
Review Article | DOI: https://doi.org/10.31579/2692-9759/076
Clinic of Gastroenterology, Second MHAT Sofia – Sofia, Bulgaria
*Corresponding Author: N. Tsonev, Clinic of Gastroenterology, Second MHAT Sofia – Sofia, Bulgaria.
Citation: N. Tsonev , D. Vandeva, K. Toncheva, D. Zvezdov. (2022). Management Of Therapy of Anticoagulants and Antiplatelets in Acute Gastrointestinal Bleeding and In the Periendoscopic Period. Cardiology Research and Reports. 4(4); DOI:10.31579/2692-9759/076
Copyright: © 2022 N. Tsonev, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 29 September 2022 | Accepted: 10 October 2022 | Published: 16 November 2022
Keywords: anticoagulants; antiplatelet agents; gastrointestinal bleeding; management
Management of anticoagulant and antiplatelet therapy is a common clinical problem in case of urgent or elective gastrointestinal endoscopic procedures. Anticoagulants and antiplatelet agents are widely used drugs for cardiovascular prevention and reducing the risk of thromboembolic events. Gastrointestinal bleeding represents a serious complication of their use. It’s recommended temporary interruption of anticoagulants in clinically significant gastrointestinal bleeding. For the antiplatelet therapy the decision is when to stop and restart the therapy, depending on whether it’s for primary or secondary cardiovascular prevention. Treatment with antithrombotic drugs in the periprocedural endoscopic period is based on balancing the bleeding risk against the thromboembolic risk. It’s recommended temporary discontinuation of antithrombotic treatment in high-risk endoscopic procedures with high risk for bleeding and to consider the use of “bridging” therapy with LWMH for patients on vitamin K antagonists who are at high thrombotic risk. Antithrombotic agents in endoscopic procedures with lower bleeding risk are not needed to be withheld. Evaluating cardiovascular risk and management of antithrombotic therapy could be a challenge for gastrointestinal endoscopists, therefore collaboration with a cardiologist is of great importance, at least for some patients.
Anticoagulants and antiplatelets are widely used drugs for several cardiovascular and thrombotic conditions. These drugs increase the risk of bleeding during endoscopic procedures and discontinuation of their administration carries a risk for thromboembolic events. The assessment of whether and when to interrupt and reverse the antithrombotic drugs intake in case of urgent or elective gastrointestinal endoscopy creates difficulties, as the thrombotic risk and the risk of bleeding are different for each patient [1].
In case of GIT bleeding, the coagulation status (platelets, INR and aPTT) must be examined, and the correction of coagulation is carried out depending on the situation. In case of acute bleeding, endoscopic intervention can be performed regardless of laboratory parameters. Significant disorders in hemostasis are corrected regardless of the time of endoscopy. A study on the routine examination of coagulation status before endoscopic or surgical treatment showed no correlation with the actual incidence of bleeding without a history of predisposing disease or previous hemorrhage [2]. The anamnestic history reveals evidence of acquired or congenital coagulopathy, for example bleeding from a previous procedure, diseases associated with an increased risk of bleeding Ehler Danlos, Marfan syndrome congenital thrombocytopathies, congenital plasma coagulopathies, Willebrand syndrome, congenital deficiency of Factor VIII and IX, acquired platelet dysfunction and coagulopathies in liver, nephrological diseases, long-term biliary obstruction, long-term antibiotic treatment, malnutrition or myeloproliferative diseases [2].
