and subsequently promoting stent delivery and optimization. [27] The balloon catheter with multiple lithotripsy emitters is negotiated over a guidewire to the target lesion. The balloon is attached to the external pulse generator. With balloon inflation at low pressure (4 atm), a burst of 10 pulses of high energy is delivered over 10 seconds followed by further balloon inflation at 6 atm for 15-20 seconds before deflation. This process can be repeated to a total of 8 cycles per balloon (80 pulses). The balloon sizing is based on the desired stent size for that target lesion (ie, 1:1 for the reference vessel diameter) and is often guided by intracoronary imaging. [28] The IVL balloons are all 12 mm long with diameters ranging from 2.5 mm to 4.0 mm. Guide catheter extenders and buddy wire support may be required for deliverability and positioning of this large profile balloon.
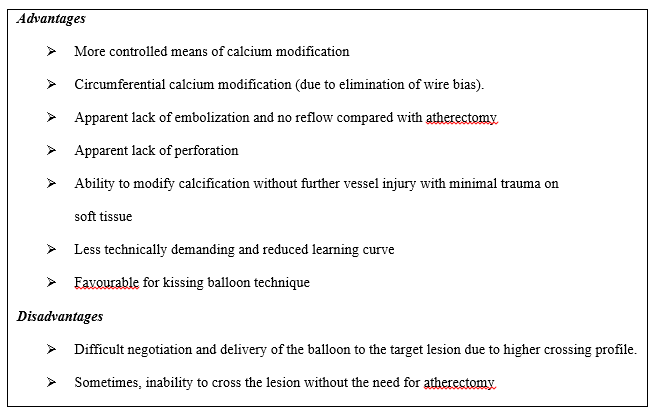
By inducing calcium fractures (as assessed with IVUS or OCT)., [29-31] the IVL therapy achieves optimal stent expansion in undilatable specialty balloons and rotational atherectomy (RA) refractory lesions. The navigation of IVL balloon could be impacted by severe tortuosity or angulation, critical lumen reduction, plaque indentation into the lumen and a small vessels and multiple stent layers. Up to 46% of the lesions might also require dedicated lesion predilatation and/or post-dilatation with NC balloons or could benefit from other adjunctive devices such as cutting or scoring balloons or atherectomy to either facilitate balloon delivery or increase calcium compliance after IVL therapy. [30,32] IVL targets CAC circumferentially and thus avoids guidewire bias. Reduced learning curve, apparent lack of embolization and perforation are all very attractive attributes of IVL as compared to atherectomy (Table 3). [22] Furthermore, IVL is possible following stenting. Unlike RA, IVL can be used with more than one guidewire to protect side branches. Because of the presumed ability to pass across a second balloon, IVL can be used with the kissing balloon technique.
This modality can cause vessel complications although balloon rupture is uncommon. The sudden balloon burst has been described with arterial dissection during lithotripsy therapy. Recently there is a case report of perforation following this therapy.33 Furthermore, vessels with a diameter >4 mm (maximum shockwave balloon size) or important plaque eccentricity preclude appropriate IVL balloon apposition to the vessel wall, and may reduce the efficacy of the therapy. IVL could be safely performed with high procedural success, minimal complications with substantial calcific plaque fracture in most lesions in a prospective multicenter Disrupt CAD II study. [34]
2.3.2 Atherectomy or ablative devices
A strategy of debulking calcified lesions as a part of bail-out technique to address heavy CAC has evolved into a primary lesion preparation approach called primary atherectomy in contemporary practice. Compared to bail-out strategy, the primary atherectomy is associated with decreased procedural and fluoroscopy times, contrast volume, and the number of predilatation balloon catheters used. [35] This alters plaque morphology, inflicting fractures in heavy CAC and changing lesion compliance, to increase the likelihood of maximal MLD and complete stent expansion.
2.3.2.1 Rotational atherectomy
Rotational atherectomy (RA [Boston Scientific, Marlborough, Massachusetts]) system is composed of a high-speed rotating diamond-coated burr aimed to act as an abrasive rotatory surface against calcific plaque. The elliptic-shaped metallic burr is available in different sizes (from 1.25 to 2.5 mm) and is mounted over an advancer (RotaLink) drive-shaft connected to a motor that converts compressed gas into rotational energy. The burr is advanced over a Rotawire (dedicated 0.009-inch 325 cm long wire) designed to maximize flexibility and to minimize wire bias. The recently introduced RotaPro (Boston Scientific) represents an updated iteration and it offers a better user interface and controls integrated on the advancer. Applying the principle of "differential cutting" RA acts preferentially the fibrocalcific plaque tissue while sparing elastic tissue (Figure 3).
