
Case Report | DOI: https://doi.org/10.31579/2578-8868/158
*Corresponding Author: K. Badache, Neurosurgery department of Ali Ait Idir Health Hospital Establishment, Algiers
Citation: Badache K., Shabhay Z., Yahiaoui M., Benmamar T., Boublata L., (2021) Management of The Posterior Cerebral Fossa Ependymomas. J. Neuroscience and Neurological Surgery. 8(3); DOI:10.31579/2578-8868/158
Copyright: © 2021 K. Badache, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 02 February 2021 | Accepted: 22 March 2021 | Published: 26 March 2021
Keywords: ependymoma; survival; resection; grade; outcome
Background
Posterior fossa brain ependymomas are one of the most devastating forms of human illnesses which are more common in children. Brainstem compression, herniation and death are the risks with tumours in this critical location.
Patients and Methods:
A retrospective study including 50 patients with posterior fossa ependymoma were performed at the Neurosurgery Department in Ait IDDIR University Hospital between the period of January 2005 and December 2015 . In each case, diagnosis was made clinically and confirmed radiologically and histo-pathologically.. All patients received the adjuvant treatment
Results
Out of 50 patients, 30 (60%) patients were males and 20 (40%) were females. The mean age was 24 years (ranged 5 months –47 years) ; we identified 29 (58%) children and 21 (42%) adults,. Ventriculo-peritoneal shunts were placed in all our patients, the total tumor excision was done to 35% and the partial tumor excision was done to 65% patients.
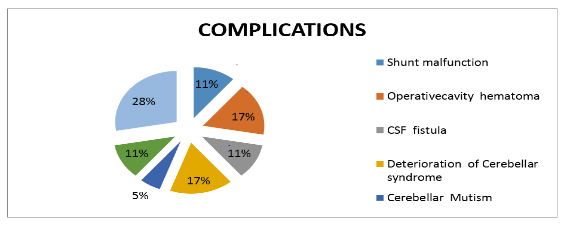
The most common complications were as follows: Shunt malfunction : 4% , operative cavity hematoma 6%, CSF fistula 4%, deterioration of Cerebellar syndrome 6%, Cerebellar Mutism 2%, Mixed nerves palsy 4% and early post operative deaths 10%.
Tumor architecture was classified as classic (Grade II) in 35 (70%) cases and anaplastic (Grade III) in 13(26%) cases.
Adjuvant treatment regimens following resection included radiation therapy only (72%) for 36 patients including children above and adults and chemotherapy only (36%) for 9 children below 4 years and 9 recurrent tumors.
During follow-up period, recurrence occurred in 27% 11patients out of 41patients .Five patients died (10%).
Conclusion
The surgical treatment of posterior fossa tumours still represents a challenge for neurosurgeons, Radical surgery with preservation of vital structures is the treatment of choice in patients with Posterior Cerebral Fossa ependymomas.. Our experience shows the accepted results, complications and surgical outcome in relation to previous clinical studies.
Ependymoma represents the third most common childhood malignancy of the brain, accounting for approximately 10% of all pediatric brain malignancies. [1] The most common site of presentation is the posterior fossa.[1] Standard therapy involves maximal safe resection, followed by radiation therapy (RT).[2]
A retrospective clinical cohort study of 50 patients with posterior fossa ependymoma were performed, and they underwent open surgical excision with ventriculo-peritoneal (V-P) shunt. All patients were admitted to the Neurosurgery department in Ait IDDIR University Hospital Algiers between a period of January 2005 and December 2015.
For all the patients, the diagnosis was made after surgery. All patients received the adjuvant treatment.
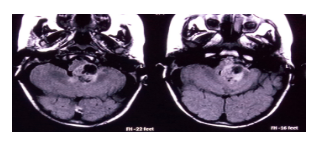
All patients underwent routine physical examination; they also received a thorough neurological evaluation. A special neuro-surgical sheet was applied in all cases included in the study to cover all suspects needed. CT as well as MRI, with and without contrast enhancement, was done for all cases before surgery as shown in (Figure 1)
Surgery was performed with general anaesthesia, in prone position, using an operating microscope and microsurgical instruments in all studied cases.
