
Case Report | DOI: https://doi.org/10.31579/JHV-2021/008
*Corresponding Author: Nwafor IA, NCTCE/Dept. of Surgery, UNTH, Ituku-Ozalla, Enugu Nigeria.
Citation: Nwafor IA., Onwura CC., Obi CC., Akanni BA, Gold I. and Eze JC. (2021) Management of Ruptured Pseudo-aneurysm of Right Common Carotid Artery in a low-income-Setting. J, Heart and Vasculature 1(1); DOI: 10.31579/JHV-2021/008
Copyright: © 2021, Nwafor IA, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 05 March 2021 | Accepted: 19 March 2021 | Published: 22 March 2021
Keywords: pseudo-aneurysm, innominate artery, endarterectomy, sternotomy
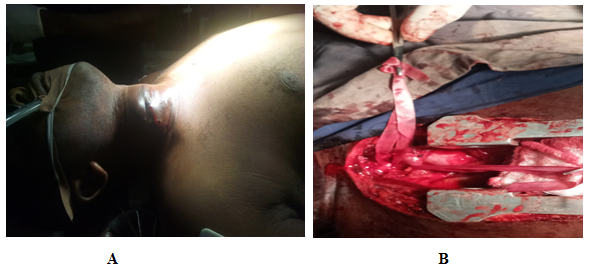
Carotid artery injuries with pseudo-aneurysm are uncommon but associated with central neurologic dysfunction. We present a giant bleeding pseudo-aneurysm of right common carotid artery managed by emergency sternotomy, neck exploration and repair of the aneurysm. A 26-year old man with machete cut to the right side of the neck presented with a progressive (R) sided neck swelling which started 6 weeks after the injury. In view of the progressive swelling, pain and continuous discharge of serosanguinous fluid from a sinus within the swelling, he was referred to our service, after having received 2 units of blood at the initial hospital. Clinical examination revealed a preserved man with intact vital signs, save for the pallor. On the right side of the neck was a 10 x 8 cm mass occupying almost the entire posterior triangle. It was pulsatile, tender with sinus discharging serosanguinous fluid. Positive thrill and bruit were demonstrable over the mass.
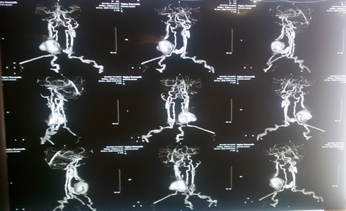
Conventional CTA and DSA showed a 1cm defect in the lateral wall of the distal RCCA, complete circle of Willis and massive blood clot at the site of the defect. He had emergency repair of the pseudo-aneurysm by way of median sternotomy and neck dissection, receiving 3 units of blood intra-operatively. Postoperative course was uneventful as he was managed with antibiotics, analgesics, haematinics, anticoagulants and physiotherapy.
Conclusion: In middle-and low-income settings where the technical know-how and resources for stenting including cerebral pulse oximeter are not available, expertise in open surgical approach becomes the only way to save life.
Aneurysm is defined as localized artery enlargement more than 150% of the segmental artery diameter [1, 2]. Extra-cranial carotid artery pseudo-aneurysms and true aneurysms are extremely rare, altogether accounting for only 0.4–4% of all peripheral artery aneurysms [3, 4]. Pseudo-aneurysm in particular has the propensity to enlarge and rupture (contained or uncontained, put compression on the surrounding structures like trachea, oesophagus, stellate ganglion, recurrent laryngeal nerve [5, 6]. Other complication that makes surgical treatment mandatory is the atheroembolism with associated cerebrovascular accident/stroke. According to Attigah and Malikov classification [7], the types 1 and 2 are very difficult to treat surgically, hence the need for multidisciplinary approach with neurosurgeons, neurophysician, otorlarngyogologist, maxillofacial surgeon, vascular surgeon and physiotherapist as well as radiologist and histopathologist. Open and endovascular or hybrid treatment approaches are recognized in the literature. Ultimately, the type of treatment will depend on mode of presentation, surgeon/interventionist experience, aneurysm location or accessibility and aetiology [8, 9].
The patient is O. K, a 26 year old tailor apprentice. He is a Christian of Roman Catholic denomination. He presented with progressive right sided neck swelling, 6 weeks prior.