When should antiplatelet and anticoagulant therapy be stopped and in which diseases should it be continued? There are no established data on the optimal INR for emergency endoscopy.A retrospective analysis of patients with supratherapeutic INR (INR > 4) and patients with therapeutic values reported similar outcomes for recurrent bleeding, need for blood transfusion, and hospital mortality [3]. In an English study, results differed, reporting poorer endoscopic bleeding control at INR > 1.5 [4]. Some authors recommend an INR < 2>2.5 OR 7.9) and of mortality in non-variceal GIT bleeding (INR>1.5 OR 5.6 [10]. This is indicative of the role of INR as an indicator of comorbidities. Neutralization of the effect of anticoagulant therapy in acute gastrointestinal bleeding is based on the use of IV vitamin K, fresh frozen plasma, and concentrated prothrombin complex for warfarin users [11,12] and activated charcoal - oral, hemodialysis, idarucizumab or prothrombin complex for DOAC users [13,14]. The effect of prothrombin complex in DOAC hasn’t been studied. A heparin bridge does not significantly alter the risk of rebleeding and thromboembolism in gastrointestinal bleeding [9]. In a retrospective study in patients treated with warfarin, a higher rate of bleeding was reported in the non-bridging group, with no difference in periprocedural thromboembolism [15].Similar results were also reported in periprocedural DOAC users [16].
When to resume taking of anticoagulants? A meta-analysis showed that restarting anticoagulants reduced the incidence of thrombotic events in patients with discontinued therapy due to bleeding (HR 0.68 95 Percentage CI 0.52-0.88) and mortality (HR 0.76 95 Percentage CI 0.66- 0.88) without significantly increasing the incidence of recurrent bleeding (HR 1.20 95 Percentage CI 0.97-1.48) [17].
A study comparing the administration of DOAC and warfarin showed that the incidence of recurrent bleeding at day 90 after endoscopy was similar in the DOAC-resumed and non-resuming groups. In this study, a history of venous thrombosis was associated with thromboembolic events (HR 3.30 95 Percentage CI 1.29-7.38) [18]. Another study determined the risk of acute gastrointestinal bleeding with anticoagulant use based on five factors (absence of PPI, chronic kidney disease, COPD, ulcer history, and liver cirrhosis). The new statistical rating system (0.65) outperforms that of HAS-BLED (0.57) [18,19].
Anticoagulants and risk of bleeding in elective endoscopic procedures
Annually, about 10 Percentage of patients taking anticoagulants require temporary discontinuation of therapy due to surgical or other invasive elective procedures, such as gastrointestinal endoscopy [20]. A serious complication of anticoagulant therapy is severe GIT bleeding, with an incidence of approximately 1-4 Percentage per year and a fatal incidence of up to 10 Percentage [21,22 ]. About 15 Percentage of patients with acute upper GIT bleeding and up to 32 Percentage of patients with lower GIT bleeding take anticoagulants [23,24].
The recommendations of the British Gastroenterology Association (BSG) and the European Gastrointestinal Endoscopy Association (ESGE) for anticoagulant therapy in patients undergoing routine endoscopy are based on stratification of patients at risk categories according to the risk of bleeding in the endoscopic procedure and thromboembolic risk (table. 1 and table. 2) [25,26].
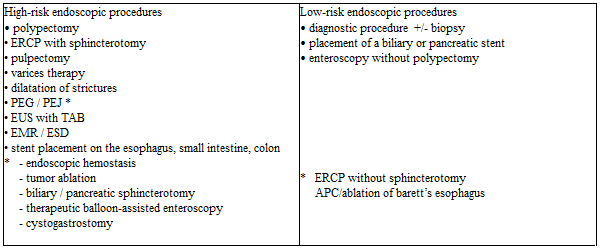
Тable 1: Endoscopic procedures with high and low risk of [25,26,27]
ERCP - endoscopic retrograde cholangiopancreatography; PEG - percutaneous endoscopic gastrostomy; PEJ - percutaneous endoscopic jejunostomy; EUS – endoscopic ultrasound; TAB - fine-needle aspiration biopsy; EMR - endoscopic mucosal resection; ESD - endoscopic submucosal dissection; APC - argon plasma coagulation
* Endoscopic procedures included in the guideline of the American Society of Gastrointestinal Endoscopy

*AF – atrial fibrillation
Таble 2: Conditions with high and low thromboembolic risk [25,26].