In our study, all patients were operated via a midline suboccipital approach. The objective of this surgery was to complete microsurgical excision of the tumour unless that tumour was invading the brain stem or attaching important vessels or nervous tissue.
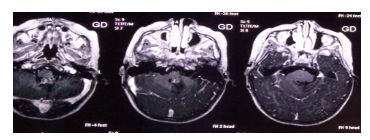
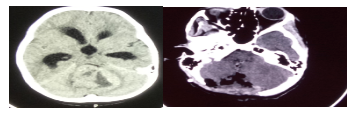
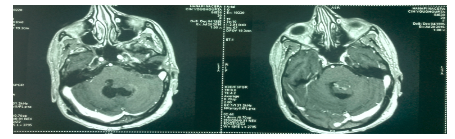
Early CT scan was performed to rule out early complications. Patients were followed clinically in our hospital then in outpatient neurosurgery clinic and also radiological through a period of 10 to 28 months. CT ± MRI with contrast was done at 3rd to 6th month of postoperative period then 1–2 years later. All intraoperative and postoperative complications were collected and reviewed, to detect any recurrence of the excised tumour (Figure 2-5).


Between January 2005 and December 2015, 50 patients with posterior fossa ependymoma were operated, 30 (60%) patients were males and 20 (40%) were females. The mean age was 24 years (ranged 5 months –47 years). A male and pediatric predominance were observed in our series.
Clinical manifestations of ependymoma vary widely according to the location.The most frequent clinical manifestations found were Intracranial hypertension syndrome (87%) and static and kinetic cerebellar syndrome (10%).
The imagery had shown that 92% of these tumors originated from the floor of the 4th ventricle and only 8% were extended to the cerebello-pontine angle cistern via foramen of Lushka and towards the cisterna magna via foramen of Magendie
For the Surgical outcome of this study : the Ventriculo-peritoneal shunts were placed in all our patients, the total tumor excision was done to 35% and the partial tumor excision was done to 65%patients.
In our study, the most common complications were as follows: Shunt malfunction : 4% (2 patients), operative cavity hematoma 3 cases (6%), CSF fistula 2 cases (4%), deterioration of Cerebellar syndrome 3 cases (6%), Cerebellar Mutism 1case ( 2%), Mixed nerves palsy2 cases (4%) and early post operative deaths 5 cases (10% )(Figure 6) .
According to tumour pathology, two patients (4%) had Grade I, thirty-five (70%) patients had Grade II (non-anaplastic) ependymoma and thirteen (26%) had Grade III (anaplastic) pathology.
Adjuvant treatment regimens following resection included radiation therapy only (72%) for 36 patients including children above and adults and chemotherapy only (36%) for 9 children below 4 years and 9 recurrent tumors. During follow-up period, recurrence occurred in 27% 11patients out of 41patients .Five patients died (10%). The decision to re-operate must always be discussed before All recurrent tumors were re-operated .Chemotherapy was often indicated after repeat surgery or in case of tumor inoperability.
According to the long term progress, the pourcentage of survival was as following :
at 5 years 29% (12 patients) and at 10 years 12% (7 patients).
According to an Australian study [1], the management of children operated of ependymoma of the posterior cerebral fossa is controversial. Radiotherapy should be delayed in children where tumor excision was total, on the contrary it is strongly indicated in those who underwent partial excision.
A European study [2] showed that the prognosis of PFC ependymomas depends on:
For the first time, WHO classification of CNS tumors has used molecular parameters and also histo-pathology to define the numerous tumoral entities [3]. This recent classification is based on the advances in molecular knowledge that guide therapeutic strategies to improve the prognosis.
According to Packer et all Children operated of Posterior Cerebral Fossa ependymomas , with total tumoral excision followed by chemotherapy and radiotherapy were completely cured. [4]
Radical surgery with preservation of vital structures is the treatment of choice in patients with Posterior Cerebral Fossa ependymomas. It must be followed by chemotherapy and/or radiotherapy if it is of higher histologic grade or after subtotal excision.
Progress has been achieved in the management and prognosis of these tumors, and is attributed to the high knowledge of the clinical and biological behaviour of these lesions.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