He was cut in the right side of the neck with machete by a co-worker following a misunderstanding. There was profuse bleeding around the site. On raising alarm, he got assistance by some village security men who helped him put pressure at the site and took him to hospital. Wound was sutured to arrest haemostasis and he received 2 units of blood during resuscitation. Patient’s clinical condition remained uneventful. Swelling insidiously developed around the wound and progressively increased in size. With increase in size, a sinus developed within the wound and continued to discharge serosanguinous fluid few days prior to referral to our service. Our review noted the above findings. Patient was moderately pale. Hemoglobin was 8.9 gram%. In addition, a mass 10 x 8 cm, tender, pulsatile with bruit was found in the posterior triangle with scarification mark and a sinus discharging serosanguinous fluid. Conventional computerized tomographic scan and digital subtraction angiography showed a 1cm defect in the lateral wall of the distal right common carotid artery artery, complete circle of Willis and massive blood clot at the site of the defect. Patient t was worked up for emergency surgery.

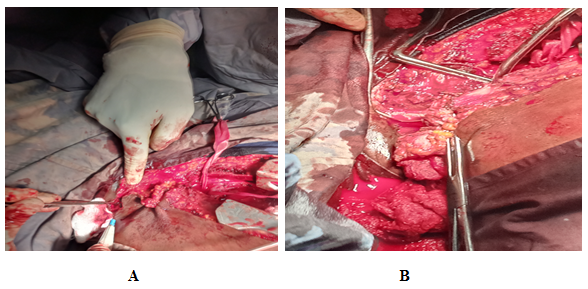
Proximal and distal control of right common carotid artery was done, bleeding defect isolated and controlled with digital pressure before closing with 5-0 prolene. Duration of right innominate artery clamping was 15 minutes and common carotid artery clamping was 10 minutes respectively. This is regarded as warm ischemic time. Patient was transfused 3 units of blood intra-operatively and estimated blood loss was about one liter. Wound was closed in layers with redivac drain in the neck and mediastinal drains in the chest. Analgesics, antibiotics, anticoagulants, heamatinics and physiotherapy were instituted postoperatively. His recovery was uneventful.

Trauma and prior carotid surgery such as endarterectomy are the most common causes of carotid artery pseudo-aneurysms. Other causes include atherosclerosis, vasculitis and collagen vascular diseases [10, 11]. The index case was caused by penetrating trauma. The location of the aneurysms was equally distributed between the internal and common carotid arteries. The external carotid aneurysm is usually inconsequential as it can be ligated with impunity. In the index case surgical repair was safe and effective with no significant morbidity or mortality and good midterm stroke prevention strategies. In the developed world, endovascular techniques with stent-graft exclusion have emerged as an efficient and safe alternative to open surgical resection [12]. . However, in low-income setting like ours, with absence of technical know- how and resources for endovascular intervention, expertise in open surgical approach becomes the only way to save life.
Historically, extra-cranial carotid aneurysm repair has undergone evolution from the time of Astley Cooper who performed the first ligation in 1805. Treatment strategies in open approach involve resection and reconstruction with end to end anastomosis, with interposition graft using autologous external artery conduit, saphenous vein or exogenous prostheses like expanded tetrafluoroethylene (ePTFE) or Dacron graft. Other methods are resection with intracranial and extra cranial bypass or outright ligation as a damage control measures in uncontained ruptured [8]. Our patient was treated by lateral tarsorraphy
Usually, a complete work up will help in determining the cause, location, morphologic features, evaluation of surrounding structures, vascular anatomic information and treatment planning. Ultrasonography, computerized tomographic scan and digital subtraction angiography are the main diagnostic tools in evaluating patients with pseudoaneurysms of common carotid artery of either side or both. These were deployed in the index case.
In the modern era, surgical repair of carotid artery injuries is associated with mortality rates of 0% to 22% and postoperative progression of neurologic deficit of 0% to 21% [10]. Endovascular approaches are increasingly used more frequently in carotid injuries. Stenting has most commonly been used for high extra cranial internal carotid lesions as pseudoaneurysms [12, 13]. Compared with surgical treatment of carotid injuries, with an associated mortality rate of up to 22%, carotid stenting appears to be much lower at 0.9% [11, 12, 13, and 14]. In addition, stroke rates associated with carotid stenting of trauma, at 3.5%, appear comparable to those after operative repair (0–21%) [11]. In the low-income setting, the technical know-how and resources for stenting are absent. Furthermore, the use of cerebral oximeter in the course of surgery is a cutting edge technology that is currently not available in the developing country like ours.
Though extra-cranial carotid aneurysm is rare, it usually presents a lot of challenges in its management, especially when it presents as emergency in the form of rupture, either contained or uncontained. Depending on the type, according to Attigah and malikove Classification, multidisciplinary team approach is very important in the management. Stenting and or hybrid procedures are not possible in the low-income setting like ours. This justifies emphasis on expertise on open approach.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