Studies have found that gastrointestinal bleeding is a typical complication of vitamin K using antagonists as a difference in risk between vitamin K antagonists (VKA) and direct-acting oral anticoagulants (DOAC) were not observed [21]. A meta-analysis involving 23 prospective studies, comparing the use of DOAC (apixaban, dabigatran, edoxaban, and rivaroxaban) and vit K antagonists on the risk of massive gastrointestinal bleeding, did not show any difference (RR 1.08) [28]. A meta-analysis of 43 prospective randomized trials reported a slightly increased risk of gastrointestinal bleeding with DOAC compared to vit. K antagonists (OR 1.45) [29]. A Finnish study in 100,000 patients reported a risk of 2.3 Percentage per year for hospitalized ones for gastrointestinal bleeding at the start of therapy and 0.9 Percentage during long-term treatment. The risk was the highest in the first 30 days of initiating anticoagulant therapy [30]. The risk of severe bleeding also depended on comorbidity, concomitant therapy, duration of anticoagulant therapy, and indications for anticoagulation (the incidence is 2.5 Percentage in patients with atrial fibrillation and 0.5 Percentage in patients with pulmonary embolism) [28].
The risk of bleeding increases when using an anticoagulant with an antiplatelet agent and especially with two antiplatelet agents. The “Stent Anticoagulation Restenosis Study” reported a higher number of bleeding events with an anticoagulant and Aspirin compared to the Aspirin-only group - 6.2 Percentage to 1.8 Percentage [31], as bleeding events from the GIT were not reported. In a retrospective analysis of 666 patients on triple therapy with aspirin, clopidogrel, and enoxaparin, with short-term use in patients with acute coronary heart disease, gastrointestinal bleeding was observed in 2.7 Percentage of the patients on day 30 [32]. In a Danish retrospective study of 118,606 patients, bleeding cases were reported with triple therapy with aspirin, clopidogrel, and vit. K antagonist - 15.7 Percentage per year, and in a double therapy group with vitamin K antagonist and clopidogrel - 13.9 Percentage per year [33]. Comparing monotherapy with vitamin K antagonist with dual therapy with clopidogrel, a 3.1-fold increase in risk and respectively 3.7-fold increase with triple therapy was reported. The gastrointestinal bleeding was 5.1 Percentage per year, a 5.38 times increase compared to oral anticoagulant monotherapy. The risk of bleeding after myocardial infarction with triple therapy was 1.4 times higher than with vitamin K antagonist therapy and antiplatelet agent. The proportion of patients with fatal GIT bleeding compared with non-fatal cases was 45.3 Percentage to 33.8 Percentage [34]. In a prospective study where the bleeding was targeted, a significantly higher frequency was reported. Episodes of bleeding were reported annually in 19.4 Percentage of patients on dual therapy and in 44.4 Percentage of patients on triple therapy, with 2 Percentage to 8.8 Percentage of patients experiencing GIT bleeding [35].
In the study by Sorensen et al., the risk of hospitalization due to hemorrhage associated with various antithrombotic regimens was investigated. It covered 40,812 patients over the age of 30 who were admitted to a hospital with myocardial infarction for the first time. They were divided into the following groups: monotherapy with aspirin, clopidogrel, or vitamin K antagonist; double therapy with aspirin plus clopidogrel, aspirin plus vitamin K antagonist, or clopidogrel plus vitamin K antagonist, or triple therapy involving all three drugs. The risk of bleeding, recurrent myocardial infarction, and death has been assessed. During the mean follow-up of 476.5 days (SD ± 142.0), 1891 (4.6 Percentage) patients were admitted to the hospital with bleeding. The annual bleeding rate was 2.6 Percentage for the aspirin group, 4.6 Percentage for clopidogrel, 4.3 Percentage for the vitamin K antagonist, 3.7 Percentage for the aspirin plus clopidogrel, 5.1 Percentage for the aspirin plus vitamin antagonist. K, 12.3 Percentage for clopidogrel plus vitamin K antagonist and 12.0 Percentage for triple therapy. With aspirin as the reference drug, the corrected risk factor for bleeding was 1.33 (95 Percentage CI 1.11-1.59) for clopidogrel, 1.23 (0.94-1.61) for vitamin K antagonist, 1.47 (1.28-1.69) for aspirin plus clopidogrel, 1.84 (1.51-2.23) for aspirin plus vitamin K antagonist, 3.52 (2.42-5.11) for clopidogrel plus vitamin K antagonist, and 4.05 (3.08-5.33) for triple therapy. 702 (37.9 Percentage) of 1852 patients with non-fatal bleeding had a recurrent myocardial infarction or died during the study period compared with 7178 (18.4 Percentage) of 38 960 patients without non-fatal bleeding (HR 3.00, 95 Percentage CI 2.75-3.27, p less than 0.0001). In patients with myocardial infarction, the risk of bleeding increases with the number of antithrombotic drugs used [36].