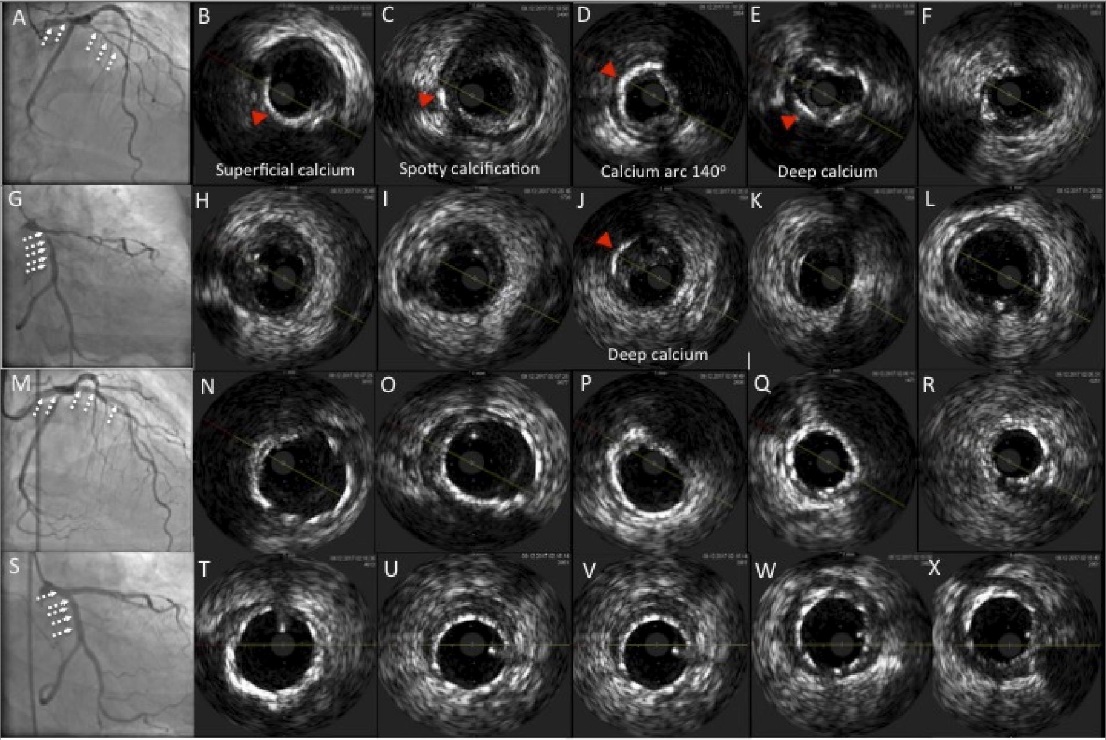
A-F: Baseline lesion in left anterior descending (LAD)
G-L: Baseline lesion in left circumflex (LCX)
M-R: Final result after RA followed by left main bifurcation stenting
S-X: Final result after RA followed by left main bifurcation stenting
A, G, M, S: Angiographic images
B-f, H-L, N-R, T-X: IVUS imaging
Figure 3. Intravascular ultrasound (IVUS) depiction of the effects of rotational atherectomy (RA) on heavy coronary calcium
The ablated tissue is pulverized in 5 to 10 mm debris, which are released into the distal coronary microcirculation. This is the likely mechanism underlying the potential for transient slow/no reflow following RA. [36] The wiring technique has been facilitated by the use of a regular workhorse wire or hydrophilic wire subsequently exchanged over microcatheters or OTW balloons with the rotawire. The RA results are affected by CAC eccentricity, vessel luminal area, burr size and wire bias degree. [37] An optimal scenario for RA in terms of predictable luminal gain is a lesion with concentric circumferential calcium (cross-section >2700 of CAC) and a minimal lumen area smaller than the burr size. Complications of RA include burr entrapment, coronary dissection, and perforation but their occurrence can be usually minimized by optimal technique. Fundamental elements of contemporary optimal technique include use of a single burr (1.5 mm) with burr-to-artery ratio of 0.6, rotational speed of about 140,000 to 180,000 rpm, gradual burr advancement using a pecking motion, short ablative runs (15 to 20 s), and avoidance of decelerations >5000 rpm. However, in lesions not crossable with a 1.5-mm burr or in very long tortuous segments; a 1.25-mm burr with stepwise escalation may be necessary. [38]
ROTAXUS (Rotational Atherectomy Prior to Taxus Stent Treatment for Complex Native Coronary Artery Disease) [39] trial failed to demonstrate a superiority of RA versus conventional balloon dilatation before DES implantation in heavy CAC. Upfront high-speed RA is feasible in nearly all patients and improves the success of DES deployment compared with modified cutting or scoring balloons, according to results of the contemporary Comparison of Strategies to PREPARE Severely CALCIFIED Coronary Lesions (PREPARE-CALC) trial. Although both strategies ensure equal safety and efficacy, the use of RA is no longer associated with excessive late lumen loss in the modern era. [40]
2.3.2.2 Orbital atherectomy
Orbital atherectomy (OA) is another novel treatment modality for heavy CAC. [31] It consists of an eccentrically mounted diamond-coated 1.25-mm crown, connected to a drive shaft and to a controller powered by a pneumatic console (CSI Diamond 3600 Coronary Orbital Atherectomy System, St. Paul, Minnesota). Compared with the rotaburr, which only allows calcium ablation during forward advancement, the crown of OA with diamond chips both on front and back, enables bidirectional atheroablation (Table 4).
