
Research Article | DOI: https://doi.org/10.31579/2640-1045/012
*Corresponding Author: R F Gross man, Department of Endocrinology, Diabetics,Israel
Citation: R F Gross man , Sami Micheal. Management Thyroid Disease in Pregnancy: Preconception, and the postpartum complications. J. Endocrinology and Disorders. DOI:10.31579/2640-1045/012
Copyright: © 2017. R F Gross man. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 03 August 2017 | Accepted: 09 September 2017 | Published: 27 September 2017
Keywords: thyroid disorders, pregnancy, hypothyroidism
Pregnancy has a profound impact on the thyroid gland and thyroid function since the thyroid may encounter changes to hormones and size during pregnancy. The diagnosis and treatment of thyroid disease during pregnancy and the postpartum is complex but knowledge regarding the interaction between the thyroids and pregnancy/the postpartum period is advancing at a rapid pace.
For women known to have hypothyroidism, an increase in thyroxine dose by 20–40% when pregnancy is confirmed usually ensures they remain euthyroid. Treatment of subclinical hypothyroidism is recommended if the woman has antithyroid antibodies.
Treatment of hyperthyroidism, unless it is related to human chorionic gonadotrophin, involves propylthiouracil in the first trimester. Carbimazole may be used in the second trimester. Thyroid function tests are checked every month and every two weeks following a change in dose.
Women with a current or a past history of Graves’ disease who have thyrotropin receptor antibodies require early specialist referral as there is a 1–5% risk of fetal hyperthyroidism.
Women with thyroid disorders in pregnancy should be followed up by their GP in the postpartum period. Postpartum thyroiditis may present months after delivery.
Thyroid disorders are common in pregnancy and related to maternal and fetal complications.
Hyperthyroidism occurs in 0.1–0.4% of pregnant women. Whereas about 2–3% of pregnant women are hypothyroid, of whom 0.3–0.5% have overt hypothyroidism and 2–2.5% present subclinical hypothyroidism.
At least 5–10% of women are positive for thyroid antibodies and have an increased risk of developing a certain degree of thyroid insufficiency during pregnancy.
Thyroid function is influenzed by pregnancy and its dysfunction is associated with maternal and fetal morbidity. Moreover the role of subclinical hypothyroidism in the developement of fetal and maternal complications is not univocal. Indeed subclinical hyperthyroidism is not associated with adverse outcomes. Thyroid autoimmunity appears to be associated with an increased risk of miscarriage and preterm delivery.
In this article we aimed to review the possible adverse maternal and fetal outcomes of thyroid during pregnancy and the proper management of these conditions to avoid such complications.
Physiology of maternal and fetal thyroid in pregnancy
During pregnancy the thyroid gland undergoes hyperplasia and increased vascularity. Circulating iodine is reduced and thyroid-binding globulin increases.
The rising concentration of beta-human chorionic gonadotrophin (HCG) in the first trimester can directly stimulate the thyroid stimulating hormone (TSH) receptor as HCG has structural similarities to TSH. This in turn leads to increased free triidothyronine (fT3) and free thyroxine (fT4), suppressing TSH secretion. A serum TSH below 0.1 mIU/L may be present in 5% of women by the 11th week of pregnancy.
The TSH subsequently normalises as beta-HCG falls in the second and third trimesters.
In view of these physiological changes, consult gestation-specific TSH concentration ranges when interpreting thyroid function tests. These reference ranges differ from non-pregnant ranges (Table 1).
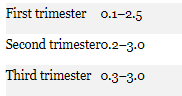
Note that individual laboratories may have slightly different pregnancy-specific ranges and it is important to confirm ranges with your local pathologist.
Women with hypothyroidism
After conception, an increase in thyroxine as soon as possible is recommended with the goal of normalising the TSH concentration. An easy approach is to increase the total weekly thyroxine dose by an extra two tablets per week or by 20–30% of the baseline dose when pregnancy is confirmed.
Serum TSH should be monitored every four weeks in the first trimester to ensure the woman is euthyroid, and then six to eight weekly therafter.Thyroid function tests should be rechecked four weeks after any dosage adjustments to ensure euthyroid levels are maintained. Aim to maintain TSH in the range 0.5–2.5 mIU/L.
Failure to achieve a euthyroid state despite appropriate therapy necessitates investigation into causes for a lack of thyroxine uptake. This can result from poor adherence to therapy or impaired absorption. Women should be advised to take their thyroxine on an empty stomach before breakfast. There should be a 4–5 hour gap before taking medicines such as vitamins, calcium and iron tablets as interactions in the gastrointestinal tract can reduce thyroxine absorption.
Following delivery, the thyroxine dose should be reduced to the patient’s preconception dose, assuming the woman was euthyroid on that dose. Check thyroid function tests 4–6 weeks after their dose has been reduced postpartum.
Hypothyroidism diagnosed during pregnancy
A new diagnosis of overt hypothyroidism should warrant immediate thyroxine replacement and further investigation for the presence of thyroid auto-antibodies:
antithyroid peroxidase antibodies (antiTPO)
antithyroglobulin antibodies (TgAb)
thyrotropin receptor antibodies (TRAb) (if there is a history of treated Graves’ disease).