According to the recommendations of BSG and ESGE, anticoagulants could be continued in low-risk endoscopic procedures but should be discontinued in all high-risk procedures. In procedures with a low risk of bleeding, the INR values should be checked one week before the procedure and should be at therapeutical limits. For INR values above therapeutical limits but below 5, it is recommended to reduce the daily dose until therapeutic levels are reached. Discontinuation of VKA may also be considered in diagnostic procedures that are likely to become high-risk, such as colonoscopy polypectomy [25,26]. In this regard, studies have shown that it is safe to perform a polypectomy of a colon polyp below 10 mm without interrupting the VKA, provided that endoscopic clips are prophylactically inserted [37] or that an end loop polypectomy technique is used to reduce the risk of late bleeding [38].
In patients on vitamin K antagonist therapy who is undergoing an endoscopic procedure with a high risk of bleeding but a low thrombotic risk is recommended to discontinue vitamin K antagonist intake 5 days before the procedure for Warfarin, 3 days for acenocoumarol. For this period, the INR values reach ≤ 1.5 in 93 Percentage of patients. After the endoscopic procedure, the intake of vitamin K antagonist can be restored on the same day at the usual daily dose [25,26].
In endoscopic procedures with a high risk of bleeding and conditions with a high thrombotic risk, it is recommended to discontinue the oral anticoagulant and switch to bridging therapy with a direct-acting parenteral anticoagulant, usually low molecular weight heparin (LMWH) /100 UI / kg 2x / to reduce the periprocedural risk of thromboembolism.
LMWH should be discontinued 24 hours before the procedure and resumed the next day in low-risk post-procedural bleeding or after 48 hours in high-risk post-procedural bleeding (according to the 2012 ACCP guideline) [39]. On the other hand, ESGE's recommendations for bridging heparin therapy do not include patients who are traditionally considered to be at high risk for thromboembolic events, such as those with non-valvular atrial fibrillation and previous thromboembolic events and/or CHADS2 score 5 or 6, and those with recent (up to 3 months) venous thromboembolism [20].
After decades in which vit. K antagonists were the only oral anticoagulants, the spectrum of these drugs was expanded to include a new class of drugs, such as direct oral anticoagulants - directly inhibiting thrombin/dabigatran - Pradaxa® / or activated factor Xa (Rivaroxaban – Xarelto®; Apixaban- Eliquis®). DOAC has several advantages over vit. K antagonists - due to more predictable pharmacokinetics, are prescribed in a fixed-dose, no routine monitoring of coagulation status is required. The rapid onset of action / 1-4 hours / and short half-life / 9-17 hours / makes the initiation and interruption of therapy relatively easier and safer than vitamin K antagonists [1].
There is also a risk of bleeding when taking DOAC. In a retrospective study in patients stratified into three age groups with non-valvular atrial fibrillation and dabigatran, rivaroxaban, or apixaban, Mayo researchers evaluated the incidence of total GIT bleeding and compared rivaroxaban with dabigatran in 31,574 patients, apixaban with dabigatran in 13,084 patients and for apixaban with rivaroxaban in 13,130 patients. Apixaban was found to have the most favorable safety profile for GIT compared to dabigatran and rivaroxaban in the three age groups. Rivaroxaban has the most unfavorable safety profile for the GIT. Patients using apixaban were 61% less likely to experience GIT bleeding than those on dabigatran (HR 0.39; 95% CI, 0.27-0.58). Dabigatran patients were 20% less likely to bleed than rivaroxaban (HR, 1.20; 95% CI, 1.00-1.45). It is observed that the cases of bleeding from the GIT in patients taking DOAC increase with age, with the greatest risk observed in persons aged 75 years and older. The researchers concluded that Apixaban had the safest profile of the three drugs studied in this age group [40].