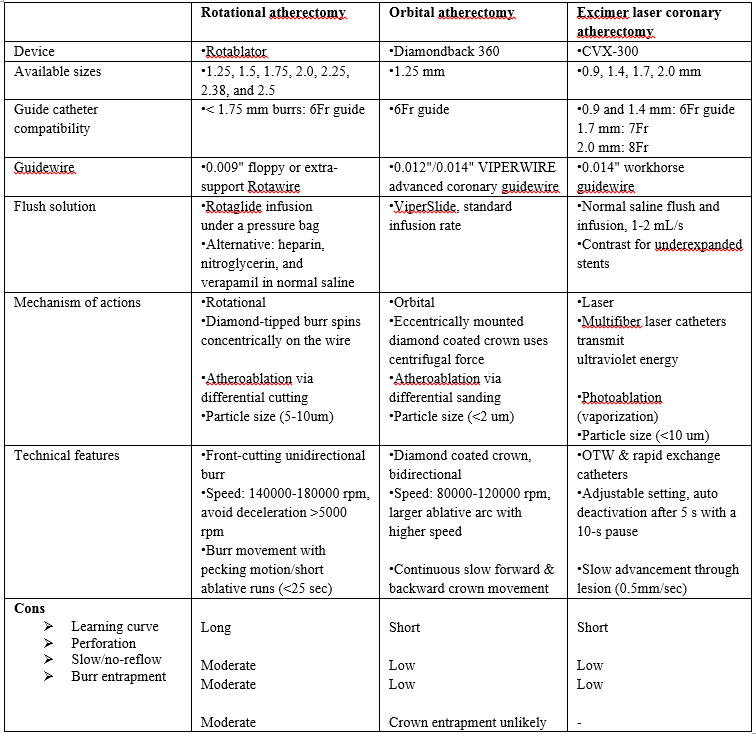
The crown entrapment is less likely as compared to burr entrapment due to retrograde ablation. The crown is advanced over a dedicated (ViperWire Advance, St. Paul, Minnesota) a 0.014-inchwire, with superior maneuverability compared with the 0.009-inch Rotawire. Using the controller, the operator can move the crown forward and backward and can regulate the speed of the crown orbit (80,000 to 120,000 rpm). OA incorporates centrifugal forces which pushes and compresses the crown against the plaque with a “sanding” action of the calcified component. OA might have a selective action on the rigid calcified component, whereas healthy elastic tissue may be spared. Whereas the RA burr is moved forward in a slow, pecking motion to allow intermittent ablation; the OA crown is advanced with a gradual, continuous motion, even interrupting in a region of interest to permit more time for ablation. Notably, by increasing its orbit as rotational speed increases, OA allows ablation of CAC using the same device (1.25-mm crown) in vessels up to 3.5-mm diameter. Other advantages of OA include the 6-F guiding catheter compatibility, smaller size of particles released during ablation (2 vs. 5 to 10 mm in RA), no interruption in blood flow during crown orbiting, and less vascular heating.
For moderate degree of CAC, the lesion preparation could be achieved with balloon-based approaches. Conversely, higher degree of CAC may require more aggressive ablative approaches, such as ELCA, RA or OA. Because of its ease of use, shorter
learning curve, and unique action on both superficial and deep CAC, IVL has the potential of more widespread adoption.
The authors feel that there would be a surge in a hybrid approach involving drill (RA or OA) and shock (IVL) in near future. Despite the growingdata for various modalities, additional randomized controlled trials are warranted to further clarify the superiority of one modality over another.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