Subclinical hypothyroidism
Subclinical hypothyroidism in pregnancy is associated with an increased risk of recurrent miscarriage, intrauterine growth restriction, preterm birth, low birth weight, perinatal mortality and pre-eclampsia.Thyroxine may reduce associated risks Recent studies support thyroxine replacement in women with subclinical hypothyroidism undergoing assisted reproduction technologies, to improve pregnancy outcome. The aim of treatment is to achieve a TSH less than 2.5 mIU/L.
The American Thyroid Association in 2017 updated its guidelines for the management of thyroid disease in pregnancy following new research. Thyroxine should be given if there are antithyroid antibodies and the initial TSH is 2.5–4 mIU/L. If the initial TSH is 4 mIU/L or more, start thyroxine irrespective of antibody status.
If a decision is made to treat subclinical hypothyroidism, the suggested starting dose of thyroxine is 50 micrograms per day. Thyroid function tests are checked within four weeks of starting therapy.
As the pregnancy advances, dose requirement comes down in most of the cases; one-third of pregnant women can actually stop anti-thyroid medication in the third trimester. A significant percentage of these women need to start after delivery for relapse. Our routine practice is to check the thyroid function two weeks after delivery as opposed to six to eight weeks in cases of hypothyroidism. Beta-blockers, if necessary, can be given for a short duration for controlling symptoms. When thyroidectomy is needed for the control of hyperthyroidism, it should be planned in the second trimester of pregnancy; fortunately, this is very rare, and none of the authors can remember a single case they referred to surgeons for uncontrolled hyperthyroidism in pregnancy.
Breast feeding while on anti-thyroid medication remains a sensitive issue; PTU is the preferred medicine as it is more protein-bound and is secreted least in breast milk. Up to 600 mg a day PTU is considered safe; it is recommended to keep an eye on growth of the baby clinically with biochemical test for thyroid function if suspected for growth problem.
Showing the thyroid function and treatment of a patient with Graves' disease in pregnancy treated by the authors

Gestational hyperthyroidism or gestational thyrotoxicosis is used when there are symptoms of hyperthyroidism due to the high levels of HCG, which causes thyroid hyperfunction. This condition needs to be differentiated from Graves' disease, as most of the symptoms are similar to those in pregnancy. Up to 15% of normal pregnancy TSH can be suppressed due to hCG effect; they do not require extra treatment; careful observation is good enough. There is another entity in pregnancy called transient gestational thyroticosis, where free thyroid hormone can be increased, and they require a short course of anti-thyroid medication. Gestational thyrotoxicosis is usually transient and recovers over a period of few weeks. This is essentially a retrospective diagnosis.
Management
The goal of treatment is to keep the patient euthyroid, using the lowest possible dose of antithyroid drugs necessary to maintain FT4 levels in the upper one-third of the normal non pregnant range or just above the normal range excessive doses of ATDs, indeed, may affect fetal thyroid function, with the development of hypothyroidism and/or goiter
The dose should be adjusted every 2–4 weeks and the presence of detectable TSH is an indication to decrease ATD dose
The treatment of choise is propylthiouracil (PTU), but methimazole (MMI) is also an alternative, both are considered compatible with breastfeeding. PTU is given in a dose of 100–450 mg/day. It may be necessary 2–4 weeks from the start of treatment to see a clinical change. MMI can be prescribed at 10–20 mg/day. Beta blockers may be, also, used to control the adrenergic symptoms of thyrotoxicosis. In addition, beta blockers block the peripheral conversion of T4 to T3. Propranolol in a dose of 10–40 mg every 4–6 h or atenolol 25–50 mg daily, are recommended. In acute cases, intravenous esmolol (up to 200 ∝g/kg/minute) may be used to maintain a heart rate of less than 90 beats/min. Thyroidectomy is reserved for patients requiring high doses of medication or in the rare case of allergies to ATD.
The use of iodine therapy in addition to anti-thyroid medications has fallen into disuse due to higher rates of neonatal goiter and hypothyroidism. Radioactive iodine therapy is contraindicated in pregnancy and lactation. It is recommended to continue medications throughout the postpartum period.
It is well documented that thyroid disorders are associated with maternal and fetal complications during gestation and sequelea after delivery.
Despite the correlation between thyroid function during pregnancy and maternal and fetal outcomes is a widely discussed topic, it remains to clarify several points.
While ADT therapy does not appear to be relevant in patients with subclinical hyperthyroidism, in cases of overt hyperthyroidism it plays a key role.
In pregnant women with newly diagnose of overt hypothyroidism it is strongly recommended to begin substitutive treatment with LT4 as soon as possible, that should be considered in case of subclinical hypothyroidism; hypothyroid women already being treated by LT4 require an increase of dosage by 30–50% at the start of pregnancy. In this review we tried to evaluate possible strategies to prevent and to apply appropriate management to avoid an unfavorable outcome for both mother and offspring.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