Due to the short half-life of DOAC, they can be discontinued hours before the endoscopic procedure, and due to the rapid onset of action, anticoagulation is achieved within a few hours after inclusion [1]. These pharmacokinetic properties of DOAC eliminate the need for bridging heparin therapy. On the other hand, this class of drugs is not indicated for use in patients at high thrombotic risk [25,26].
For endoscopic procedures with a low risk of bleeding, ESGE recommends skipping the morning dose of DOAC. The optimal window for the endoscopic procedure is considered to be when the anticoagulant effect is relatively low - about 10 hours after the last dose for drugs taken twice daily and about 20 hours - for the once-daily medication (Rivaroxaban). In high-risk procedures - the last dose is recommended to be taken 48 hours before the endoscopic procedure, for Dabigatran (with CrCl - 30-50 ml/min) - 72 hours before the manipulation [25,26].
Antiplatelet agents are widely used drugs in clinical practice, mainly for primary and secondary prevention of cardiovascular diseases [41]. The use of antiplatelet agents has been associated with outweighing clinical benefits [42], but may nevertheless cause upper and lower GIT bleeding [43,44,45]. Antiplatelet agents lead to the formation of erosions and ulcers in the duodenum and stomach and can provoke bleeding from existing ones [43]. The role of antiplatelet agents for bleeding from the large intestine, mainly from diverticula [45], as well as for bleeding from the small intestine, mainly in erosive enteropathy, is also discussed [44]. Antiplatelet agents also increase the risk of bleeding on endoscopy. A retrospective study suggests that the risk of bleeding in mucosal biopsy varies between 0.02 Percentage -0.1 Percentage, increasing in those patients taking antiplatelet agents as well as with the number of biopsies [39]. In a prospective study, a bleeding episode requiring endoscopic hemostasis was observed in 2.2 Percentage of 1015 patients who underwent polypectomy of colonic polyps less than 10 mm with an endoloop technique. In this study, antiplatelet monotherapy (aspirin or ticlopidine) was associated with a 4-fold increase in the risk of bleeding (95 Percentage CI 1.5-10.6) [46]. A study by Lanas and Gargallo found that the risk of severe upper GIT bleeding was high when two antiplatelet agents were included in the therapy and were increasing 1.8-fold with low-dose aspirin and 7.4-fold with aspirin and clopidogrel [47].
A meta-analysis of prospective studies involving more than 100,000 patients found that the risk of total bleeding (OR 1.70) as well as of severe or significant bleeding (OR 1.31) was increased with medications [48]. Another meta-analysis showed an increase in the risk of bleeding annually by 0.13 Percentage for severe bleeding and by 0.12 Percentage for light bleeding with prolonged use of aspirin. The relative risk remains 2.22 for severe gastrointestinal bleeding and 1.23 for fatal bleeding [49]. The CAPRIE STUDY showed a lower risk of gastrointestinal bleeding with Clopidogrel compared to Aspirin (RR 1.45) [50]. The use of an antibody against GP2II3a in patients with myocardial infarction increases the risk of bleeding [51]. The risk of bleeding from GIT with double antiplatelet therapy was found to be higher than with monotherapy and reaches HR 2.7 [52]. In triple antiplatelet therapy, when cilostazol was added to aspirin and clopidogrel, the same risk of bleeding was observed compared to dual antiplatelet therapy - 2.39 Percentage vs. 2.04 Percentage, but the risk of gastrointestinal bleeding was significantly higher with triple anti-aggregation (OR 2.46) [ 53]. In the study of Luis et al., the risk of upper gastrointestinal bleeding associated with the use of low doses of acetylsalicylic acid (75 to 300 mg / d) alone and in combination with other gastronomic drugs was assessed in 2049 patients. Researchers found that the risk of upper GIT bleeding was increased in low-dose aspirin (RR, 1.80; 95 Percentage CI, 1.59 to 2.03) or clopidogrel users(RR, 1.67; 95 Percentage CI, 1.24 to 2.24) compared with non-users. The risk of upper GIT bleeding was significantly increased when aspirin is used in combination with clopidogrel (RR 2.08; 95 Percentage CI, 1.34 to 3.21), with oral anticoagulants (RR 2.00; 95 Percentage CI, 1.15 to 3.45), low/medium dose nonsteroidal anti-inflammatory drugs (RR 2.63; 95 Percentage CI, 1.93 to 3.60), high dose nonsteroidal anti-inflammatory drugs (RR, 2.66; 95 Percentage CI, 1.88 to 3.76) or with high-dose oral corticosteroids (RR, 4.43; 95 Percentage CI, 2.10 to 9.34) compared to low-dose aspirin monotherapy. The risk was not significantly increased when co-administered with statins (RR, 0.99; 95 Percentage CI, 0.81 to 1.21) or low-dose oral corticosteroids (RR, 1.01; 95 Percentage CI, 0.58 to 1.77) [54].
In the study of Weil et al., the risks of hospitalization due to peptic ulcer bleeding (gastric or duodenal) were determined against the background of prophylactic regimens with aspirin of 300 mg daily or less in 1121 patients. In 144 (12.8 Percentage) cases, regular use of aspirin (at least five days a week in the previous month) was found compared to 101 (9.0 Percentage) patients in the control hospitalized group and 77 (7.8 Percentage) community controls. The odds ratio was increased for all doses of aspirin taken, whether compared to hospital or municipal controls (compared to combined controls: 75 mg, 2.3 (95 Percentage CI 1.2 to 4.4), 150 mg, 3.2 (1.7 to 6.5), 300 mg 3.9 (2.5 to 6.3) Results are not affected by obscuring factors such as age, gender, previous ulcerative disease or dyspepsia or concomitant use of non-aspirin NSAIDs Researchers have not established a conventional prophylactic regimen of aspirin which is without risk of complications of the peptic ulcer [55].
On the other hand, the potential cardiovascular risk associated with the discontinuation of antiplatelet agents is ignored [56]. If the patient is on long-term antiplatelet therapy for primary or secondary cardiovascular prevention, a cardiovascular event may occur when antiplatelet agents are discontinued for several days. Most (60-70 Percentage) serious cardiovascular events occur within 10 days of antiplatelet discontinuation [57,58].
The use of antiplatelet agents in routine endoscopic procedures is based on an assessment of the risk of bleeding during endoscopy and the patient's thrombotic risk [57]. BSG and ESGE recommend that antiplatelet agents are continued in patients undergoing endoscopic procedures with a low risk of bleeding [25,26]. Aspirin can be continued with all endoscopic procedures, except for ESD, colon EMR over 2 cm, upper EMR, and pulpectomy. The risk of thrombosis versus the risk of bleeding should be assessed in these procedures for each patient [25]. In patients receiving dual antiplatelet therapy, only clopidogrel should be discontinued 5 days before high-risk endoscopic procedures when the risk of thrombosis is low. In case of high thrombotic risk, a consultation with a cardiologist is required [25,59]. When the thrombotic risk of stopping clopidogrel is high (30 days after coronary stent placement), the endoscopic procedure should be postponed. Clopidogrel can be resumed after the procedure when endoscopic hemostasis has been achieved [59].
The use of antithrombotic drugs is associated with an increased risk of bleeding from the GIT. In endoscopic interventions, it is necessary to balance the risk of bleeding and the thromboembolic risk in each patient. In addition to assessing the risk of bleeding, the endoscopist must be familiar with the criteria for assessing cardiovascular risk. In this area collaboration with a cardiologist is essential, especially in the manipulation of certain patients.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
